Article Text

Abstract
BACKGROUND Sputum induction is a non-invasive procedure for measuring inflammatory processes of the lower respiratory tract. The aim of this study was to establish sputum cell counts and differentials in patients after lung transplantation (LTx), with or without chronic transplant rejection.
METHODS Sputum induction was performed in 41 LTx patients (25 single LTx (sLTx), 16 double LTx (dLTx) and 15 healthy non-smoking volunteers. Sputum was processed according to standard protocols. Total cell count was calculated as mean (SE) cells × 106/ml sputum and cell differential (%) was evaluated after staining. Cellular profiles were correlated with lung function.
RESULTS Total sputum cell counts were increased in sLTx (9 (1.9) cells × 106/ml, p=0.01) and dLTx patients (7.2 (1.5) × 106/ml, p=0.01) compared with healthy controls (2.6 (0.6) × 106/ml). There was also a marked sputum neutrophilia in both patient groups (59 (6)% and 62 (6)%, respectively, p<0.001v controls). Moreover, in both sLTx and dLTx patients with chronic transplant rejection there was an increased number of sputum neutrophils compared with patients with normal graft function (p<0.05 both comparisons), and neutrophils were inversely correlated with lung function (forced expiratory volume in one second (FEV1) % predicted): sLTx,r=–0.61, p=0.001; dLTx,r=–0.75, p=0.001, respectively). Sputum lymphocytes and eosinophils were similar in both groups. No relevant side effects occurred during sputum induction.
CONCLUSIONS Sputum induction is a safe and non-invasive tool for monitoring lower respiratory tract inflammation in LTx patients. Both sLTx and dLTx patients with chronic rejection had increased sputum neutrophils compared with patients with normal transplant function. These data support findings of other authors highlighting a possible role for neutrophils in the pathogenesis of chronic transplant rejection.
- lung transplantation
- sputum
- rejection
Statistics from Altmetric.com
Lung transplantation (LTx) has become a therapeutic option for a growing number of patients with end stage lung disease—for example, idiopathic pulmonary fibrosis (IPF), cystic fibrosis (CF), chronic obstructive pulmonary disease (COPD), or pulmonary hypertension.1 However, despite recent improvements in surgical procedures and post-transplant immunosuppression, overall prognosis after lung transplantation is limited with a 2 year survival rate of 70–80% and a 5 year survival of only 50–60%.2-4 Besides pulmonary infection, chronic transplant failure due to rejection is the major cause of transplant associated morbidity and mortality.5 ,6 Chronic transplant rejection is characterised by a progressive decline in pulmonary function associated with inflammatory processes leading to tissue damage and fibrosis, predominantly in the small airways.7Chronic rejection is often referred to as “bronchiolitis obliterans syndrome” (BOS), although knowledge of the pathogenesis of BOS is limited. Most evidence suggests a combined role of host immune responses to the allograft and pulmonary infection, especially cytomegalovirus (CMV) infection, as major trigger factors for BOS.7
Transbronchial biopsy is the gold standard for detecting histological changes in allografts consistent with BOS.8 However, transbronchial biopsies carry some potential risks such as alveolar bleeding or pneumothorax. Other diagnostic tools such as high resolution computed tomography (HRCT) or spirometry are therefore used to monitor transplant function, and diagnosis of BOS is based on clinical criteria as proposed by the International Society of Heart and Lung Transplantation.8 Despite this, there is an emerging need for non-invasive procedures to evaluate lower respiratory tract inflammation in LTx patients.
Sputum induction has been extensively used to characterise inflammatory processes in patients with asthma or COPD.9 ,10 It provides a reliable and safe non-invasive tool for studying cellular and soluble components of the lower respiratory tract which may be applied to a variety of pulmonary disorders. Until now the potential value of sputum induction in patients with LTx has not been assessed. Thus, the aim of this cross sectional study was to evaluate sputum cell counts and differentials in LTx patients, and to determine whether chronic rejection is accompanied by an alteration in the pattern of the cellular components in the respiratory tract which may also be correlated with lung function in these patients.
Methods
PATIENTS
The study population consisted of 41 LTx patients (76% men) of mean age 49 years (range 18–64 years. The underlying diseases were pulmonary emphysema (n=19), IPF (n=13), cystic fibrosis (n=6), and others (n=3). Twenty five patients had undergone single lung transplantation (sLTx) and 15 patients had undergone double lung transplantation (dLTx). One patient with cystic fibrosis had received a single re-transplant after initial dLTx. Immunosuppressive regimens following transplantation were either a combination of azathioprine/cyclosporin A (CsA, n=24), mycophenolate/CsA (n=10), or mycophenolate/tacrolimus (FK506, n=7), together with low dose corticosteroids (10–20 mg/day).
