Article Text

Statistics from Altmetric.com
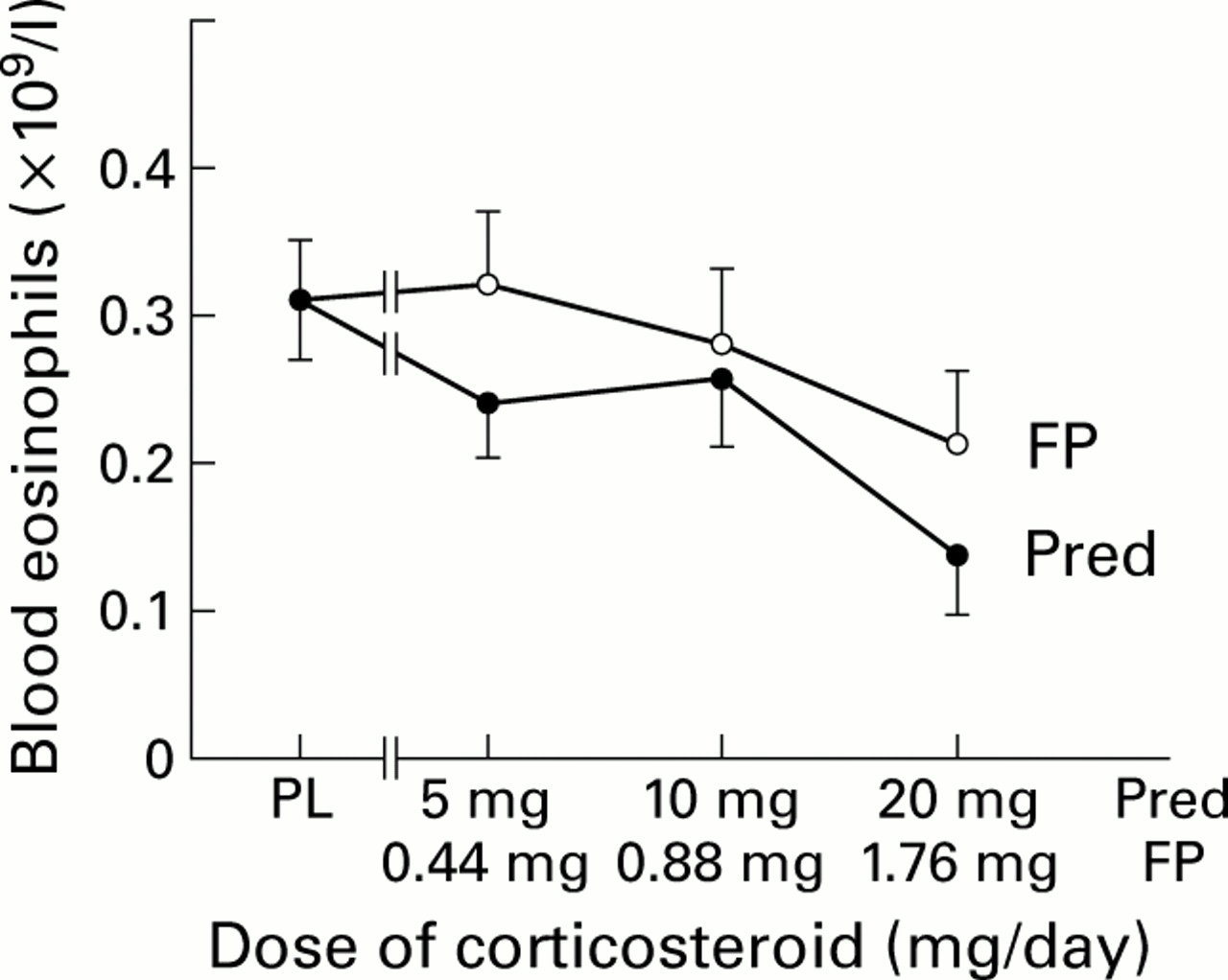
I read with interest the case report by Tuggey and Hosker where Churg-Strauss syndrome was associated with the use of montelukast in an asthmatic patient in whom there was no recent exposure to oral corticosteroid.1 However, it is worth noting that the patient was using a high dose of inhaled fluticasone propionate (1.5 mg/day) via a large volume spacer prior to the introduction of montelukast. In this respect, a large volume spacer has been shown to double the systemic bioavailability of fluticasone propionate compared with a metered dose inhaler, in terms of its propensity for adrenal suppression.2 In a dose ranging study in asthmatic patients a comparison was made between inhaled fluticasone propionate via a 750 ml large volume spacer (Volumatic) and oral prednisolone.3 Regression analysis showed significant (p<0.05) dose-response relationships with both drugs for suppression of peripheral blood eosinophils (fig 1), in keeping with their systemic bioavailability. At the highest doses studied for prednisolone (20 mg/day) and fluticasone propionate (2 mg/day nominal dose) there was a 1.5-fold (95% CI 0.8 to 2.7) greater suppression of blood eosinophils with prednisolone than with fluticasone although, as indicated by the confidence interval (which included unity), this did not represent a significant difference between the drugs. Our data are in keeping with those of Toogood et al who also showed dose related suppression of blood eosinophils with inhaled budesonide and oral prednisolone.4
{kind=link}
Dose response for suppression of peripheral blood eosinophils with inhaled fluticasone propionate (FP) given via large volume spacer and oral prednisolone (Pred) compared with placebo (PL). Significant dose related suppression of eosinophils was accompanied by other systemic bioactivity markers including serum osteocalcin and plasma cortisol. Doses of FP are shown ex-actuator, with 1.76 mg/day ex-actuator corresponding to 2.0 mg/day ex-valve (nominal dose).3
It is therefore evident that a high dose of inhaled fluticasone via a spacer, as reported in the case of Tuggey and Hosker, might have been suppressing the eosinophil count and therefore masking previously undiagnosed Churg-Strauss syndrome prior to starting montelukast. Indeed, it has been shown in a previous meta-analysis of 13 studies that, in terms of relative systemic bioactivity for producing suppression of early morning plasma cortisol, 1 mg inhaled fluticasone is approximately equivalent to 10 mg oral prednisolone.5
The learning point here is that high doses of inhaled corticosteroid may exhibit sufficient systemic bioactivity as a class effect to suppress previously undiagnosed Churg-Strauss syndrome in the same way as low doses of oral corticosteroids. Furthermore, the revised package insert for fluticasone propionate (as Flovent, GlaxoWellcome Inc, Research Triangle Park, North Carolina, USA) now has an insertion in the section on precautions and adverse reactions stating that “in rare cases patients on inhaled fluticasone propionate may present with systemic eosinophilic conditions, with some patients presenting with clinical features of vasculitis consistent with Churg-Strauss syndrome. These events usually but not always have been associated with the reduction and/or withdrawal of oral corticosteroids following the introduction of fluticasone propionate. A causal relationship between fluticasone propionate and these underlying conditions has not been established”. It is also difficult to understand, in the case described by Tuggey and Hosker, how the introduction of montelukast may have precipitated Churg-Strauss syndrome and a peripheral eosinophilia, given that studies have shown montelukast actually to suppress the peripheral blood eosinophil count.6
