Article Text

Abstract
BACKGROUND In vitro the long acting β2 agonist salmeterol can, in contrast to formoterol, behave as a partial agonist and become a partial antagonist to other β2 agonists. To study this in vivo, the bronchodilating effect of salbutamol was measured during methacholine induced moderate to severe bronchoconstriction in patients receiving maintenance treatment with high dose long acting β2agonists.
METHODS A randomised double blind crossover study was performed in 19 asthmatic patients with mean forced expiratory volume in one second (FEV1) of 88.4% predicted and median concentration of methacholine provoking a fall in FEV1 of 20% or more (PC20) of 0.62 mg/ml at entry. One hour after the last dose of 2 weeks of treatment with formoterol (24 μg twice daily by Turbuhaler), salmeterol (100 μg twice daily by Diskhaler), or placebo a methacholine provocation test was performed and continued until there was at least a 30% decrease in FEV1. Salbutamol (50 μg) was administered immediately thereafter, followed by ipratropium bromide (40 μg) after a further 30 minutes. Lung function was monitored for 1 hour after provocation.
RESULTS There was a significant bronchodilating and bronchoprotective effect after 2 weeks of active treatment. The dose of methacholine needed to provoke a fall in FEV1 of ⩾30% was higher after pretreatment with formoterol (2.48 mg) than with salmeterol (1.58 mg) or placebo (0.74 mg). The difference between formoterol and salmeterol was statistically significant: 0.7 doubling dose steps (95% CI 0.1 to 1.2, p=0.016). The immediate bronchodilating effect of subsequently administered salbutamol was significantly impaired after pretreatment with both drugs (p<0.0003 for both). Three minutes after inhaling salbutamol the increase in FEV1 relative to the pre-methacholine baseline was 15.8%, 7.3%, and 5.5% for placebo, formoterol and salmeterol, respectively (equivalent to increases of 26%, 14%, and 12%, respectively, from the lowest FEV1after methacholine). At 30 minutes significant differences remained, but 1 hour after completing the methacholine challenge FEV1had returned to baseline values in all three treatment groups.
CONCLUSION Formoterol has a greater intrinsic activity than salmeterol as a bronchoprotective agent, indicating that salmeterol is a partial agonist compared with formoterol in contracted human airways in vivo. Irrespective of this, prior long term treatment with both long acting β2agonists reduced the bronchodilating effect of an additional single dose of salbutamol equally, indicating that the development of tolerance or high receptor occupancy overshadowed any possible partial antagonistic activity of salmeterol. Patients on regular treatment with long acting β2 agonists should be made aware that an additional single dose of a short acting β2 agonist may become less effective.
- formoterol
- salmeterol
- salbutamol
- asthma
- tolerance
Statistics from Altmetric.com
Inhaled β2 agonists are extensively used in the treatment of asthma due to their excellent bronchodilating and bronchoprotective effects.1-3 As the duration of action of the two newest β2 agonists, salmeterol and formoterol, is longer than of the older β2 agonists, they are classified as long acting β2 agonists. Both salmeterol and formoterol have an established position in the maintenance treatment of moderate to severe asthma, with short acting β2 agonists being used additionally “as needed”.3
Salmeterol and formoterol differ pharmacologically in that formoterol has a much faster onset of action than salmeterol4-6 and, in vitro, salmeterol is a partial agonist on the β2receptor while formoterol is virtually a full agonist.7 ,8During strong cholinergic broncochoconstriction, salmeterol has been shown to behave as an antagonist towards subsequently administered β2 agonists.7 ,8 In vivo, such cholinergic bronchoconstriction may exist during an acute asthma attack.
Many studies have focused on tachyphylaxis and tolerance during treatment with β2 agonists.9-18 This phenomenon appears to have a stronger effect after continued treatment of the β2 agonist than after a single dose.
In this study we have investigated whether formoterol and salmeterol, given in high doses, behave as antagonists to subsequently given salbutamol. The effect of β2 agonist induced reversal of methacholine induced bronchoconstriction (inducing a fall in FEV1 of at least 30% from baseline) was used as a model.4 The assumption was that, after strong cholinergic stimulation, a difference in the ability of salbutamol to reverse the bronchoconstriction may develop depending on the type of additional β2 agonist pretreatment, creating an in vivo analogy of the in vitro study by Molimard et al.8 In contrast to Molimard's model which used single dose administration, high dose maintenance treatment with the two long acting β2 agonists was applied which has more relevance to the clinical situation.
