Article Text

Abstract
BACKGROUND The aim of this study was to validate exhaled nitric oxide (eNO) values obtained with an alternative off line, single breath, low flow balloon sampling method against on line sampling according to ERS and ATS guidelines in children who could perform both methods.
METHODS One hundred and twenty seven white children of median age 14.1 years, all pupils of a secondary school, participated in the study. They performed the two different sampling techniques at three different flows of 50, 100, 150 ml/s. Additional measurements were done in random subgroups to determine the influence of the dead space air on eNO values obtained off line by excluding the first 220 ml of exhaled air. All children completed a questionnaire on respiratory and allergic disorders and underwent spirometric tests.
RESULTS The off line eNO values were significantly higher than the on line values at all flows. At 50 ml/s the geometric mean (SE) off line eNO was 18.7 (1.1) ppb and the on line eNO was 15.1 (1.1) ppb (p<0.0001). However, when dead space air was discarded, off line and on line values were similar: at 50 ml/s off line eNO was 17.7 (1.0) ppb and on line eNO 16.0 (1.2) ppb. There was a good agreement between off line eNO values without dead space air and on line eNO: for 50 ml/s the mean on/off line ratio was 0.95 (95% agreement limits 0.63 to 1.27). The off line eNO level at 50 ml/s in 80 children with negative questionnaires for asthma, rhinitis, and eczema was 13.6 (1.0) ppb compared with 33.3 (1.1) ppb in the remaining children with positive questionnaires on asthma and allergy and/or recent symptoms of cold (p<0.0001).
CONCLUSIONS In children, off line assessment of eNO using constant low flow sampling and excluding dead space air is feasible and produces similar results as on line assessment with the same exhalation flow rate. Both sampling methods are sufficiently sensitive to differentiate between groups of otherwise healthy school children with and without self-reported asthma, allergy, and/or colds. We propose that, for off line sampling, similar low flow rates should be used as are recommended for on line measurements.
- exhaled nitric oxide
- children
- measurement
- on line sampling
- off line sampling
Statistics from Altmetric.com
Nitric oxide (NO) is produced by a number of cells in the respiratory tract and has been implicated in the pathophysiology of airway diseases.1 ,2 NO can be detected in human exhaled air.3 Exhaled NO (eNO) has been proposed as a non-invasive marker of airway inflammation, especially in asthma.4Recently, attempts have been made to standardise eNO measurement procedures, recommending on line single breath collection of eNO in adults and children from the age of 6 years.5 ,6 An alternative method is off line sampling, which has the advantage that it is independent from the analyser. Subjects perform a single deep expiration against a resistance into an NO inert and impermeable balloon.7 The content of the balloon is analysed for eNO later. Subjects may be studied outside the laboratory so this method is potentially useful for large epidemiological studies or for home monitoring of asthmatic airway inflammation.
Measurement conditions—including expiratory flow conditions, ambient NO, breath holding, previous forced expiratory manoeuvres, and contamination by nasal NO—have important effects on eNO concentrations.5 ,6 ,8 NO in exhaled air is flow dependent, an effect that is most pronounced at low flows.9-11 To date, most off line measurement techniques for children have not taken into account the dependency on rate of flow. We have previously shown in children that, despite lack of flow standardisation, off line sampling in balloons produces eNO concentrations that are reproducible and similar to those measured on line with high flow rates.7 However, we found that eNO discriminates better between different disease states when measured on line with low rates of flow.11 The aim of this study was therefore to compare a modified off line single breath, low flow method with on line single breath measurements in children, and to establish a reference range of low flow, off line eNO values in healthy school children.
Methods
We recruited 127 non-smoking white children of median age 14.1 years (range 12.0–16.1) from a secondary school. They were interviewed with questionnaires on asthma, eczema, and rhinitis, translated and validated from the core questionnaires of the International Study of Asthma and Allergy in Childhood (ISAAC),12 and were asked for recent symptoms of cold. Of these 127 children, 80 had negative questionnaires and did not report symptoms of cold during the 3 weeks before the study. These 80 children were regarded as healthy. The remaining 47 children had positive questionnaires and/or recent colds and will be referred to as “diseased”. The study was approved by the hospital ethics committee and written informed consent was obtained.