Fifteen healthy, non-smoking adults (60% men) of mean age 30 years (range 20–38) without a history of atopy or respiratory disorders served as controls. The study was approved by the local ethics committee and all patients were informed of the purpose of the study and gave informed written consent.
CLINICAL EVALUATION AND EXCLUSION OF ACTIVE INFECTION
Patients with LTx were clinically evaluated on presentation to the outpatient transplant clinic or during hospital stays for routine procedures. Standard procedures included chest radiography and spirometric tests (Jaeger, Masterlab II, Wuerzburg, Germany). Spirometric measurements included forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) manoeuvres.
To minimise the possibility of airway infection, only patients without clinical signs of active infection such as fever or malaise were included. Furthermore, chest radiographs, leucocyte count, and serum C reactive protein (CRP) levels had to be normal or unchanged. Sputum samples were also cultured to detect microbiological organisms and the results had to be negative or considered as low grade colonisation only if positive.
A diagnosis of chronic rejection was either based on histological findings in the bronchial biopsy specimens or clinical criteria of a progressive decline in lung function or gas exchange over time, a consistent chest radiograph or HRCT scan, or a combination of these, as proposed by the consensus report of the International Society of Heart and Lung Transplantation.8
SPUTUM INDUCTION
Sputum induction was performed according to a method previously described9 with slight modifications. Patients inhaled 4% hypertonic saline delivered by an ultrasonic nebuliser device (UltraNeb 2000, DeVilbiss, UK) for 15 minutes. They were then told to rinse their mouth, blow their nose, and carefully cough sputum into a petri dish using forced expiratory manoeuvres. If the induction was well tolerated, the first portion of sputum was discarded and the inhalation procedure was repeated for another 15 minutes. Lung function was carefully monitored by spirometric tests every 5 minutes during induction to ascertain safety of the procedure. Induction was stopped when a fall in FEV1 of >20% occurred and patients were given two puffs of salbutamol (100 μg/puff).
SPUTUM PROCESSING AND COUNTING
Sputum plugs were carefully separated from salivary secretions and examined by light microscopy to ascertain the least possible contamination of sputum with saliva and squamous cells. An appropriate sample was then filled into a 1 ml Eppendorf cup, weighed, and mixed with twice the volume of dithiotreitol (DTT 0.1%, Calbiochem, Germany). The sputum was gently vortexed and placed into a water bath at 37°C for 15 minutes to allow homogenisation of the sample, with repeated mixing. Phosphate buffered saline (PBS, Gibco Life, UK) was added to achieve a 20-fold dilution and the samples were centrifuged at 400g for 10 minutes. The supernatant was discarded and the cell pellet was resuspended in 200–400 μl PBS with 1% bovine serum albumin (BSA, Sigma Chemicals, Germany). 20 μl of cell suspension was added to 5 μl trypan blue, vortexed, and 10 μl of the solution was then counted in a Neubauer cell chamber. Viable cells were counted and the total cell count was calculated as cell count/ml sputum. For cytospins, an adequate sample of the cell suspension was added to a cytospin tube to achieve a total number of 20 000–30 000 cells per slide, spun for 5 minutes, fixed and stained with Hemacolor staining (Merck, Germany) to allow differentiation of squamous cells, macrophages, neutrophils, eosinophils, and lymphocytes. Cytospin quality was regarded adequate when contamination with squamous cells was less than 20%. A total of 400 non-squamous cells were then independently counted by two blinded observers. The relative proportion of cell types was counted as the percentage of all non-squamous cells.
STATISTICAL ANALYSIS
Statistical analysis was performed using the stata 5.0 intercooled software package (Stata Corp, Texas, USA) for personal computer. Unless otherwise stated, data are given as mean (SE) values or median for time after transplantation. The Kolmogorov-Smirnov test was used to test variables for normal distribution. Differences between groups were measured using the Mann-Whitney U test for non-normally distributed values and the Student'st test for normally distributed values. Unless otherwise stated, patients undergoing sLTx and dLTx were analysed separately. Correlational analysis was performed by simple linear regression. Since the total sputum cell counts were log normally distributed, log values were used for correlational analysis. A p value of less than 0.05 was considered statistically significant.