Methods
PATIENTS
Patients diagnosed as having asthma according to the American Thoracic Society guidelines were invited to participate in the study.1 The inclusion criteria included age 18–45 years; forced expiratory volume in one second (FEV1) >1.5 l and >60% predicted19; concentration of methacholine causing a decrease in FEV1 of 20% (PC20) 4 mg/ml maximum; and decrease in FEV1 of at least 30% during methacholine provocation. Exclusion criteria included concomitant diseases or conditions that might affect the study; use of long acting β2 agonists, oral antihistamines, or oral bronchodilators for 24 hours before the enrolment visit until completion of the study; change in dose of inhaled corticosteroids or use of oral steroids in the 6 weeks before the study; and pregnancy. All patients had mild to moderate asthma with obvious bronchial hyperresponsiveness and were being treated with an inhaled glucocorticosteroid (continued unchanged during the study) and a bronchodilator on an “as needed” basis (replaced with ipratropium bromide during the study).
The study was approved by the medical ethics committee of the Martini Hospital, Groningen, the Netherlands and was conducted according to Good Clinical Practice Guidelines. Written informed consent was obtained from all patients prior to enrolment.
STUDY DESIGN
This double blind, randomised, crossover study used a double dummy technique for administering study drugs. The enrolment visit and each of the three test days were separated by three treatment periods of 2 weeks.
Inhalers with formoterol (blinded Oxis Turbuhaler, 12 μg formoterol fumarate per metered dose mixed with lactose, equivalent to 9 μg delivered dose), salmeterol (blinded Serevent Diskhaler, 50 μg salmeterol xinafoate per dose mixed with lactose), and placebo (lactose) were provided by AstraZeneca R&D Lund. Two doses from each of two inhalers were administered twice daily over 2 weeks, starting in the evening after a visit day and using the last dose on the morning of the clinic visit, after measuring FEV1. The daily dosages were thus 48 μg formoterol and 200 μg salmeterol. The 1:4 relationship has previously been reported to result in approximately equal bronchodilation; the high dose was applied to ensure maximal bronchodilation.6 Ipratropium bromide was allowed as rescue medication (40 μg Atrovent capsules administered via Inhalator Ingelheim, Boehringer Ingelheim, the Netherlands). No washout period was deemed necessary since it was expected that a new steady state situation would be attained within 1 week.9 Before each visit the patients had not taken inhaled ipratropium bromide, inhaled glucocorticosteroids, or cromoglycate in the previous 6 hours, nor caffeine containing beverages in the previous 2 hours. They also refrained from exercise before the tests.
A test day was postponed if morning FEV1 was below 80% or above 120% of the baseline FEV1 at enrolment. In the morning of the three test days pre-dose lung function was measured, followed by the last dose of study medication. One hour later lung function was again measured—referred to hereafter as the post-dose and “baseline” lung function—and the methacholine provocation test started. The provocation tests were scheduled within 1 hour of the time at which they were performed during the enrolment visit. The same technician performed all tests. At the initial visit the patients practised their inhalation technique with empty inhalers in accordance with the manufacturers' instructions. At the screening visit and 1 hour after the morning dose on the three test days a standard methacholine provocation test was performed and continued until a reduction of at least 30% in FEV1 was achieved.4 The challenges were performed using a Wiesbadener Doppelinhalator giving an output of 0.2 ml in 2 minutes. After saline, doubling concentrations of methacholine bromide from 0.125 mg/ml to 64 mg/ml dissolved in saline were inhaled at 5 minute intervals during 2 minutes of tidal breathing. FEV1 was measured with a dry spirometer (Schiller SP-100, Schiller, Baar, Switzerland) which was calibrated daily. Pre-dose and post-dose (baseline) FEV1 were measured in triplicate and the highest FEV1 values were used in the analyses. The baseline FEV1 (after the study drug but before saline) was taken as the reference value for the calculation of changes in FEV1. Single FEV1 assessments were made 30 and 90 seconds after completing each 2 minute nebulisation and the lowest value was used for the analyses. The methacholine provocation test was stopped when FEV1 decreased by 30% or more compared with baseline. One dose of salbutamol (50 μg via Turbuhaler, Astra Draco, Lund, Sweden) was inhaled within 1 minute of reaching a decrease in FEV1of >30%. Single assessments of FEV1 were made at 1, 3, 5, 10, 15, 20, 25 and 30 minutes after inhaling salbutamol (0 min). A single dose of ipratropium bromide (40 μg) was then inhaled and lung function was assessed in triplicate after a further 30 minutes. If dyspnoea became too severe, either during or within 60 minutes of the provocation test, as judged by the patient or the technician, a bronchodilator was administered and the test halted and an inhaled bronchodilator was then administered freely. This test was repeated on another day.
