Article Text

Abstract
BACKGROUND We have previously reported that disseminated pulmonaryMycobacterium avium complex (MAC) infection is more common in human T lymphotrophic virus type I (HTLV-I) carriers than in non-carriers. However, the reason for this remains unclear. It has been shown that glycopeptidelipid (GPL), one of the lipid components of the cell envelope of MAC, is able to reduce the lymphocyte blastogenic response to mitogens. The purpose of this study was to clarify whether or not the inhibitory effect of GPL differs between HTLV-I carriers and non-carriers.
METHODS Peripheral blood lymphocytes were obtained from 29 patients who had recovered from pulmonary MAC infection (10 of whom also had HTLV-I infection) and the lymphocyte counts and T cell subpopulations of the peripheral blood lymphocytes in HTLV-I carriers and non-carriers were compared. The inhibitory effect of GPL on the lymphocyte blastogenic response to phytohaemagglutinin (PHA) was tested in these 29 cases and in 15 healthy controls who had never suffered from MAC (seven of whom also had HTLV-I infection). All HTLV-I positive cases were carriers.
RESULTS There was no significant difference in the numbers or subset proportions of T cells between HTLV-I carriers and non-carriers. Lymphocyte activation by PHA was significantly inhibited by GPL in MAC positive and negative HTLV-I carriers compared with MAC negative non-carriers and MAC negative healthy controls (p<0.001).
CONCLUSIONS We suggest that MAC infection leads to strong inhibition of lymphocyte activation in HTLV-I carriers. This may account, in part, for the severity of pulmonary MAC infection in HTLV-I carriers.
- lymphocyte blastogenic response
- glycopeptidelipid
- HTLV-I carriers
- Mycobacterium aviumcomplex
Statistics from Altmetric.com
Mycobacterium avium complex (MAC) commonly causes problems in patients with CD4+ T lymphocyte abnormalities such as AIDS.1 We recently reported that pulmonary MAC infection is more common and spreads more widely in human T lymphotrophic virus type I (HTLV-I) carriers than in non-carriers.2 However, the reasons for this difference still remain unclear. MAC is classified into serotypes according to the serovar-specific glycopeptidelipid (GPL) antigens, one of the lipid components of the cell envelope of MAC, using seroagglutination of whole cells or thin layer chromatography.3 Serovar 4 MAC infection is most common in AIDS4 and is known to be able to reduce the lymphocyte blastogenic response to concanavalin A (Con A) and phytohaemagglutinin (PHA).5 In addition, there have been some reports regarding the immunological effects of HTLV-I on lymphocytes—for example, the effect on lymphocyte populations6 and the effect of PHA on T lymphocytes of asymptomatic HTLV-I infected individuals.7 This study was undertaken to compare the inhibitory effect of GPL on the lymphocyte blastogenic response to PHA in HTLV-I carriers and non-carriers and to clarify the immunological abnormality associated with MAC infection in HTLV-I carriers.
Methods
SUBJECTS
Blood samples were obtained from 29 individuals who had recovered from pulmonary MAC infection, 10 of whom also had HTLV-I (all women, mean (SD) age 70.1 (10.2) years) and 19 who did not have HTLV-I (16 women, mean (SD) age 70.9 (9.5) years).2 They had neither systemic nor local underlying disorders which might predispose to pulmonary MAC infection such as alcoholism and residual pulmonary damage from previous infection, nor any unexplained pulmonary diseases or other pathogens. HTLV-I infection was serologically diagnosed with an Eitest-ATL kit (Eisai Inc, Tokyo, Japan). The HTLV-I positive cases had never had adult T cell leukaemia or HTLV-I associated myelopathy. MAC infection had been diagnosed based on culture of sputum or bronchial washing fluids on Ogawa egg medium on at least two separate occasions. They had all received treatment and were now clinically well.
Fifteen healthy volunteers were also recruited, seven of whom also had HTLV-I (five women, mean (SD) age 68.8 (8.1) years) and eight who did not have HTLV-I (six women, mean (SD) age 69.2 (8.8) years) as healthy controls. None of the volunteers had any disease such as collagen disease or AIDS which might cause immunological abnormalities and pulmonary disorders, and none had ever been infected with MAC. The HTLV-I positive volunteers had never had adult T cell leukaemia or HTLV-I associated myelopathy.
All the cases and volunteers gave written consent to participate in the study.
T CELL SUBSETS IN PERIPHERAL BLOOD LYMPHOCYTES
Total lymphocyte counts and lymphocyte subsets in the peripheral blood of MAC infected HTLV-I carriers, MAC infected non-carriers, and healthy volunteers were measured by flow cytometry on at least two separate occasions.
EXTRACTION AND PURIFICATION OF GPL FROM MAC
Serovar 4 of MAC was identified by thin layer chromatography3 and GPL was extracted as reported previously,5 after which it was dissolved in propanol:methanol (2:1).
