Article Text

Abstract
BACKGROUND When monitoring patients with chronic lung disease it is important to distinguish genuine changes in gas transfer over time from natural variability. This study aims to define the coefficient of repeatability for routine measurements of single breath transfer factor (Tco) and transfer coefficient (Kco).
METHODS Sixty eight subjects (32 with emphysema, 36 healthy volunteers) had Tcomeasured twice at a mean (SD) interval of 7.5 (1.3) days. On each occasion a standard protocol (conforming to BTS guidelines) was followed, comprising duplicate measurements satisfying standard technical criteria. The mean of these duplicates was recorded. For the pooled data changes in Tco and Kco between study days were expressed as coefficient of repeatability.
RESULTS The coefficient of repeatability was ±1.60 mmol/min/kPa for Tco and ±0.24 mmol/min/kPa/l for Kco. Correcting Tco and Kco for prevailing barometric pressure or carboxyhaemoglobin level made no significant difference to the results.
CONCLUSIONS The quoted limits for variability in gas transfer over time are valid for a wide range of clinically relevant values. Changes in Tco and Kco greater than these limits are unlikely to arise from natural variation.
- transfer factor
- natural variability
- single breath method
Statistics from Altmetric.com
Measurements of single breath carbon monoxide transfer factor (Tco) and transfer coefficient (Kco) are used widely in the diagnosis and monitoring of respiratory disease. To define significant changes in gas transfer over time it is necessary to know the natural variability of the measurement.
Several small studies have investigated intrasubject coefficient of variation (CV%) and found values ranging from 2.4% to15%.1-5 Expressing variability as a percentage presupposes that variability is greater for higher values, but this has not been investigated.
The aim of this study was to define the variability of repeated routine measurements of Tco and Kco in both healthy volunteers and patients with emphysema. In addition, the effects of correcting for barometric pressure and carboxyhaemoglobin concentration on gas transfer results were investigated.
Methods
SUBJECTS
Two groups of subjects were selected whose gas transfer should be stable over the study period—healthy volunteers and patients with stable emphysema. The study was approved by Lothian research ethics committee and all subjects gave informed consent.
Healthy volunteers
Thirty six healthy volunteers with normal spirometric values6 ,7 and no respiratory disease were recruited. Five were current smokers, the remainder were non-smokers.
Emphysema patients
Thirty two patients with airflow obstruction, a clinical diagnosis of emphysema, and a Kco at least 1.65 SD below the predicted value8 ,9 were chosen to provide low but biologically stable values for Tco and Kco. Patients were excluded if they had suffered an upper respiratory tract infection or an infective exacerbation or had received oral steroids or antibiotics within the previous 3 months. Patients were withdrawn if their clinical condition changed between study days. No attempt was made to alter smoking behaviour (see below).
MEASUREMENT OF TCO AND KCO
To ensure the applicability of the results, local routine laboratory protocols were used. After 15 minutes of rest, forced expiratory volume in one second (FEV1) and vital capacity (VC) were measured (Vitalograph, Buckingham, UK). Up to four measurements of transfer factor were then made using a standard single breath method (Autolink bag-in-box device, Morgan Medical, Kent, UK; test gas mixture 0.28% CO, 14% He, 18% O2, balance N2, breath hold 9 seconds, 700 ml dead space discarded). Samples of inspirate and expirate were analysed for CO and He content following the absorption of carbon dioxide and water vapour. The breath hold time was recorded automatically according to the Jones-Meade method.10
Following local protocols, duplicate measurements of Tcowithin 0.5 mmol/min/kPa and Kco within 0.2 mmol/min/kPa/l were obtained from each subject on each study day and the mean values recorded for Tco, Kco, inspiratory volume, and alveolar volume. Tests were deemed technically acceptable if the inspired VC during the transfer test was within 500 ml of the spirometric VC.
Because of the clinical stability of the subjects and the short interval between study days, it was assumed that haemoglobin did not change significantly between the study days. Tco and Kco values reported here are not corrected for measured haemoglobin, but assume a standard value of 146 g/l.
STUDY DESIGN
Natural variability of measurements of transfer factor
Spirometric parameters and transfer factor were measured on all subjects on two separate days, at least 7 days apart. To prevent diurnal variation from influencing the results, subjects were studied at the same time on both days. British and European measurement guidelines11 ,12 were followed except for the requirement for patients not to smoke for 24 hours before testing, which was felt to be an unrealistic requirement with which patients were unlikely to comply.
Correction of gas transfer results for barometric pressure
Tco was calculated using the equation of Hill and Newall13 which includes barometric pressure. To investigate the effects of barometric pressure on Tcocalculations the values obtained using the ambient barometric pressure at the time of each test (from local Meteorological Office records) were compared with values calculated from the same data assuming a standard barometric pressure of 760 mm Hg.