Compliance was assessed by counting either the number of used and unused Diskhaler doses returned or the number of remaining clicks in the Turbuhaler. Adverse events were recorded at the start of each test day.
DATA ANALYSIS
The primary parameter in the statistical analysis was the increase in FEV1 from 0 to 3 minutes after inhaling salbutamol, expressed as % of the baseline value (post-dose FEV1). Secondary parameters (FEV1 at 30 and at 60 minutes, PC20 methacholine, PD30+ methacholine, and the recovery time) were statistically analysed to a limited extent to prevent false positive conclusions. The PC20 was calculated by linear interpolation of the log methacholine concentration (non-cumulative) versus the percentage fall in FEV1 from baseline. The cumulative methacholine dose administered to induce the PD30 was calculated from the nebuliser output, arbitrarily assuming that all methacholine nebulised during 2 minutes penetrated into the lungs. The recovery time was calculated from the data points immediately before and after FEV1 returned to 85% of baseline by linear interpolation. In cases where FEV1 did not return to 85% of baseline within 60 minutes, an arbitrary time of 75 minutes was used in the analyses. For the statistical analysis of PC20, PD30+ and the recovery time a log transformation was made. If the lowest methacholine dose caused a decrease in FEV1 of 20% or more, PC20 was arbitrarily set at half the lowest concentration—that is, 0.0625 mg/ml.
Analysis of covariance (ANCOVA) was used to determine treatment differences with patient, period, and treatment as factors. The observed maximal percentage decreases in FEV1 and PD30+ were used as covariates since both the magnitude of the fall in FEV1 and the methacholine dose could be expected to have an influence on the recovery of FEV1 at 3 minutes and the recovery time. When a covariate was not statistically significant it was excluded from the analyses. A two sided p value of <0.05 was considered significant. When treatment was statistically significant, 95% confidence intervals (95% CI) were calculated from the least squares means. Differences in PC20 and PD30+ between treatments are expressed as doubling dose steps, originating from analyses from base-2 log transformed data.
It was estimated that 20 enrolled subjects were needed to give at least 15 subjects who could be fully evaluated. The effect at 3 minutes was considered to be the primary parameter in the analysis. A power calculation, using the results of a previous study,4indicated that a difference of 4% could be detected in the increase in FEV1 after 3 minutes with a significance level of 5% and a power of 80%.
Results
Nineteen patients were enrolled in the study and randomised. Four patients were withdrawn because of concurrent airway infections; all four were comparable to the other 15 patients in baseline lung function and PC20 methacholine. The provocation tests were well tolerated and there was no need for an additional bronchodilator. Table1 shows the patient characteristics; the patients can be regarded as having mild to moderate asthma but with pronounced bronchial hyperresponsiveness.
Characteristics of patients
The absolute FEV1 values on test days are shown in table 2and the percentage predicted FEV1 during the entire test day is shown in fig 1. At the start of the test day, approximately 12 hours after inhaling the previous evening dose, pre-dose FEV1 values in the formoterol and salmeterol periods were 0.15 l and 0.12 l higher, respectively, than in the placebo period. One hour after the morning dose the differences were 0.32 l and 0.26 l (approximately 10%, statistical significance not tested). Compared with placebo, more methacholine had to be administered following active treatment before FEV1 decreased by 20% and by ⩾30% from baseline. The PC20 values after formoterol and salmeterol administration differed by 1.5 doubling dose steps (95% CI 0.8 to 2.1) and 1.0 doubling dose step (95% CI 0.3 to 1.7), respectively, both differences being statistically significant. The values between active treatments did not differ significantly (0.5 doubling dose steps, 95% CI –0.2 to 1.1). PD30+ differed in a similar way; geometric mean PD30+ was 2.48 mg after formoterol treatment, 1.58 mg after salmeterol pretreatment, and 0.74 mg after placebo pretreatment (fig 2). The difference in PD30+ of 0.7 doubling dose steps between the two active treatments was statistically significant (95% CI 0.1 to 1.2, p=0.016).