PROLIFERATION ASSAY
The GPL solution was added to a 96-well round bottom plate (Iwaki Glass Co Ltd, Tokyo, Japan) and dried under sterile conditions. Peripheral blood lymphocytes were separated from heparinised venous blood by the Ficoll-Hypaque sedimentation method as described previously.8 The lymphocytes were suspended at 5 × 105/ml in RPMI-1640 with 10% heat inactivated fetal bovine serum (Flow Laboratories Inc, McLean, VA, USA). Lymphocytes (5×104) were transferred to the wells in the 96-well plates with or without coated GPL. PHA (Wellcome Research Laboratories, Beckenham, UK) was then added to each well at a concentration of 10 μg/ml. Cells were incubated at 37°C in 5% CO2 for 72 hours.
During the final 4 hours of incubation Alamar Blue (20 μl/well; Nalge Nunc International, NY, USA) was added to each well and the fluorescence was measured using Fluoroskan Ascent (Labsystems, Helsinki, Finland).9 We measured the absorbance at a wavelength of 590 nm. The assay was carried out in duplicate. The absorbance showed a significant positive correlation with direct cell count by Trypan blue staining (r = 0.95, p<0.0001, Pearson's correlation coefficient, data not shown). The proliferation index (PI) was used to measure the lymphocyte proliferation rate by the following formula:
PI = (count in the presence of PHA − count in medium alone)/(count without PHA − count in medium alone)
To compare the degree of GPL inhibition the relative reduction in PI was calculated using the following formula:
% reduction = (PI with GPL)/(PI without GPL) × 100
STATISTICAL ANALYSIS
The Mann-Whitney U test and one way factorial ANOVA with Banferroni-Dunn test were used to compare the PI and percentage reduction in PI in the four groups. p values below 0.025 were considered significant.
Results
There were no significant differences in white blood cell counts, lymphocyte counts, and T cell subpopulations between the four groups (table 1).
Mean (SD) white blood cell counts, lymphocyte counts, T cell subpopulations and PI values in the four study groups
We first determined that the optimal PHA concentration to give the maximal lymphocyte blastogenic response in healthy volunteers was 10 μg/ml (data not shown). We next established that the optimal amount of GPL to show the maximal inhibitory effect on the lymphocyte blastogenic response with a minimal cytotoxic effect on the lymphocytes in the presence of 10 μg/ml PHA was 75 μg/well (data not shown). Further studies were conducted under these optimal conditions.
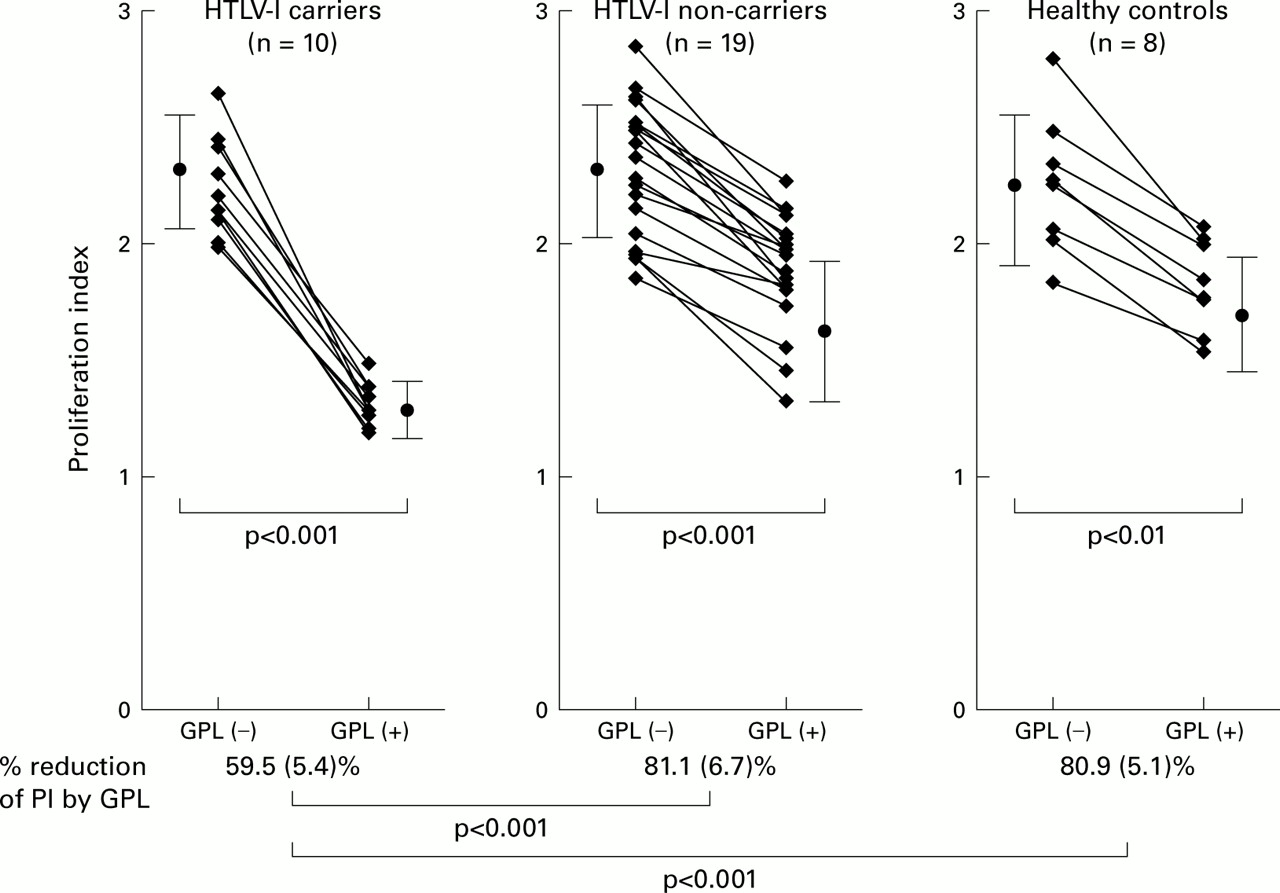
The PI values in the MAC infected HTLV-I carriers, MAC infected non-carriers, healthy HTLV-I positive volunteers, and healthy HTLV-I negative volunteers were 2.22 (0.19), 2.32 (0.28), 2.31 (0.33), and 2.25 (0.29), respectively. There was no significant difference between the four groups. GPL significantly reduced PI in each group, but the percentage reduction in PI by GPL was significantly greater in HTLV-I carriers than in non-carriers and healthy HTLV-I negative volunteers (fig 1, p<0.001). The percentage reduction in PI by GPL was also significantly greater in healthy HTLV-I positive volunteers than in MAC infected non-carriers and healthy HTLV-I negative volunteers (60.2 (6.8)%, p<0.001). There was no significant difference in the reduction in PI by GPL between MAC infected HTLV-I carriers and healthy HTLV-I positive volunteers.
{kind=link}