Correction of gas transfer results for carboxyhaemoglobin concentration
To investigate the effect of correcting for changes in tobacco use, exhaled CO was measured on both study days in a subset of 35 patients using a hand held analyser (Smokerlyser, Bedfont Scientific Instruments). The concentration of carboxyhaemoglobin (COHb) was estimated from exhaled CO using the method of Waldet al.14 Test to test variability was calculated (a) not correcting for COHb and (b) correcting for calculated COHb on each day, and the results were compared.
DATA ANALYSIS
Changes in mean Tco and Kco between the two study days were calculated and the coefficients of repeatability (defined as 2SD) were derived for healthy subjects and patients with emphysema as separate groups and also for the pooled data. To examine how gas transfer variability changes with the magnitude of the measurement, data were plotted using the method of Bland and Altman.15
In the subgroup with exhaled CO measurements, subjects were classified as smokers, ex-smokers, or non-smokers. Pairedt tests were used to investigate changes in exhaled CO between the study days.
Results
Table 1 shows the basic biological data for the two study groups. The mean (SD) interval between study days was 7.5 (1.3) days (range 7–13 days). Inspiratory VC during the transfer test was 95.4 (5.7)% of the corresponding spirometric VC (absolute difference 0.15 (0.20) l; p=NS).
Mean (SD) data for the study subjects
NATURAL VARIABILITY OF MEASUREMENTS OF TRANSFER FACTOR
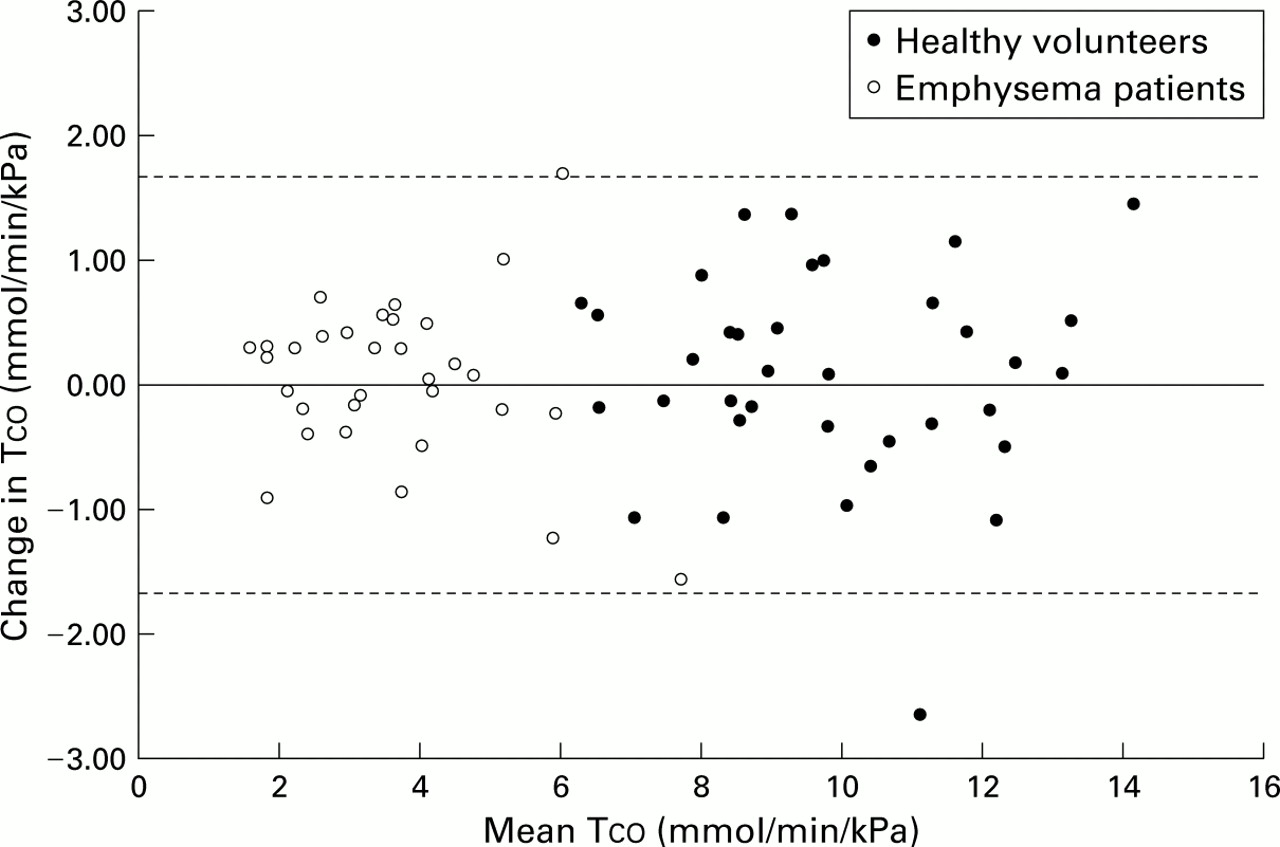
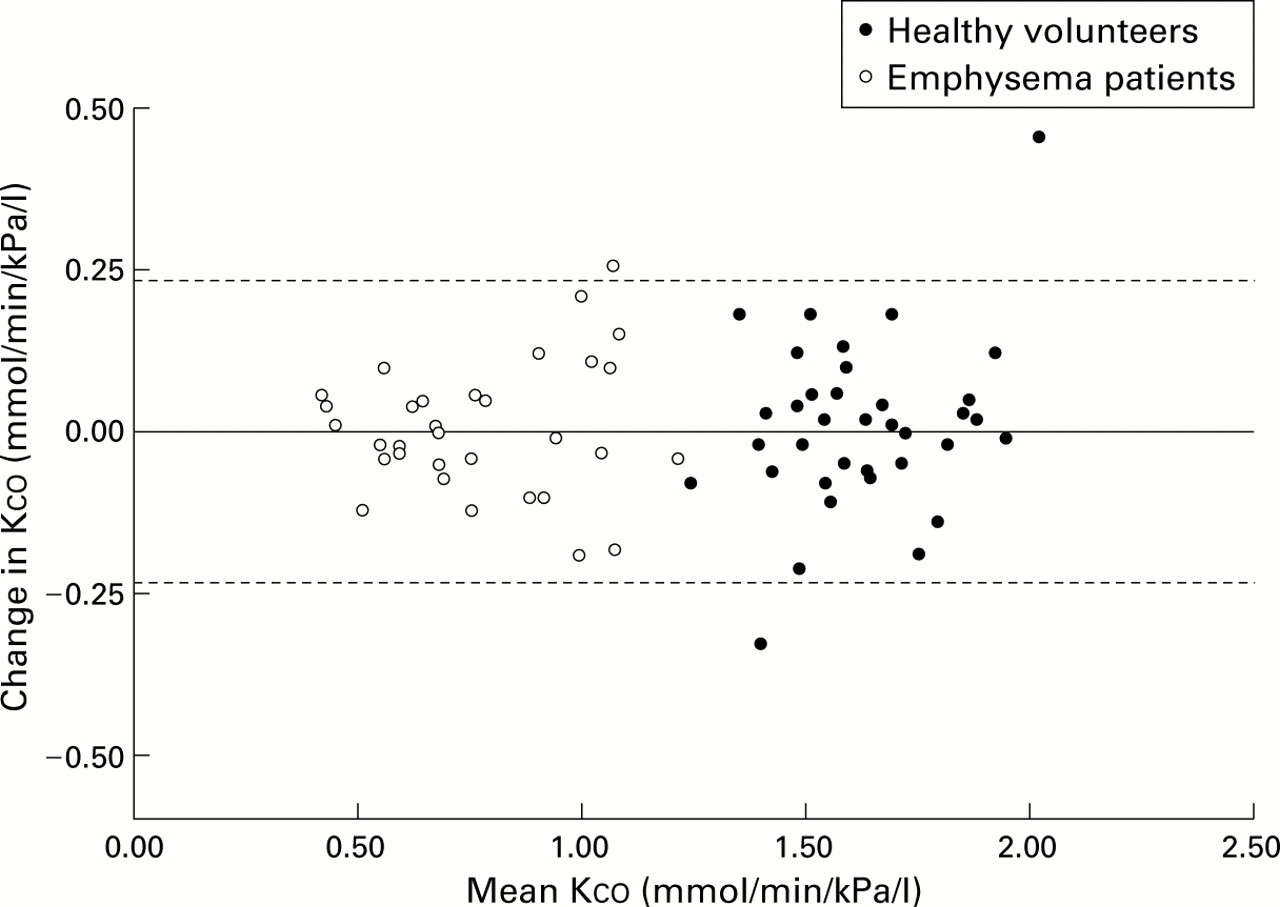
The coefficient of repeatability from the pooled data corrected for barometric pressure and COHb was ±1.60 mmol/min/kPa for Tco and ±0.24 mmol/min/kPa/l for Kco. For healthy volunteers the coefficient of repeatability for Tcowas ±1.84 and for Kco it was ±0.28. For patients with emphysema the corresponding figures were ±1.30 for Tcoand ±0.20 for Kco. Figures 1 and 2 are Bland-Altman plots indicating that day to day variability of Tco and Kco is largely independent of the magnitude of the measurement.