EXHALED AIR SAMPLING
Exhaled air was sampled on line and off line. Both sampling methods were performed by all subjects using three different flow rates (50 ml/s, 100 ml/s, 150 ml/s) in random order. All measurements were performed with the children seated and without a noseclip. Between the different manoeuvres a resting period of 2 minutes was maintained for equilibration of resting ventilatory conditions. After the exhaled air sampling procedures all subjects underwent flow-volume curve measurements using a heated Lilly-type pneumotachograph (Jaeger, Würzberg, Germany). Results of forced expiratory vital capacity (FVC) and forced expiratory volume in one second (FEV1) are expressed as percentage of predicted values.13
ON LINE MEASUREMENT
The measurement circuit consisted of a mouthpiece connected to a two way non-rebreathing valve (Rudolph Inc, Kansas City, MO, USA) through which the subjects inhaled ambient air when the ambient NO concentration was below 10 ppb and NO-free medical air when the ambient NO was higher. The subjects inhaled to total lung capacity (TLC) and immediately exhaled, with a constant flow, for as long as possible into a wide bore tube with an in-line flow resistance (20 cm H2O/l/s; Rudolph Inc). A fine bore Teflon tube continuously sampled the exhaled air from a side-port directly after the mouthpiece at 200 ml/min for measurement of eNO. This manoeuvre was performed with three different expiratory target flows of 50, 100, and 150 ml/s. This produced mouth pressures of 4, 7, and 10 cm H2O, respectively. Airflow was measured by a heated Lilly-type pneumotachograph (Jaeger, Würzberg, Germany) mounted after the resistance. A biofeedback display provided visual guidance to help the subject maintain their exhalation flow at the desired level. An end expiratory flow plateau of at least 3 seconds for the different flows was the end point of the measurement. A plateau was defined as a tracing where flow varies less than ±10% around the target flow. All subjects performed this test in triplicate for each target flow. Both the NO signal and the flow signal were fed into a computer at a sampling rate of 20 Hz. Values of NO and flow were obtained by calculating the mean value in defined time intervals of at least 3 seconds using custom made software. Individual mean values of eNO for each target flow were calculated from at least two acceptable manoeuvres.
OFF LINE MEASUREMENT
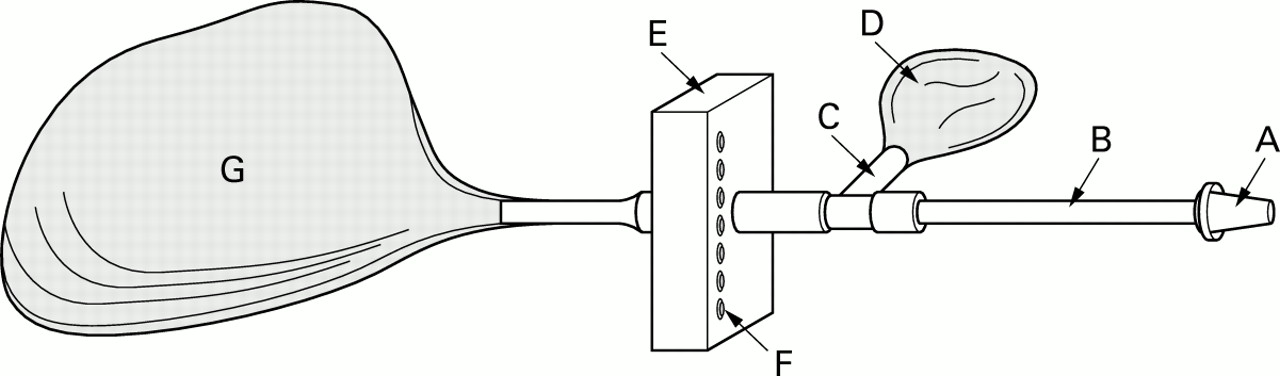
The collecting device consisted of a mouthpiece connected to a rigid perspex tube with a fixed flow restrictor which contained an upstream pressure transducer.14 The signal from the transducer was used to feed an LED display mounted on the tube to enable the subjects to maintain a constant flow (fig 1). Subjects were asked to take a deep breath and to perform one single exhalation with a constant flow into an NO inert and impermeable Mylar balloon (maximum capacity 1750 ml). Children inspired ambient air or NO-free medical air when the ambient NO was 10 ppb or higher. This manoeuvre was performed with