Mean (SD) forced expiratory volume in one second (FEV1) in litres on the three test days before and after the morning dose, at reaching a methacholine induced decrease in FEV1 of ⩾30%, at 3 and 30 minutes after salbutamol inhalation, and at 30 minutes after additional ipratropium bromide inhalation

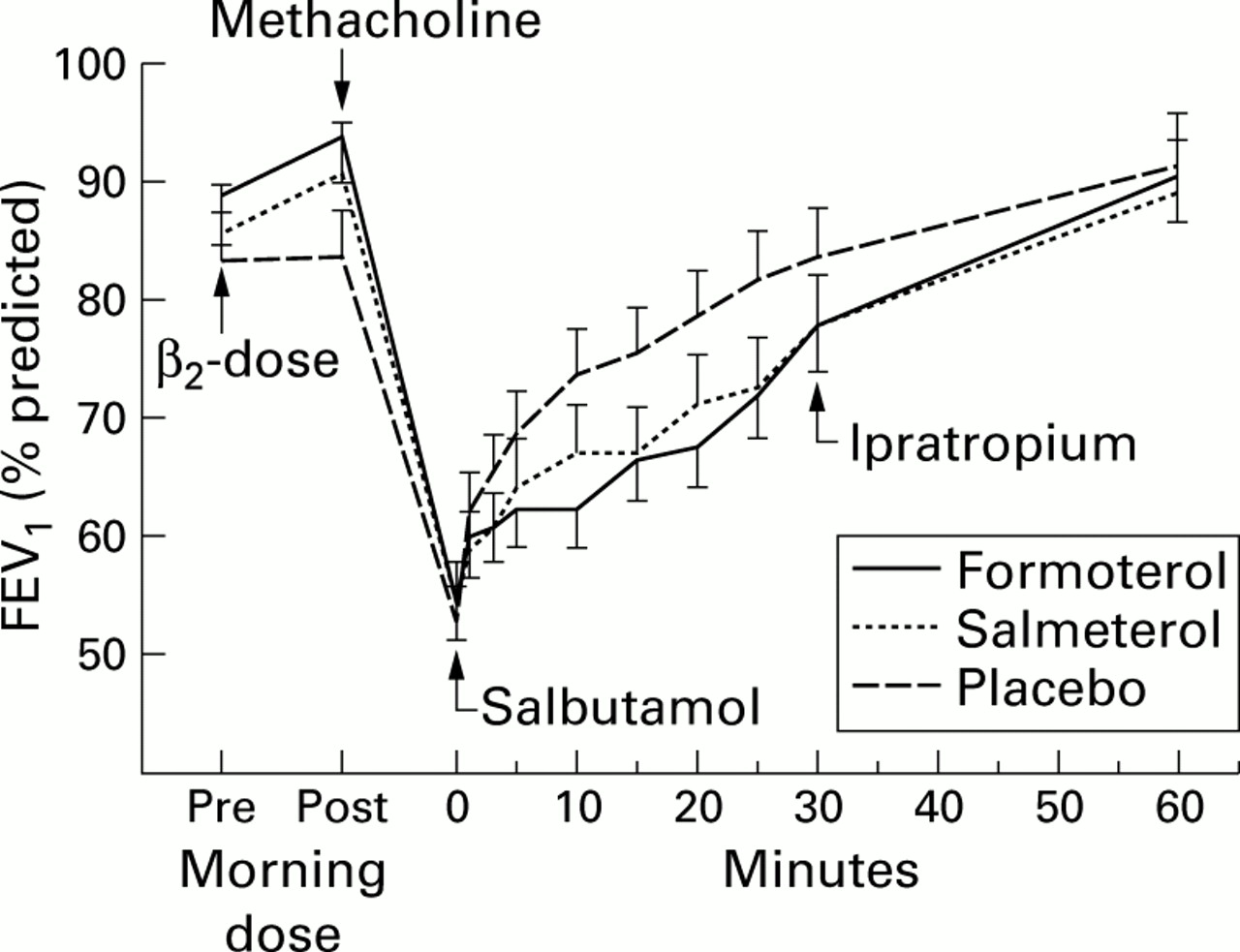
Mean (SE) percentage predicted forced expiratory volume in one second (FEV1) before and one hour after the morning dose, at reaching a methacholine induced decrease in FEV1 of ⩾30%, during 30 minutes following inhalation of 50 μg salbutamol, and after an additional 30 minutes following inhalation of 40 μg ipratropium bromide. Pretreatment for 2 weeks with formoterol 24 μg twice daily via Turbuhaler, salmeterol 100 μg twice daily via Diskhaler, or placebo twice daily.