References
authors' reply We are grateful to Professor Lipworth and Dr Wilson for their interest in our case report. Their main point seems to be that the dose of inhaled fluticasone via a Volumatic might have suppressed the eosinophil count and masked previously undiagnosed Churg-Strauss syndrome before starting treatment with montelukast. Several points can be made against this argument: (1) the blood eosinophil count was normal before the patient received any systemic or inhaled steroids (including fluticasone); (2) there was no dose reduction in inhaled fluticasone before the sudden development of systemic symptoms and profound peripheral eosinophilia; and (3) the features of vasculitis developed very rapidly with a close temporal relationship to the commencement of montelukast therapy.
Professor Lipworth and Dr Wilson also point out that montelukast is normally associated with suppression of the peripheral blood eosinophil count. However, this does not preclude the possibility of an eosinophilic vasculitis developing as a consequence of montelukast therapy.
We read with interest the case report by Tuggeyet al 1-1 of a woman who developed Churg-Strauss syndrome associated with montelukast therapy in the absence of corticosteroid withdrawal. We have recently seen a similar case of a 65 year old man who was admitted acutely to hospital with malaise, general polymyalgia, and weakness associated with a dry cough. He was known to have nasal polyps and asthma for which his general practitioner had started treatment with montelukast 10 mg daily four months previously due to poor control, despite treatment with beclomethasone 400 μg daily. He was not on oral prednisolone and had not received any courses previously. Clinical examination revealed a fever of 37.8°C and generalised muscle tenderness. The rest of the examination was unremarkable. Blood tests revealed a raised white cell count of 15 × 109 /l of which the eosinophil count was 8 × 109/l. The chest radiograph showed left basal infiltration. Discontinuation of montelukast brought about temporary improvement, but he then deteriorated with severe myalgia and paraesthesia in his toes and soles of the feet. Chest examination revealed basal crepitations. The eosinophil count had increased to 13.8 × 109/l and he had moderately positive P-ANCA (titre of 1/160) against myeloperoxidase. The clinical and biochemical tests were in keeping with the diagnosis of Churg-Strauss syndrome which we believe to be associated with montelukast therapy in this asthmatic patient in whom prednisolone had not been previously used. He was started on prednisolone 40 mg/day with prompt clinical improvement and his eosinophil count decreased to 1.5 × 109/l. We would therefore like to reinforce the message of Tuggeyet al that clinicians need to be vigilant in patients developing systemic symptoms after starting treatment with a leukotriene antagonist.
References
- 1-1.↵