three different target flows of 50, 100, and 150 ml/s leading to mouth pressures of 7, 20, and 35 cm H2O, respectively, sufficient to close the velum and prevent contamination with nasal NO.15 A sample of approximately 100 ml was drawn from each balloon in 30 seconds by the sample tube of the NO analyser within 3 hours after collection. Values of off line measurements were calculated as the mean value during these 30 seconds of sampling. We formerly found that NO is stable for at least 6 hours in Mylar balloons.16
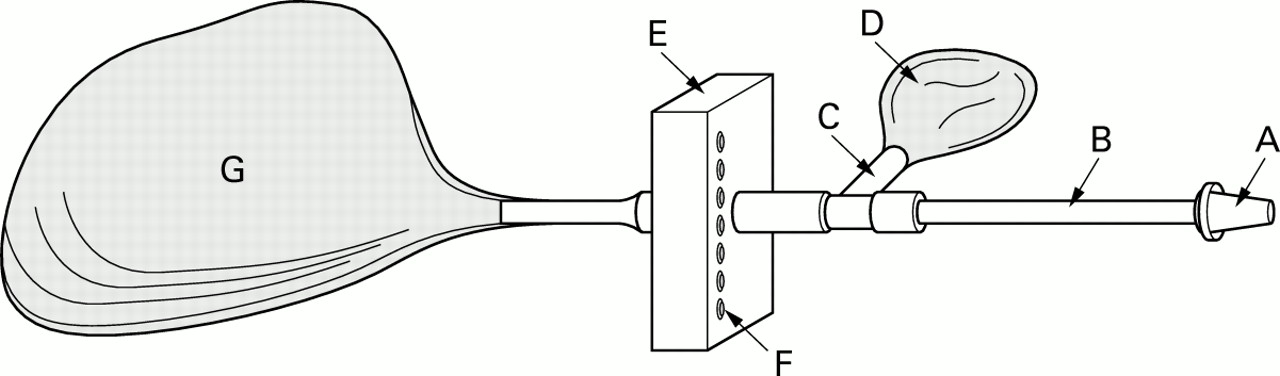
Sampling unit used in the off line collection of exhaled nitric oxide. The mouthpiece (A) is connected to a rigid perspex tube (B) which has a side port (C) with low resistance by which a non-compliant balloon (D) first fills with dead space air. Next, air passes through a small box (E) containing the flow transducer with LED display (F) and an in line flow resistance through which a second balloon (G) fills while oral pressure is raised.
To investigate the influence of the exhaled dead space volume on eNO in balloons we performed additional measurements in a random subgroup of children where we adapted the off line collecting device with a low resistance, non-compliant, small NO impermeable balloon (capacity 220 ml) connected to the exhalation tube upstream of the fixed flow restrictor. The first 220 ml of exhaled air was thus discarded in this small balloon, after which the large balloon was inflated with the remaining part of the exhaled volume. Short term reproducibility of the off line sampling method was assessed in a random subgroup of 15 children who repeated the manoeuvre with a flow of 100 ml/s after a 5 minute interval.
NO MEASUREMENT
NO was measured with a Sievers 280 chemiluminescence analyser (Sievers, Boulder, CO, USA) with a sensitivity of <0.1 ppb and a detection range of <0.1–500 000 ppb. The sample line flow was 200 ml/min, the response time 200 ms, and data were displayed with a lag time of approximately 2 seconds. The analyser was calibrated daily using certified NO gases (100 ppb and 9 ppm) and certified NO-free gas (HoekLoos, Barendrecht, The Netherlands).
DATA ANALYSIS
The results of eNO concentrations are expressed as geometric mean (SE). Because eNO was log-normally distributed, analyses were carried out on log transformed data by using the Student'st test for paired or unpaired data and back transformed. Reference values of eNO for the different target flows in the healthy group are expressed as geometric mean, standard error, and 95% reference interval. The relation between age and FVC, on the one hand, and eNO, on the other, in healthy children was assessed by Spearman's rank correlation coefficient. To analyse the within-subject short term reproducibility the intraclass correlation coefficient (r i) was calculated. Agreement between methods was assessed according to Bland and Altman using the ratios rather than the differences of pairs of observations as appropriate for log distributed values. A two tailed p value of <0.05 was considered significant.