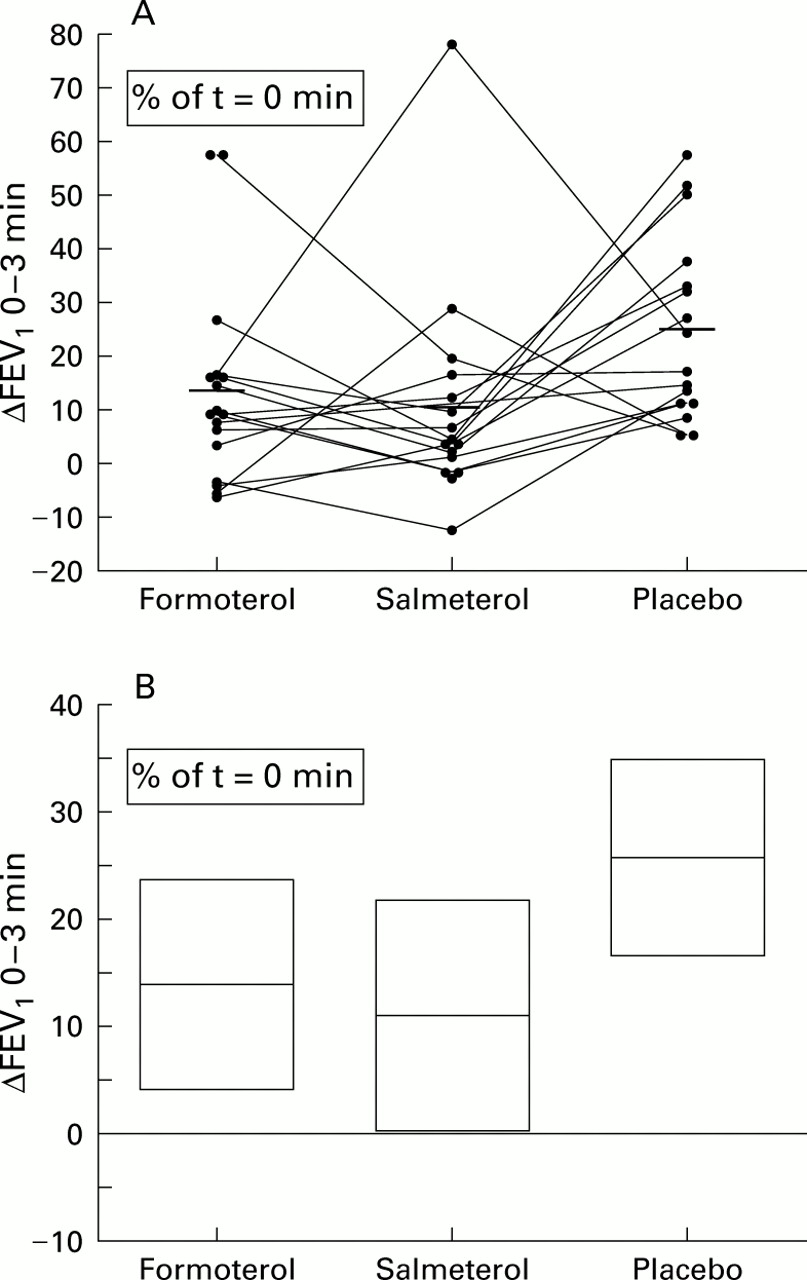
Methacholine dose needed to prevoke a fall in FEV1 of ⩾30% (PD30+) measured about one hour after the last dose of treatment for 14 days with either formoterol 24 μg twice daily via Turbuhaler, salmeterol 100 μg twice daily via Diskhaler, or placebo. Log transformed data. (A) Individual data (horizontal lines represent mean values); (B) mean values with 95% confidence intervals.