Results
Twenty one patients undergoing lung transplantation met the clinical criteria of chronic transplant rejection while the other 20 had apparently normal graft function (12/25 sLTx, 9/16 dLTx). The time elapsed after transplantation was higher in patients with chronic rejection than in those without (median 732v 241 days after transplantation, p=0.02). Sputum cultures were positive for Pseudomonas cepacia in two patients with underlying cystic fibrosis and forStaphylococcus aureus in another two patients with pulmonary emphysema. One patient who underwent sLTx for α1-antitrypsin deficiency was sputum positive forAspergillus fumigatus.
Serum CRP levels were similar in both sLTx and dLTx patients with or without chronic rejection. Absolute and relative values of FEV1 and the ratio of FEV1/FVC were significantly lower in patients with chronic rejection.
SAFETY
Sputum induction was safe and well tolerated by all patients. No significant fall in FEV1 (>20% change from baseline) was observed in any patient. The mean change in FEV1 after induction was –37 (41) ml. Single minor complaints were not clinically significant and included sensory dysfunction (n=1) and dry cough (n=1), both of which were temporary and reversed spontaneously within a few hours after the procedure. During a 4 week follow up period none of the patients developed respiratory tract infection.
SPUTUM CELLS
Compared with healthy controls, LTx patients in general had significantly higher total cell counts and percentage of neutrophils while the relative proportion of macrophages was reduced. No differences were observed between sputum lymphocyte or eosinophil counts (table 1).
Mean (SE) sputum cell counts of healthy controls and patients undergoing lung transplantation
In both sLTx and dLTx patients, those with established chronic rejection had higher sputum neutrophil counts than patients with normal transplant function. Total cell counts were also increased in patients with chronic rejection, although this observation only reached statistical significance in sLTx patients. No differences were seen in the lymphocyte and eosinophil differential counts in any of the subgroups (table 2).
Mean (SE) sputum cell counts of lung transplantation patients with or without chronic rejection
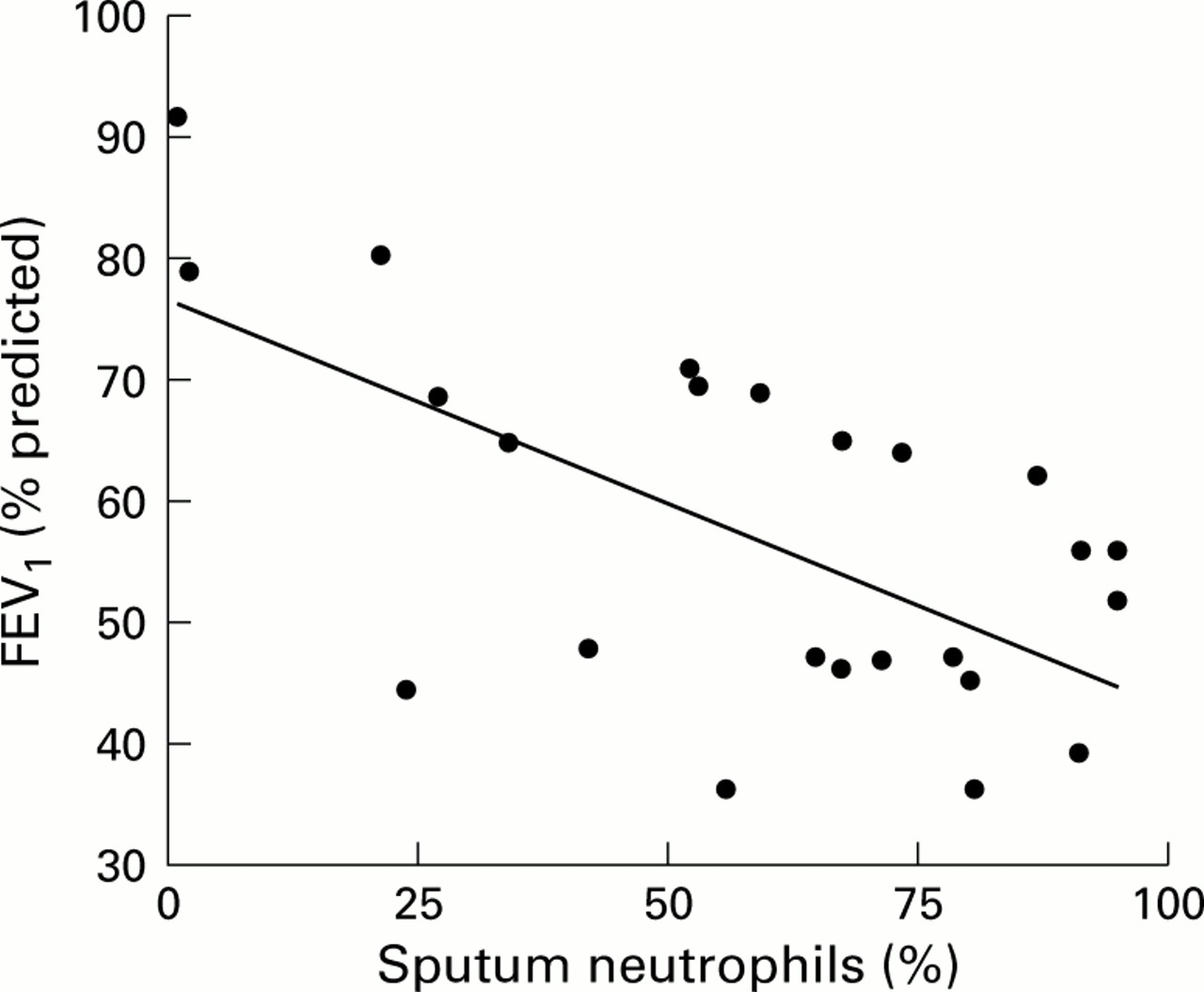
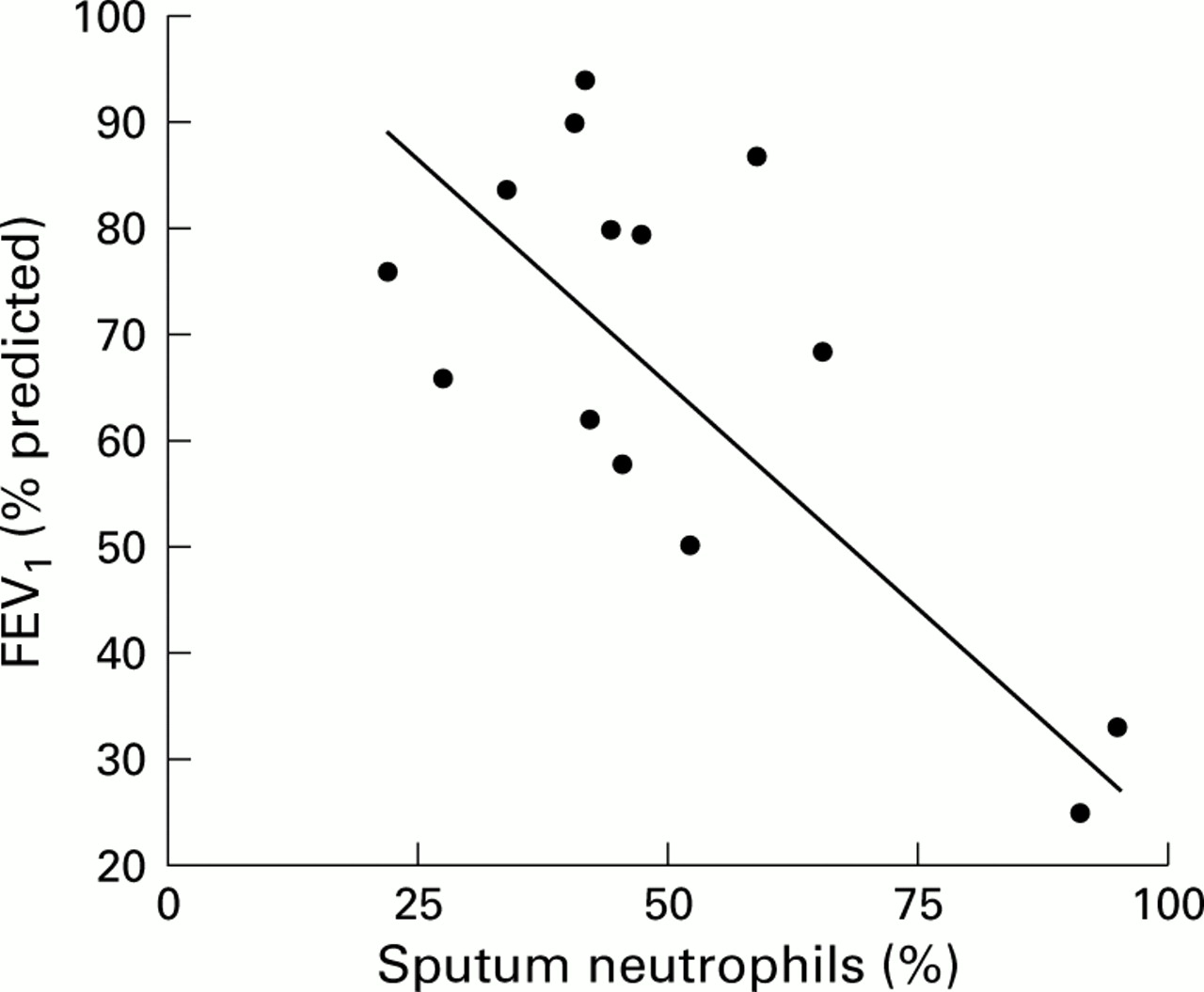
Log total sputum cell counts and the proportion of sputum neutrophils were also inversely correlated with % predicted FEV1values. This observation was true for both sLTx (log total cells:r=–0.35, p=0.07, fig 1) and dLTx patients (log total cells: r=–0.5, p=0.04, fig2).