Results
The characteristics of the two groups are shown in table 1. Mean values of FVC and FEV1 were normal for both groups. Both eNO sampling methods were well tolerated and performed by all children. No significant difference was observed in eNO concentrations between girls and boys. In both groups there was no significant correlation between eNO and age or lung function under all different sampling conditions. The off line sampling method was successfully performed by all subjects. With on line measurement, some children failed to blow an acceptable plateau (6–10% of all children for various flow rates). The eNO concentrations at the on line end expiratory plateau are given in table 2. Exhaled NO fell significantly with increasing flow under all sampling conditions in both groups (all p<0.001).
Mean (SE) characteristics of study subjects
eNO concentrations (in ppb) of 100 children of school age measured at three different flow rates on line and off line
COMPARISON OF ON LINE AND OFF LINE METHODS
One hundred children successfully performed the two different sampling methods at the three expiratory flow rates. Their on line eNO concentration was significantly lower than their off line eNO concentration at the same target flow (table 2).
INFLUENCE OF DEAD SPACE AIR ON OFF LINE EXHALED NO
Random subgroups of children performed off line measurements with and without discarding the first 220 ml of exhaled air with an exhalation flow rate of 50 ml/s (n=53) or 100 ml/s (n=22). The eNO concentrations in balloons including dead space air were significantly higher than in those without dead space air: 20.2 (1.1) ppbv 16.8 (1.1) ppb for a flow rate of 50 ml/s and 15.3 (1.1) v 10.1 (1.2) ppb for a flow rate of 100 ml/s (both p<0.001).
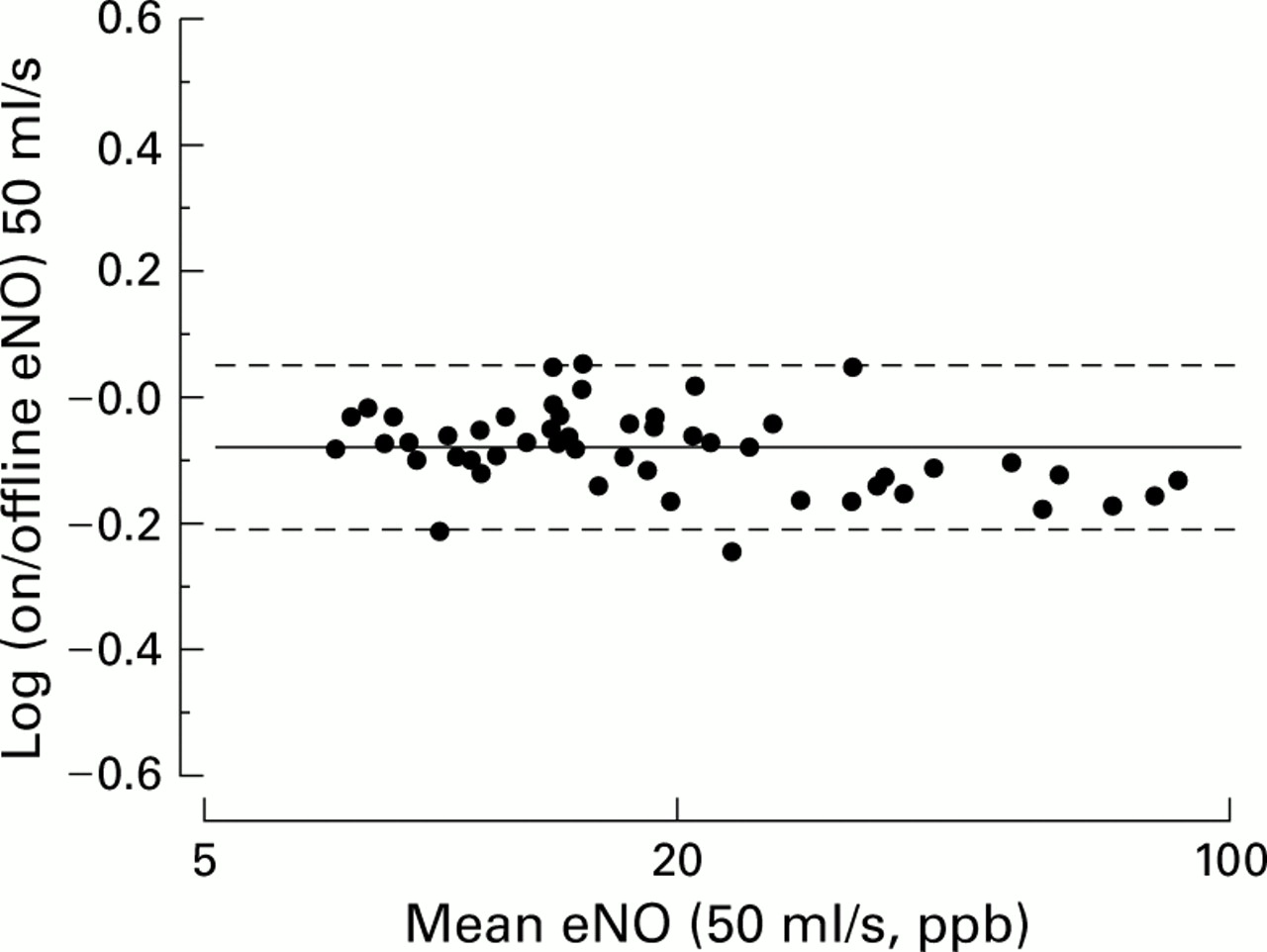
Analyses of agreement between NO values from on line and off line/dead space excluded values according to Bland and Altman, modified for log distributed data, showed a mean log ratio of −0.08 log (95% agreement limits −0.21 to 0.05) for 50 ml/s and −0.36 (−0.66 to −0.06) for 100 ml/s. The ratios were largely independent of the mean values (fig 2).

{kind=link}
{kind=link}
Modified Bland-Altman plot showing agreement of on line and off line (dead space excluded) sampling at flows of 50 ml/s (n=53). The vertical axis depicts the log ratio of on line and off line exhaled nitric oxide (eNO), the horizontal axis the geometric mean of on line and off line values on a log scale. The continuous line is the mean log ratio and the dashed lines indicate 95% agreement limits.