Apart from the difference in methacholine dose, the provocation tests on the three test days were comparable with a mean overall decrease in FEV1 of 39.3% from baseline (ranging from 29.8% to 61.3% on individual days).
Three minutes after inhaling salbutamol FEV1increased by a mean (SD) of 15.8 (9.7)% of the baseline (pre-challenge) value after pretreatment with placebo compared with 7.3 (8.4)% after pretreatment with formoterol and 5.5 (8.9)% after pretreatment with salmeterol (p=0.0003 for both treatments, ANCOVA). The covariate actual % decrease in FEV1 was statistically significant (p=0.014) whereas the covariate PD30+ was not (p=0.12). The difference in FEV1 between pretreatment with placebo and with active drug was 11.9% (95% CI 6.1 to 17.7) for formoterol and 11.3% (95% CI 5.7 to 16.9) for salmeterol (both p=0.0003). The difference between the two active pretreatments was not significant (95% CI –6.2 to 5.0, p=0.82). In a post hoc analysis comparing only the two active treatments and taking PD30+as covariate, the difference between the two long acting β2 agonists remained not significant, nor was the covariate significant. The percentage increase in FEV1 from the lowest FEV1 after methacholine was 14 (19)%, 12 (21)%, and 26 (17)% after pretreatment with formoterol, salmeterol, and placebo, respectively (fig 3). Thirty minutes after inhaling salbutamol the increase in FEV1 was still significantly smaller after both active pretreatments than after placebo (p=0.0001, ANCOVA), with again no significant difference between the two active treatments. Following all three pretreatments the mean FEV1 returned to the same value within 30 minutes after the inhalation of ipratropium bromide. The recovery time is shown in table3. After pretreatment with both long acting β2 agonists recovery was significantly slower than after placebo pretreatment (p=0.0001), but the difference between formoterol and salmeterol was not significant (p=0.55). Geometric mean recovery times were 35, 28, and 7 minutes after formoterol, salmeterol and placebo, respectively.
{kind=link}
{kind=link}
{kind=link}
Increase in FEV1 three minutes after inhalation of 50 μg salbutamol via Turbuhaler as percentage of the lowest FEV1. Salbutamol was inhaled immediately after reaching a methacholine induced decrease in FEV1 of ⩾30% about one hour after the last dose of either formoterol 24 μg twice daily via Turbuhaler, salmeterol 100 μg twice daily via Diskhaler, or placebo via both devices for 2 weeks. (A) Individual values; (B) mean values and 95% confidence intervals.
Methacholine provocation tests and recovery time of FEV1
Compliance with drug intake was more than 80% for both inhalers in all three study periods. Adverse events were reported by seven of 18 patients treated with formoterol, five of 17 treated with salmeterol, and seven of 18 following treatment with placebo. Besides respiratory symptoms and airway infections, five patients reported headache, four tremor, and one palpitations.
Discussion
This study shows that the magnitude of effect of salbutamol is equally decreased and its onset equally delayed following pretreatment with both formoterol and salmeterol in patients using inhaled glucocorticosteroids. This observation is not due to the difference in partial agonist properties of the two long acting β2agonists since no difference between the two drugs was observed. However, despite using equipotent doses—which was also shown by similar and probably maximal bronchodilatation with the two drugs—formoterol had a stronger bronchoprotective effect than salmeterol when more than 20% bronchoconstriction was induced. This confirms in vitro findings that formoterol has a greater intrinsic activity and is a fuller agonist than salmeterol, especially in contracted bronchi.7 ,8 A similar stronger bronchoprotective effect of formoterol was also shown recently in a clinical study using high single doses.20
To the best of our knowledge, this study is the first to compare the bronchodilator response of salbutamol during regular treatment with the two long acting β2 agonists formoterol and salmeterol in the same patients using methacholine provocation to mimic a moderate to severe asthma attack.
