Article Text

Abstract
Methods by which patients can artificially produce raised peak flow measurements have been described. We recently observed a patient manipulating the peak flow meter in a way that had not been described before. A study was therefore undertaken to determine if this technique could repeatedly produce clinically significant changes in peak flow readings. Fifteen adults, using a mini-Wright peak flow meter, made five measurements using the correct technique followed by five manipulated measurements under observation. Significant increases in peak flow measurements were observed in 14 of the 15 subjects. The mean increase in peak flow rate using the incorrect technique was 56% (range –4% to 86%). Clinicians should be aware that patients might employ this technique to manipulate measurements which could have consequences for management.
- peak flow measurements
- technique
- false results
Statistics from Altmetric.com
Peak flow measurement is used in asthma management.1 We are aware that peak flow measurements can be artificially increased by spitting or coughing.2 ,3 We recently observed a method of manipulating peak flow measurement which has not been previously described.
Case report
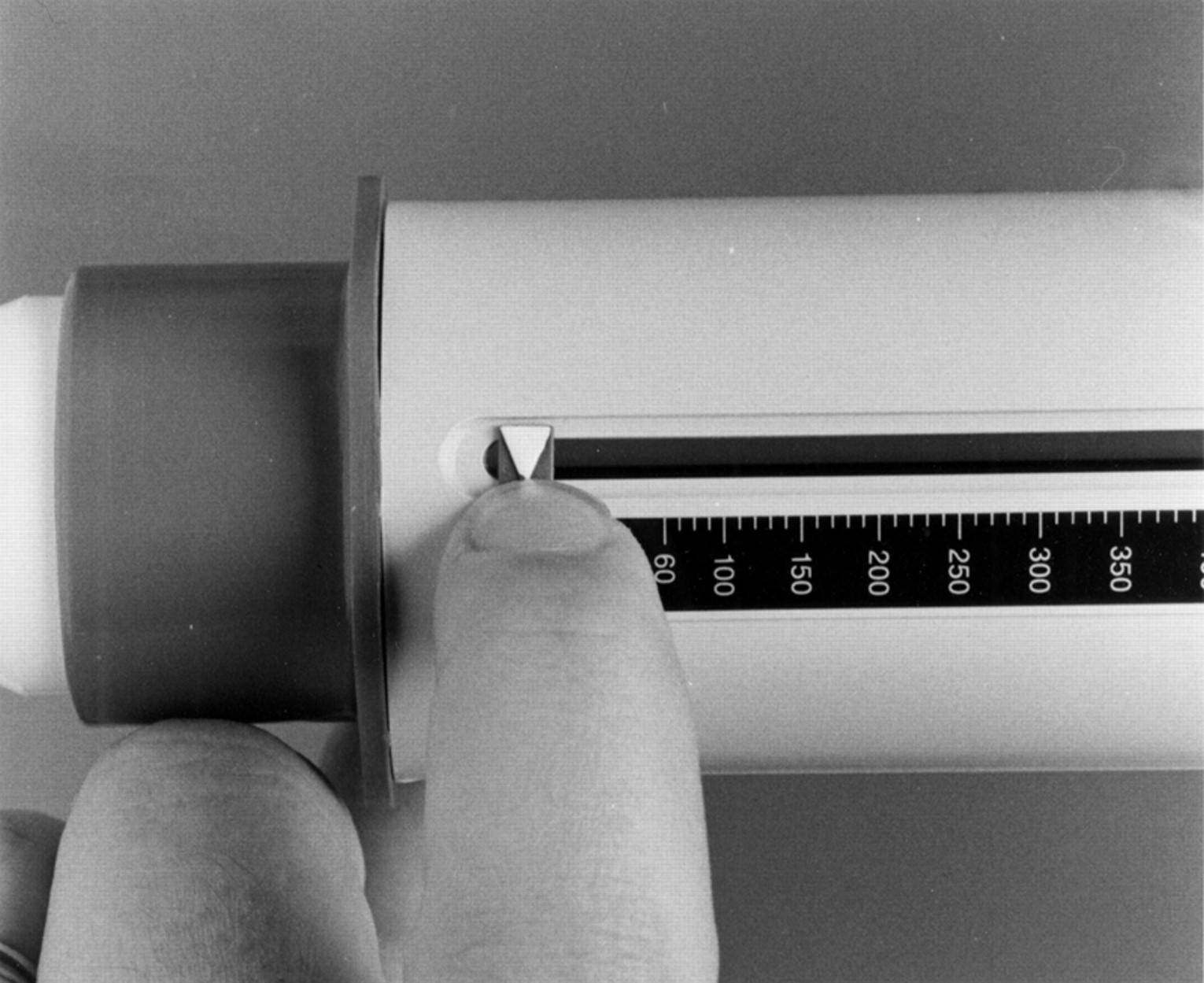
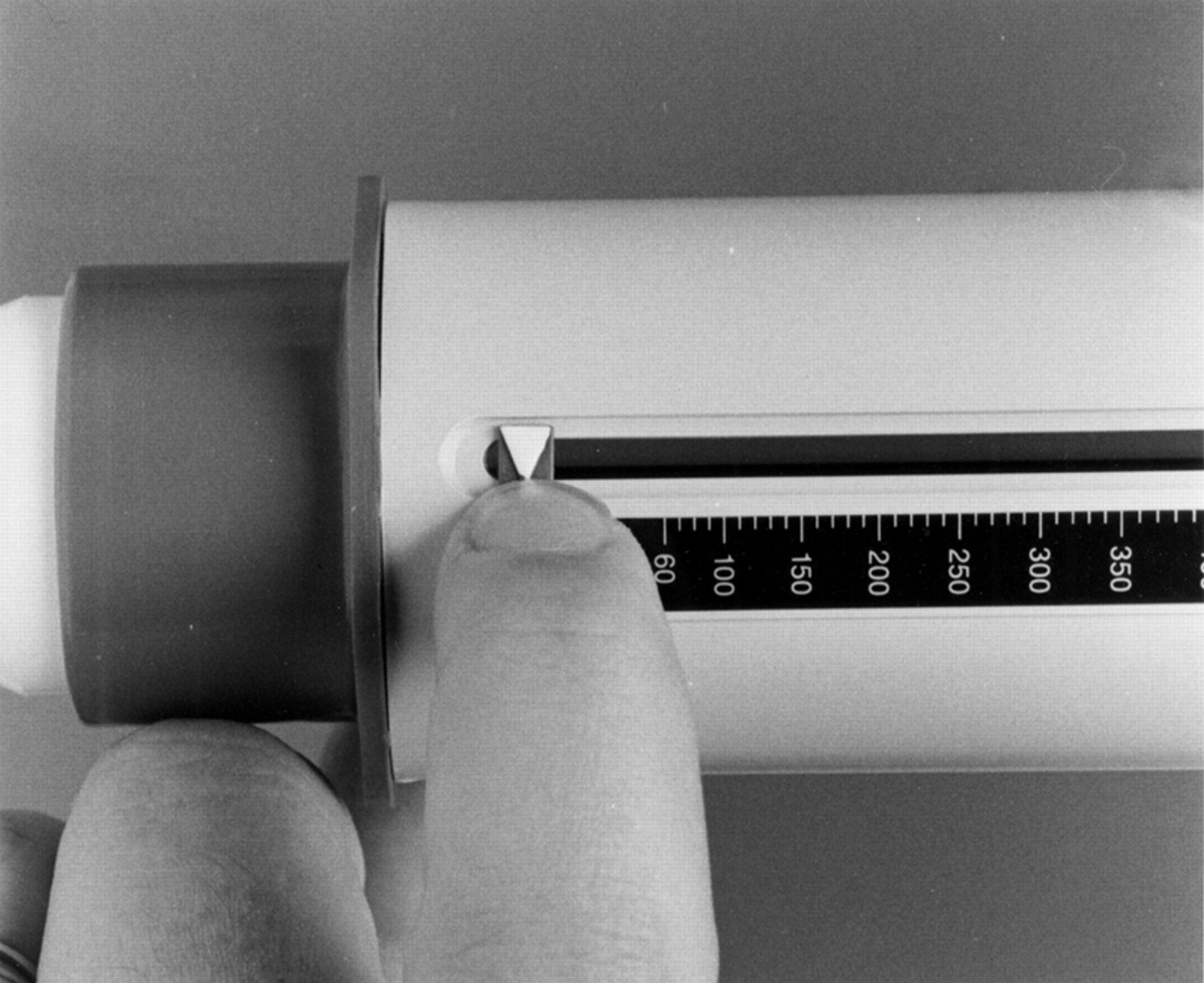
A 13 year old asthmatic boy was seen as an outpatient. He was prone to recurrent acute attacks of asthma and had four hospital admissions in the previous 3 months. The patient was asked to perform a peak flow measurement. During the manoeuvre his movements appeared slightly awkward and, when asked to explain, he admitted that he had discovered that, if he retarded the movement of the peak flow indicator with his index finger at the beginning of the manoeuvre for a fraction of a second after starting to exhale (fig 1), he could increase the reading. He also explained that, if he moved vigorously during the procedure, it appeared that he was giving maximum effort to performing the measurement and this made it difficult for the doctor to detect what he was doing with his finger.
