Article Text

Abstract
BACKGROUND To study bronchial responsiveness to adenosine 5′-monophosphate (AMP) in population surveys, repeatability of a rapid dosimetric method with quadrupling doses was evaluated.
METHODS Volunteers with symptoms of airway respiratory allergy or asthma were invited for AMP challenges on two occasions. After each dose the fall in forced expiratory volume in one second (FEV1) compared with the post-saline value was determined. The cumulative doses of AMP needed to cause a fall in FEV1 of 20% (PD20), 15% (PD15), and 10% (PD10) were calculated. Agreement was evaluated by means of kappa values. After excluding systematic differences in PD values on two occasions (t test), repeatability of a single estimation of the chosen PD values was calculated and expressed in doubling doses (DD).
RESULTS In 28 of 76 subjects a PD20 was estimated on the two visits, in 29 subjects a PD15 was estimated, and in 32 a PD10was obtained. Kappa values for a positive threshold were 0.89 for a cut off level for a 20% fall in FEV1, 0.78 for a 15% fall in FEV1, and 0.76 for a fall in FEV1 of 10%. The PD values did not differ between the two visits and 95% repeatability of a single estimation was ±1.7 DD for PD20, ±2.2 DD for PD15, and ±2.4 DD for PD10. The quadrupling dose method reduced time by 40% in non-hyperresponsive subjects and no adverse effects were observed.
CONCLUSION The short dosimeter protocol with quadrupling doses for AMP challenges is a rapid, reproducible tool for estimating bronchial responsiveness in population surveys.
- adenosine-5′-monophosphate (AMP)
- repeatability
- short dosimeter protocol
- bronchial hyperresponsiveness
Statistics from Altmetric.com
Non-specific bronchial hyperresponsiveness (BHR) is considered a central feature of asthma. BHR can be measured by a variety of stimuli, of which histamine and methacholine are most commonly used. Both substances predominantly induce bronchoconstriction by a direct effect on airway smooth muscle. Another way to induce bronchoconstriction is by provoking mediator release from inflammatory cells in the bronchi with subsequent smooth muscle contraction.1 BHR measured by this “indirect” method may provide different information on airway lability from that obtained with directly acting stimuli.
In recent years adenosine-5′-monophosphate (AMP) has been studied as an “indirect” stimulus. Although the precise mechanism by which AMP causes bronchoconstriction has not been clarified in detail, release of inflammatory mediators from mast cells plays an important role, as well as activation of nerve fibres.2-4 Several studies have indicated that airway responsiveness to AMP is a more accurate marker of bronchial inflammation in asthma than hyperresponsiveness to methacholine or histamine. Bronchial responsiveness to AMP is reduced after allergen avoidance or treatment with anti-inflammatory drugs, while responsiveness to methacholine is not.5-7 Some studies have suggested the possibility of differentiating between asthma and chronic obstructive pulmonary disease (COPD) by bronchial responsiveness to AMP, since patients with asthma have been found to have a more pronounced BHR to AMP than those with COPD.8 ,9
To date, studies on BHR to AMP have only been performed in patients with clinically diagnosed asthma or COPD. Population studies might give an insight into the value of BHR to AMP as a risk factor for asthma and determine its value in the diagnosis and therapeutic monitoring of patients with mild asthma. However, most subjects in open population studies are either not hyperresponsive or respond only at high doses, so challenge procedures using standard protocols with doubling doses (DD) until a 20% fall in forced expiratory volume in one second (FEV1) has been reached are time consuming and may influence compliance of participants. The availability of a short protocol would make it more feasible to study BHR to AMP in an open population.
The aim of this study was to evaluate the repeatability of a short dosimeter protocol in which doses of AMP are quadrupled. To include subjects with a minor degree of airway obstruction, as in population studies, we assessed the repeatability for the cumulative dose of AMP which caused a 20% fall in FEV1 (PD20), as well as falls of 15% (PD15) and 10% (PD10).