REFERENCE RANGE OF EXHALED NO IN NORMAL CHILDREN OBTAINED ON LINE AND OFF LINE
The eNO values obtained with the different sampling methods and target flows in the healthy group can be used as reference values. The eNO concentrations showed a log normal distribution. Geometric means and 95% reference intervals are given in table 3. Under all the different measurement conditions the children in the “diseased” group (n=47) with positive questionnaires on asthma, eczema and/or rhinitis, and/or symptoms of cold during the 3 week period before the eNO measurements showed a significantly higher eNO concentration than the healthy group (p<0.001). Geometric mean differences between eNO concentrations of healthy and “diseased” groups of children are given in table 4.
Reference values of eNO (in ppb) obtained in healthy children by the different sampling methods, expressed as geometric means (SE; 95% reference interval) in children with negative questionnaires on asthma, rhinitis, and eczema
Differences between eNO concentrations (in ppb) of healthy (n = 73–80) and “diseased” (n = 41–45) children measured at three different flow rates on line and off line
REPRODUCIBILITY OF OFF LINE EXHALED NO
The within-method short term reproducibility of duplicate NO values obtained off line with an exhalation flow rate of 100 ml/s was excellent (r i = 0.94). The mean of all individual coefficients of variation of all eNO values was 6%. Bland and Altman analysis, modified for log distributed data, showed a mean ratio for repeated eNO measurements of 1.03 (95% agreement limits 0.87 to 1.19). This was independent of the mean eNO concentration within the measured range.
Discussion
This study shows that the on line eNO concentration was lower than the off line eNO concentration measured with a controlled low flow balloon sampling technique. However, when dead space air was discarded, agreement between on and off line values was good. Furthermore, we found significant differences in eNO concentrations between children with and without self-reported asthma, allergy and colds, suggesting that our off line method is sufficiently sensitive to detect minor degrees of airway inflammation in groups of otherwise healthy school age children.