We used high doses of formoterol and salmeterol and treatment lasted for 14 days to provide maximum stimulation of the β2 receptor and to establish a situation in which tolerance was likely.9 The methacholine provocation test was performed 1 hour after administration of the last dose of formoterol and salmeterol, when the effects of formoterol and salmeterol were expected to be maximal and when a potential antagonistic property, reflected as a difference in response to the additional salbutamol, would be most apparent. Salbutamol was chosen to reverse methacholine induced bronchoconstriction rather than fenoterol because salbutamol is the most widely used rescue medication, despite the fact that fenoterol is a fuller agonist.7 ,8The dose of salbutamol used may appear to be low but, when inhaled via a Turbuhaler, a 50 μg dose of salbutamol has been reported to be equipotent to 200 μg by Rotahaler or Diskhaler21 or 100 μg by metered dose inhaler22 and has been shown to be effective during acute bronchoconstriction.4 A single dose was used to increase the likelihood of detecting small differences between the two long acting β2 agonists.
At the time of salbutamol inhalation the mean FEV1 had decreased by 39%, corresponding to a moderate to severe asthma attack. After pretreatment with placebo there was a rapid onset of salbutamol action as shown in a previous study.4 However, a decreased response to inhaled salbutamol, expressed both in magnitude and as recovery time, was observed after both active treatments with no difference between the two treatments.
The observed lower sensitivity to inhaled salbutamol may have several causes. Firstly, there is evidence that continuous treatment with long acting β2 agonists leads to a reduction in their bronchoprotective effect to a number of bronchoconstricting stimuli.23-25 This loss of bronchoprotective effect is due to β2 receptor downregulation (tolerance) which is associated with subsensitivity to salbutamol, as shown in this study. This tolerance can only have been induced by the long acting β2 agonists since no additional β2 rescue medication was used during the study period. There is, however, controversy about the development of the diminished bronchodilator effect of salbutamol after long term treatment with long acting β2 agonists, as seen in our study. Some studies have found that bronchodilator subsensitivity to cumulative doses of salbutamol may be induced after continuous treatment with long acting β2 agonists, as shown by an increase in FEV1from baseline,11-13 ,15 with no induction of subsensitivity after long term treatment with formoterol.13 Others have determined the absolute values of lung function16-18 and found no reduction in the sensitivity to the bronchodilating effects of salbutamol. Probable explanations are differences in baselines16-18 and in the time of the last dose of long acting β2 agonist (within 12 hours17 ,18 or after 12 hours11-13 ,15 ,16). Also, unlike this study, concomitant β2 agonist rescue medication was used during placebo treatment in some studies17 ,18 and some remaining β2 receptor stimulation may have induced the reduced sensitivity. In none of these studies was the methacholine provocation test model used. The justification for distinguishing tolerance between the bronchodilator and bronchoprotective response has been questioned. The methacholine provocation test has recently been used to show that continuous treatment with short acting β2 agonists induces bronchodilator tolerance,26 something that other methods had previously failed to do.27 ,28 In this situation of increased bronchomotor tone, relaxation of airway smooth muscle may require more β2 receptor activity and tolerance is easier to demonstrate.26 It seems likely that continuous treatment with long acting β2 agonists will also lead to tolerance in bronchodilating response, similar to the loss of bronchoprotective effect seen previously.
Secondly, in the present study the methacholine provocation test was performed at the peak of the agonist response. This may have obscured the effects of salbutamol because of the high degree of receptor occupancy induced. It was previously been shown that inhaled formoterol (72 μg) and salmeterol (300 μg) antagonised extrapulmonary β2 receptor mediated responses to inhaled fenoterol,29 while a single, much lower dose (formoterol 12 μg, salmeterol 25 μg) had no such significant effects.30 This indicates that, in the latter situation, a lower degree of receptor occupancy occurred and this did not interfere with fenoterol.
Thirdly, after active treatment a higher dose of methacholine was administered which may have led to a slower recovery in FEV1. When tested in the ANCOVA, however, the PD30+ was not a significant covariate.