Correlation of sputum neutrophils and lung function (FEV1 % predicted) in 25 patients undergoing single lung transplantation (r=–0.61; p=0.001).

{kind=link}
{kind=link}
Correlation of sputum neutrophils and lung function (FEV1 % predicted) in 16 patients undergoing double lung transplantation (r=–0.75; p=0.001).
Discussion
Chronic transplant rejection is the major cause limiting the overall prognosis of patients after lung transplantation. Since standard techniques to monitor rejection are often invasive and may therefore bear a significant risk for the patients, there is a need for non-invasive procedures to monitor lower respiratory tract inflammation in LTx patients. This study was performed to evaluate the role of sputum induction in lung transplantation.
Sputum induction was safe and well tolerated by all LTx patients and healthy volunteers. No significant fall in FEV1 was observed in any patient, and minor complaints were negligible. Despite this, because of the underlying immunosuppression in these highly susceptible individuals, hygiene precautions should be undertaken to avoid contamination of the nebuliser, valves, or tubes, and sterile disposable equipment should be used.
Since patients have different lung diseases after sLTx and dLTx, with the native lung remaining in situ in sLTx patients, these two groups were analysed separately. Compared with healthy volunteers, both groups of patients had significantly increased total sputum cell counts and a higher proportion of sputum neutrophils. This observation was independent of established chronic rejection. The general increase in cell count and neutrophils may be due, at least in part, to treatment with oral corticosteroids which have the potential to increase blood and tissue neutrophils.11 However, total cells and neutrophils in both transplantation groups were increased even more in those patients with chronic rejection, despite the fact that there was no difference in corticosteroid therapy between these groups. Moreover, a significant correlation of total sputum cell counts and sputum neutrophils with the severity of airflow obstruction was observed in both groups of patients.
With regard to sputum neutrophilia, lower respiratory tract infection was assumed to be a major confounding factor affecting the interpretation of the observed cellular profiles in the population under survey. We have therefore carefully evaluated the patients to minimise the possibility of underlying infection. Only patients with no clinical abnormalities, leucocytosis, and increased serum CRP levels were studied. Apart from the five patients discussed earlier, sputum cultures revealed no bacterial or fungal growth in any sample and the organisms grown were considered to represent colonisation rather than infection. Moreover, these patients did not have the lowest FEV1 values, hence inclusion in the analysis did not bias the basic results of our study.
In contrast to bronchoalveolar lavage samples, the assessment of induced sputum cells in single lung transplant recipients is problematic because it cannot be ascertained clearly whether the sputum sample derives from the transplanted allograft or the residual lung. It is therefore possible that the underlying pathology in the native lung contributes to the sputum neutrophilia, especially since the sLTx patients in this cross sectional analysis predominantly had IPF or COPD, both of which are associated with accumulation of neutrophils in the lower respiratory tract.12 ,13 Nevertheless, even in these patients we found a clear negative correlation between sputum neutrophilia and severity of airflow limitation.
It therefore appears likely that sputum neutrophilia reflects an underlying inflammatory process involved in the pathogenesis of chronic rejection, promoting inflammation, tissue damage, and airway wall remodelling. These findings are in agreement with bronchoalveolar lavage and biopsy studies which have consistently reported a marked neutrophilia in lavage fluid14-17 or lung tissue18 ,19 during chronic rejection.
We conclude that sputum induction provides a safe non-invasive tool for measuring airway inflammation in LTx patients. Further studies will evaluate the sensitivity of serial sputum induction and the predictive value for chronic rejection in LTx patients. Further elucidation of the possible contribution of neutrophils to chronic rejection is also necessary, since novel anti-inflammatory drugs targeting neutrophils, such as leukotriene B4 antagonists20 or selective phosphodiesterase inhibitors,21 may offer potential therapeutic benefit in this condition.