{kind=link}
Position of index finger when retarding movement of peak flow indicator.
A study was therefore undertaken to determine whether this technique could repeatedly produce clinically significant changes in peak flow readings.
Methods
Fifteen adults, one of whom had asthma, were asked to make five peak flow measurements in the standard way followed by a further five peak flow measurements by retarding the movement of the peak flow indicator as described in the case report, after an initial practice. All measurements were carried out using a mini-Wright peak flow meter.
Results
The results are shown in table 1. Both the mean and the best of five readings for the two techniques were recorded. It can be seen that altering the technique of peak flow measurement (as described in the case study) produced significant increases in peak flow rate in 14 of the 15 subjects. Using the mean of the five attempts, a mean increase of 28% (range –2% to 66%) was achieved. When the highest of the five attempts was taken as representative, the mean increase was 56% (range –4% to 85%).
Results of peak flow measurements
Discussion
Peak flow recording is important in asthma management1 and these measurements are used to inform decisions about the need for referral to hospital, admission, and timing of discharge. Patients dislike being in hospital and may be tempted to manipulate peak flow measurements in order to give falsely raised readings that could influence their management. For example, patients may have a true peak flow <50% of their personal best but, by falsely increasing the peak flow measurement by 28%, management could be quite different. Clinicians need to be aware of this and of other manoeuvres that lead to falsely raised readings. We would emphasise that it is possible to interfere with the movement of the peak flow indicator with subtlety and this would not be readily noticed unless the clinician is watching closely. Asking patients to “cradle” the peak flow meter with a hand underneath the device is likely to prevent this problem.