Bland-Altman plots of variability in carbon monoxide transfer factor (Tco) from pooled study data with coefficients of repeatability indicated by dashed lines.

{kind=link}
{kind=link}
Bland-Altman plots of variability in carbon monoxide transfer coefficient (Kco) from pooled study data with coefficients of repeatability indicated by dashed lines.
EFFECT OF CORRECTING FOR BAROMETRIC PRESSURE ON GAS TRANSFER REPRODUCIBILITY
During the study period barometric pressure varied from 725 to 779 mm Hg (mean 758 mm Hg). Inclusion of measured barometric pressure in the calculations changed Tco and Kco by 1.02 (0.73)%.
EFFECT OF CORRECTION FOR CARBOXYHAEMOGLOBIN ON GAS TRANSFER VARIABILITY
Exhaled CO levels were measured in 16 smokers, eight ex-smokers, and 11 non-smokers. Values ranged from 2 ppm to 37 ppm but there were no statistically significant changes in exhaled CO levels in any group between days 1 and 2 (95% of the individual results on day 2 were within 4 ppm of the corresponding values on day 1). The mean absolute change in Kco following correction for COHb was 2.04 (1.78)%, yielding coefficients of reproducibility of ±1.20 mmol/min/kPa for Tco and ±0.18 mmol/min/kPa/l for Kco. Exclusion of the correction for calculated COHb gave a day to day coefficient of reproducibility for Tco of ±1.18 mmol/min/kPa and for Kco of ±0.18 mmol/min/kPa/l.
Discussion
This study has defined the limits of natural variability of routine single breath gas transfer over a 7 day period. Subjects were chosen in whom disease related changes in gas transfer were unlikely during the study period. In addition, standard laboratory practice was used throughout so that the results would be a true reflection of normal laboratory practice.
What is a reasonable interval between measurements when studying reproducibility? Short intervals examine principally short term biological variability—for example, differences in cardiac output—and equipment related variability. They minimise the effects of changing clinical conditions and changing haemoglobin concentration (negligible over short periods). Thus, while studies of intervals of several months may reflect clinical practice more closely, the multitude of possible contributors to change in patients makes interpretation difficult.
Technical factors contribute to gas transfer variability. Hathawayet al 2 described significant differences between Tco measurements made in the same subjects using different equipment. Variability in gas analysis has been recognised as a potential source of variation.16 ,17These variations are most relevant when comparisons between different laboratories are made and internal variability is likely to be lower. Technical variability can be minimised by calibration and by staff training to ensure that the instructions given to patients remain constant. In the current study the gas analysers were calibrated daily and checks of accuracy and linearity were performed weekly.
Patient technique during tests may affect measurements. Breathless or severely obstructed patients may find the single breath method difficult, leading to a reduction in measured inspiratory volume and an underestimate of Tco. Current guidelines require inspiratory volume to be >90% of spirometric expiratory vital capacity11 ,18 or 90–95% of total lung capacity.12 Subjects unable to fulfil this criterion were excluded from the current study. To examine the possible contribution of day to day changes in inspiratory volume to the observed variability, we tested for a correlation between the difference in alveolar volume on the two test days and the difference in Tco. A low but significant positive correlation (r=0.38, p<0.002) was found. Thus, approximately 14% of the variability in Tco can be explained by underlying variability in alveolar volume.
In line with current recommendations,4 ,12 no attempt was made to correct Tco and Kco results for measured haemoglobin concentration. Furthermore, no attempt was made to alter patients' smoking habits as this was felt to be unrealistic in practice. The exhaled CO measurements show that, if this non-restrictive policy is used, patients' CO values vary little from visit to visit and will have minimal influence on the test to test variability of gas transfer. Similarly, correcting for ambient barometric pressure had little effect on the test to test variability.
Plotting the study data using the Bland-Altman method (figs 1 and 2) illustrates that variability of Tco and Kco is largely independent of the magnitude of the measurement. This is similar to the findings of Tweeddale et al 19 who showed that the natural variability in FEV1 and VC was independent of the size of the measurement. As for spirometric parameters, the results are important because they invalidate the use of a percentage value to describe the variability of a population. Using a percentage will lead to underestimation of variability in low values and overestimation for high values.
In conclusion, when reporting changes in gas transfer, staff should be aware of the natural variability of this measurement. The observation that this variability is constant over a wide range of measurement means that even large percentage changes in low values of gas transfer may occur by chance. Failure to recognise this may result in inappropriate treatment decisions.
Acknowledgments
The authors thank Jill Lenney, Jill Fallen, Shirley Armstrong, and Vicky Zgardzinski for their help in recruiting volunteers for the study.