Methods
POPULATION AND STUDY DESIGN
Volunteers aged 20–45 years were recruited from the department and from two universities. The study population consisted of 29 volunteers in 1995 and 47 in 1998/9. In 1999 we selected subjects at risk of BHR by questionnaire on symptoms of airway allergy or asthma. AMP challenges using a protocol with quadrupling dose intervals were conducted twice at the same time of day at an interval of 2–14 days. Subjects with cardiovascular or neurological disorders were excluded, as were subjects with a baseline FEV1 of <1.5 l. Cromoglycate and antihistamines were withheld for 48 hours and β-sympathomimetic agents were withheld for 8 hours before the challenge. Subjects were asked not to smoke during the hour before testing. At the second appointment the subjects were questioned about side effects. If the second appointment was missed, subjects were approached by telephone.
In 1995 subjects were also challenged according to the standard dosimeter protocol with doubling dose intervals. A PD20AMP was obtained by both protocols in seven subjects; the standard protocol yielded a somewhat higher mean PD20AMP than the short one with a mean difference of 0.7 DD (95% CI 0.2 to 1.2). We decided not to include the standard protocol in the population studied in 1999 because the difference between the two protocols was small. Furthermore, the short protocol is particularly useful in epidemiological studies of subjects in whom bronchial hyperresponsiveness, if present, is usually mild and where repeatability is the predominant issue of concern.
Informed consent was obtained from each subject and the Wageningen University ethical board approved the study.
LUNG FUNCTION
In 1995 lung function was measured with a dry rolling seal spirometer (Mijnhardt, Groningen, Netherlands) and in 1999 with a pneumotachometer (Jaeger, Germany). During lung function measurement subjects were seated in an upright position, wearing a nose clip. Prior to bronchial challenge forced expiratory manoeuvres were repeated until two readings of reproducible values for FEV1(within 5%), forced vital capacity (FVC, within 5%), and peak expiratory flow (PEF, within 10%) were reached.10 ,11 The highest FEV1 value was used in the analyses. If no reproducible values for FEV1 were recorded, the highest of the two most consistent acceptable spirograms was used. All lung function parameters were corrected to body temperature and pressure saturated with water vapour (BTPS).
AMP CHALLENGE
Bronchial challenges were performed using a breath actuated dosimeter APS (Jaeger GmbH, Germany). The dosimeter was powered by compressed air at 20 psi. The inhalations were made from functional residual capacity (FRC) to total lung capacity (TLC) and held for 8–10 seconds. Subjects wore a nose clip during the inhalation procedure.
Nebulisers were calibrated before and after the measurement sessions. Nebuliser output was constant during the study periods. In 1995 the mean output was 4.10 μl/s and inhalation time was fixed at 2.2 seconds, and in 1999 mean output was 3.60 μl/s. To avoid increasing the number of dose steps, inhalation time, or number of inhalations per dose step, AMP dilutions were concentrated compared with 1995. To assure a similar cumulative dose the inhalation time was set at 2.0 seconds for this study period.
AMP solutions were made in 0.9% saline. Table 1 shows the inhalation scheme and calculated cumulative doses for both study periods. In principle, doses were quadrupled except for the last one. Two minutes after each dose step two reproducible efforts for FEV1 were achieved. The post-saline value for FEV1 was chosen as a reference. If the post-saline FEV1 fell more than 10% compared with FEV1 before the challenge, subjects were excluded from further challenge. If FEV1 fell more than 6% compared with the reference, the test was continued with doubling doses according to the inhalation scheme. The test ended if FEV1fell by 20% or more from the post-saline value, or after inhalation of the highest dose. Salbutamol aerosol was administered to treat bronchoconstriction, if needed.
Inhalation schemes used for AMP challenge
Both the test subjects and observer were blind to the results of the first challenge, as far as possible. During the challenge no information was given about lung function results, and FEV1values of previous dose steps were not visible to the observer.
DATA ANALYSIS
Cumulative doses of inhaled AMP causing a fall in FEV1of 20% (PD20), 15% (PD15), and 10% (PD10) were calculated. The cumulative dose needed to cause this fall in FEV1 was estimated by linear interpolation between the last two points. To increase the number of subjects with a positive threshold we did separate analyses by including PD values determined by extrapolation over one doubling dose (DD).