The relative contribution of the partial agonist property, β2 receptor downregulation, and receptor occupancy to the observed diminished response to salbutamol could not be assessed in this study. As we did not study spontaneous recovery with placebo as rescue medication, the exact additional effect of salbutamol could not be determined. Furthermore, we did not investigate the effect of salbutamol after a single dose of the two long acting β2 agonists simultaneously. These measurements may have provided additional information with regard to the partial antagonistic properties and the development of tolerance. It is possible that the effects of receptor occupancy and tolerance may have overshadowed the effect of partial antagonism in the present study. The almost identical recovery time following the two active treatments may have been a consequence of this and may be a reason why no clinically relevant contribution resulting from the partial β2 antagonistic property of salmeterol (to the additionally inhaled salbutamol) during maintenance treatment could be demonstrated.
These results differ from in vitro findings where salmeterol appeared to antagonise the relaxation of cholinergically contracted human bronchi induced by other β2 agonists such as salbutamol.7 ,8 The in vitro study also differed from our in vivo study in that the bronchi were contracted first, then incubated with salmeterol, formoterol or placebo and the dose response curve to salbutamol produced while, in our study, the bronchi were contracted after dosing with salmeterol, formoterol, and placebo. The present study more closely mimics the clinical situation where patients are using long acting β2 agonists and, despite this, experience an asthma attack; this is clinically more relevant than β2 agonist naive patients experiencing bronchoconstriction and then being treated with two simultaneous β2 agonists for reversal.
Additional studies are needed to assess interactions between long acting and short acting β2 agonists after a longer interval such as 12 hours from administration of the long acting β2 agonists when the bronchodilation and bronchoprotection of the long acting drug is submaximal. It would be expected that, at this time, patients are more vulnerable to an attack of bronchospasm requiring additional salbutamol rescue therapy.
This study shows that, after pretreatment with long acting β2 agonists, the bronchodilating effect of a single dose of salbutamol is diminished, both in magnitude and onset. With a higher dose of salbutamol this phenomenon may have been missed. Indeed, in a recent study a higher dose of salbutamol was found to overcome terbutaline induced tachyphylaxis in a methacholine provocative test.26 However, a high dose of salbutamol did not overcome bronchoprotective subsensitivity in asthmatic patients receiving a single dose31 or regular treatment with salmeterol or formoterol,25 although in these latter studies some interaction caused by receptor occupancy may have occurred.
The present study shows that formoterol has a greater intrinsic activity than salmeterol. Theoretically, stronger β2receptor stimulation may lead to a stronger tendency towards desensitisation. If this occurred, it would have resulted in a decreased effect on the FEV1 12 hours after the previous dose and/or a poorer immediate response in FEV1 and PC20 after inhalation of the study medication. It would also have led to a diminished effect of salbutamol. However, we found small and insignificant differences between the two long acting β2 agonists on FEV1 before methacholine provocation, a significantly stronger protective effect against methacholine after formoterol compared with salmeterol, and an equally diminished response to inhaled salbutamol. These results indicate that formoterol does not cause a stronger desensitisation than salmeterol or, if it does, any difference is counterbalanced by the antagonist activity of salmeterol.
In summary, the present study did not confirm in vivo the observed in vitro findings of differences in (partial) antagonistic activities between salmeterol and formoterol. However, a higher intrinsic activity of formoterol was demonstrated in contracted bronchi which indicates that salmeterol is a partial agonist compared with formoterol in human airways in vivo in moderate to severe asthma attacks. The efficacy of an additional single dose β2 agonist is decreased in a situation of moderate to severe methacholine induced bronchoconstriction after pretreatment with formoterol and salmeterol. This suggests that patients on regular long acting β2 agonist treatment should be aware that a single dose of salbutamol may become less effective during an acute asthma attack.
Acknowledgments
The authors thank M Boorsma for help in designing, monitoring and analysing the study, AstraZeneca R&D Lund for preparing blinded medication, Professor J Zaagsma for critically reviewing the manuscript and G D Nossent, M P Politiek, L H Steenhuis, W J Snoek, C G Tol, and S H Wills for contributions to the clinical part of the study.
References
Footnotes
Thi study was supported by a research grant from AstraZeneca, the Netherlands.