The concentration of NO in exhaled air depends critically on the flow of exhalation, an effect that is most pronounced at low flow rates.11 It is therefore desirable to measure eNO concentrations at a constant low expiratory flow rate. Recommendations about the preferred expiratory flow rate are not in agreement.5 ,6 ,9 ,10 A recent ATS task force recommended 50 ml/s for on line measurements for adults as well as for children. For off line measurements in adults and children a target flow of 350 ml/s is recommended.6 However, low flow rates may allow for a better detection of various disease states.9 ,11 Because of the non-uniform flow recommendations, we used three different target flows (50, 100, and 150 ml/s) to compare on line and off line sampling methods and we found a significant flow dependency of eNO in children with both methods. Off line measurement studies of eNO in children have not previously taken flow dependency into account.7 ,17-19
We found that on line eNO values were lower than off line values under all measurement conditions. This seems to be in contrast with results from our previous study in younger children which showed similar eNO values on line and off line with a balloon sampling procedure.7 There are three possible explanations for this discrepancy. Firstly, the former study employed high flow rates of at least 250 ml/s. There is much less flow dependency of eNO with high flow rates and less time for contamination. Secondly, the children in the former study were younger and had a smaller dead space volume than the school children in the present study. The influence of a smaller dead space volume will be less important in a large exhaled volume. Thirdly, the nasal contribution to the dead space air might be less important in young children. With the development and pneumatisation of the paranasal sinuses in childhood, nasal NO levels increase with age. For instance, it was recently shown in a limited number of young children that mixed oral/nasal eNO concentrations collected off line via a face mask in a balloon were similar to eNO values obtained after tracheal intubation.20
The concentration of NO in the airway dead space represents a mixture of ambient NO and upper and lower airway NO which may influence eNO values with off line sampling.5 It is therefore desirable to exclude dead space air with off line sampling. In adults, Parediet al 21 compared on line eNO concentrations obtained with off line flow- and pressure-controlled sampling excluding dead space air and found good agreement between the techniques. The present study extends these observations and shows that exclusion of dead space volume improves the agreement of on line and off line eNO measurements in children in the recommended low flow range.
The on line eNO measurement technique proposed by the ERS5is rather difficult for young children.7 ,22 Canadyet al 22 showed that 24% of children were unable to perform this manoeuvre. In a previous study we found that nearly 30% of children were not able to sustain a stable end expiratory flow plateau employing relatively high flows.7 In the present study only up to 10% of school children had difficulty in obtaining a stable end expiratory plateau at various flows. The expiratory flow rate of 100 ml/s with a corresponding mouth pressure of 7 cm H2O had the lowest failure rate in this study. A likely explanation of the higher success rate of on line sampling in this study compared with our previous study7 is the difference in age of the study populations (median age 14.1 v 11.7 years). In younger children in particular the on line sampling method remains difficult to perform and an alternative methodology should be developed for them.
A source of error in the present study may be nasal contamination, especially with the lowest mouth pressures—for example, 4 cm H2O during on line sampling at 50 ml/s. One could argue that this pressure was not high enough to close the soft palate, potentially leading to nasal contamination. However, a study in adults found no contamination of NO from the nasopharynx with a mouth pressure of at least 3 mm Hg (= 4 cm H2O) using argon as a tracer gas which was applied to the nose and not retrieved in the exhaled air.15 No similar studies have been published for children. Baraldi et al observed no correlation in children between nasal and exhaled NO concentrations using a low expiratory resistance providing a mouth pressure of 3–4 cm H2O.19 Furthermore, in the present study eNO concentrations at flow rates of 100 and 150 ml/s obtained on and off line, and employing higher pressures, suggest no important contamination at lowest flows selectively. This suggests that contamination with nasal air has not introduced a bias.
Interestingly, we found significantly higher concentrations of eNO in children who reported atopic symptoms or recent colds. This suggests that eNO differentiates between healthy children and those who are likely to have minimal airway inflammation but no actual symptoms and normal lung function. We speculate that airway inflammation may already produce a significant increase in the concentration of eNO before giving rise to symptoms.
In conclusion, off line measurement of eNO is simple and feasible in school children. The off line eNO values with constant low flow, excluding dead space volume, show good agreement with on line values. Both sampling methods discriminate between groups of children with and without self-reported asthma, allergy, and colds. Off line sampling offers the possibility of studying eNO independently of the presence of an NO analyser, which could be useful for epidemiological studies and home monitoring of asthma. We propose that off line assessment of eNO should be performed using the same low flow rate of 50 ml/s as is recommended for on line assessment.6
Acknowledgments
The authors are indebted to the pupils and teachers of the “Erasmiaans Gymnasium” in Rotterdam who participated in this study.
References
Footnotes
Funding: This work was supported by research grant 94.14 from The Netherlands Asthma Foundation.