Kappa values were calculated for the agreement of a positive threshold. For calculation of the mean difference in PD values and the repeatability of a single estimation, the PD values were log2 transformed to express differences in DD, which is equivalent to the number of dose steps in a standard dosimeter protocol.12 To estimate the repeatability of a single PD value we used the stepwise method described by Bland and Altman.13 Firstly, a paired ttest was used to test for a systematic difference in reference FEV1 and PD values. The difference in PD values was then plotted against their mean to evaluate a potential relationship. After excluding the probability of systematic differences, the limits of agreement were calculated as the mean difference ±2SD; these were considered meaningful for use in epidemiological studies if they did not exceed ±3 DD.11 The repeatability of a single estimation of the PD value was calculated from the 95% range of a single measurement using the formula:t 0.05 × SD(within subject). The within subject SD was calculated by dividing the SD of the difference in log2 (PD) by the square root of 2. The calculated repeatability was expressed as a doubling dose interval (log2 equivalent) and reflects agreement between tests for an individual.
To test whether the change in equipment influenced the results, separate analyses were performed for each study period.
Results
Of the 76 subjects studied, 75 (47 women, 28 men) of mean age 29 years (range 20–45) completed the study protocol with two AMP challenges. The mean period between the tests was 7 days (range 2–14).
Table 2 shows the agreement of a threshold at the defined cut off levels for a fall in FEV1 of 20%, 15%, and 10%. The agreement of a positive threshold between the two tests was 94.5% for PD20, 89.3% for PD15, and 88.0% for PD10. The kappa value was highest for PD20 and lowest for PD10, with PD15 intermediate. The inclusion of PD values achieved by extrapolation did not change the kappa values markedly, except for PD10.
Agreement of positive and negative thresholds measured on two occasions and kappa values at cut off levels of 20%, 15% and 10% fall in FEV1 (n=75)
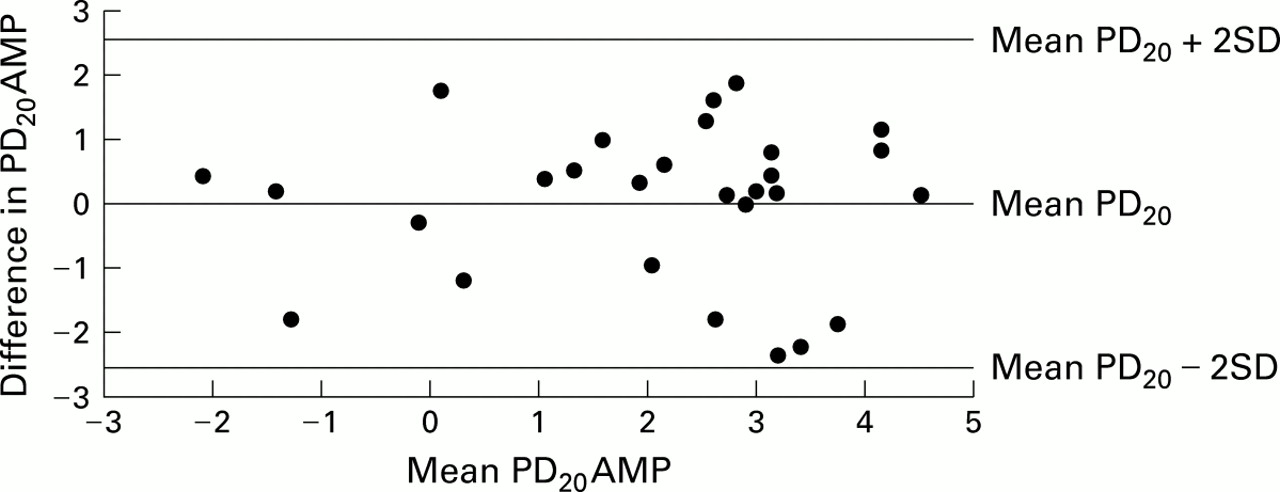
Figure 1 and table 3 show the repeatability of the actual PD values obtained. As shown in fig 1, there was no relation between the difference and the mean PD20 values at the two visits, allowing calculation of repeatability for the whole range of mean PD20 values. The limits of agreement were between –2.4 and +2.4 DD. Similarly, no relation between the difference and the mean values was seen for PD15 or PD10. Pre-challenge FEV1 values (3.80 l and 3.75 l) and PD values were the same at both visits, and the 95% repeatability of a single measurement was within 2–3 DD for all PD values, irrespective of whether or not extrapolated PD values were included. Exclusion of subjects measured in 1995, of whom three had a PD20, did not change the results.
{kind=link}
Difference between the two PD20 values against the mean PD20 (in log2PD20AMP).