Proliferation index with or without GPL in HTLV-I carriers, non-carriers, and healthy controls. Lymphocyte proliferation was significantly inhibited by GPL in all cases (p<0.001 in HTLV-I carriers and non-carriers, p<0.01 in healthy controls). The percentage reduction in PI by GPL was significantly greater in HTLV-I carriers than in non-carriers and healthy volunteers (p<0.001). Closed circles show mean values and bars show standard deviations in each group.
Discussion
In this study we have shown that inhibition of the lymphocyte blastogenic response to PHA by GPL was enhanced in HTLV-I carriers compared with non-carriers and healthy volunteers under the experimental conditions in which optimal concentrations of GPL and PHA were used. Without GPL the PI did not differ between the groups using a PHA concentration of 10 μg/ml at which lymphocytes proliferate considerably. Moreover, lymphocyte counts and T cell subsets did not differ between the three groups.
HTLV-I preferentially infects CD4+ cells in vivo and would modify T cell function.10 CD4+ lymphocytes play a pivotal role in immunological defence against microorganisms including MAC.1 ,4 These findings are in agreement with previous reports suggesting that suppressed cellular immunity in HTLV-I carriers, for example, leads to an increase in the prevalence of infectious diseases11 and the weakness of the tuberculin skin reaction.12 However, in some HTLV-I carriers there was no disturbance in T lymphocyte subsets.7 In the present study we could not find any differences in lymphocyte counts and T cell subsets in the peripheral blood lymphocytes. The PI values with PHA stimulation were notably similar in both the HTLV-I carriers and non-carriers while the inhibitory effect of GPL was more apparent in HTLV-I carriers than in non-carriers, which suggests a subclinical abnormality in lymphocytes of HTLV-I carriers.
Lymphocyte suppression by GPL of serovar 4 MAC is considered to be one of the important factors in the pathogenesis of MAC infection.4 ,5 HTLV-I infection affects not only the peripheral blood lymphocytes but also the lymphocytes in the lungs.13 ,14 Taken together, we think that the enhanced inhibitory effect of MAC GPL observed in this in vitro study is one of the reasons why MAC spreads more widely in lungs of individuals infected with HTLV-I.2 It may be necessary to treat pulmonary MAC infection in HTLV-I carriers even if there are no immunological abnormalities in the clinical data.
References
1st Asia Pacific Forum on Quality Improvement in Health Care 19–21 September 2001 Sydney, Australia
We are delighted to announce this forthcoming conference in Sydney.
Authors are invited to submit papers (call for papers closes on Friday 6 April) and delegate enquiries are welcome. The themes of the Forum are:
Improving patient safety
Leadership for improvement
Consumers driving change
Building capacity for change: measurement, education and human resources
The context: incentives and barriers for change
Improving health systems
The evidence and scientific basis for quality improvement
Presented to you by the BMJ Publishing Group (London, UK) and Institute for Healthcare Improvement (Boston, USA), with the support of the Commonwealth Department of Health and Aged Care (Australia), Safety & Quality Council (Australia), NSW Health (Australia), and Ministry of Health (New Zealand).
For more information contact:quality{at}bma.org.uk or fax +44 (0) 7383 6869
Footnotes
This study was supported by the Program for Promotion of Fundamental Studies in Health Sciences of the Organization for Pharmaceutical Safety and Research (OPSR) Japan.