Mean difference in PD20, PD15, and PD10 (with 95% CI) , and 95% repeatability in doubling doses AMP
In non-responsive subjects the AMP challenge using the quadrupling dose protocol took 25–30 minutes. No adverse reactions were observed during or after the challenge.
Discussion
In this study we have evaluated the repeatability of AMP challenges using quadrupling doses. According to the kappa value, the agreement was very good if BHR was defined as a fall in FEV1 of 20%. The 95% repeatability for a single measurement of PD20 was ±1.7 DD. In non-responsive subjects the short protocol took 25–30 minutes, resulting in a time gain of at least 40% compared with the standard dosimeter protocol using doubling doses. No adverse effects were reported during or after the challenge.
According to the kappa values the agreement for both the positive and negative thresholds was very good for PD20 and good for PD15 and PD10. However, the agreement of a negative threshold should be interpreted with caution as our population was not a random sample (in the second part of the study we selected subjects based on an increased chance of having BHR). Kappa values were almost the same if the definition of BHR was based on extrapolated PD values, except for the threshold defined by PD10. The agreement was similar for BHR defined by PD10 without extrapolated values and PD15 with extrapolated values. Thus, reproducibility is acceptable when using PD20 or PD15 values obtained by extrapolation over one doubling dose, but for PD10 extrapolation should be avoided as it has a considerable effect on reproducibility.
We did not find any difference in PD values between the two tests. The repeatability of a single PD20 value was similar to that in other studies which have evaluated short protocols for methacholine and histamine challenges.14-17 One study assessed the repeatability of PD20AMP and found limits of agreement between –4.54 and 3.78 DD.18 In this study the 95% repeatability for a single PD20AMP was ±3.1 DD. The cut off value for a 20% fall in FEV1 is a diagnostic criterion for obstructive airway disease which might be too restrictive for use in an open population. We therefore also determined the repeatability of PD15 and PD10 values that were both within the limit of 3 DD. Similar results were achieved for extrapolated PD values. The decision as to which cut off value should be used to define BHR has to be studied in relation to other measures of obstructive airway disease, particularly respiratory symptoms and lung function impairment.
We found a relatively large difference in both kappa values and 95% repeatability for PD20 compared with PD15 or PD10. Van Aalderen et al also determined the reproducibility of histamine challenge for PD20, PD15, and PD10 values and did not find a difference in repeatability.19 In our study there was no learning effect with respect to the performance of forced spirometric tests since baseline FEV1 was the same on both occasions. Circadian and seasonal variation did not affect the tests because measurements were made at the same time of day during all seasons and there was no time-dependent trend. Refractoriness to AMP can also be excluded since there were at least 2 days between the tests and, according to the literature, tachyphylaxis for repeated AMP challenges lasts only about 4 hours.20 Since there was no difference in PD20 between the two tests, bias resulting from knowledge of the first test results is unlikely. The slightly higher values for PD15 and PD10 at the second visit may be attributed to a training effect to complete the test. Both physical and psychological factors may play a part, with subjects being less exhausted by repeated lung function manoeuvres and anticipating the end of the test on the second occasion. The most likely explanation for the observed discrepancy in the kappa values and 95% repeatability for PD15 and PD10 compared with PD20 is a more precise measurement of a 20% fall in FEV1. The test protocol was fixed to a fall in FEV1 of 20%, and it might be that the examiner was more alert if the fall in FEV1 approximated this which may have resulted in increasing encouragement during lung function measurement ensuring a more accurate measurement of FEV1. Since PD15 and PD10 have been determined after the fieldwork, they will not have been biased in this way. However, one could equally well argue that the repeatability of these indices is underestimated because of less precise measurement of lung function at these cut off FEV1 values.
In summary, the reproducibility of a single estimation of PD20, PD15, and PD10 measured by a short dosimeter protocol with quadrupling doses is within 2–3 DD. The agreement between two determinations of BHR to AMP is good. The time needed to test non-hyperresponsive subjects is 25–30 minutes, and there are no adverse effects. We conclude that the short protocol is an acceptable and reproducible tool to test BHR in population surveys which may increase participation and reduce costs and logistical management of bronchial challenges.
Acknowledgments
The authors are grateful to the volunteers who participated in this study and to S de Wind and S van Gaans for their technical assistance. This study was supported by a grant from the Netherlands Asthma Fund and the Foundation Asthma Abatement.