Article Text

Abstract
BACKGROUND Exhaled nitric oxide levels are low in patients with cystic fibrosis (CF), despite the chronic inflammation present in the airways. This study aimed to determine whether levels of exhaled nitric oxide were reduced prior to the onset of respiratory symptoms in infants with CF.
METHODS The levels of exhaled nitric oxide were measured using a chemiluminescence analyser in five infants with CF and 11 healthy control subjects, both groups having a mean age of 48.6 days.
RESULTS Mean levels of exhaled nitric oxide were significantly lower in infants with CF than in the control group (4.9 ppb v 12.1 ppb; p=0.01).
CONCLUSIONS This finding may be the key to understanding the inflammatory processes in early cystic fibrosis and may lead to novel treatment approaches.
- cystic fibrosis
- nitric oxide
- paediatrics
Statistics from Altmetric.com
Cystic fibrosis (CF) is one of the most prevalent fatal hereditary diseases in the white population. Chronic progressive lung disease is the major cause of morbidity and mortality. Factors underlying the initiation of lung disease in infants with CF are poorly understood, but it has been suggested that neutrophil inflammation is present before bacterial infection.1 The mechanism for this is unclear.
Exhaled nitric oxide (eNO) has been found to be increased in inflammatory diseases of the airways such as asthma; however, despite the chronic inflammation present in the airway of symptomatic patients with CF, eNO levels are low.2
We aimed to investigate levels of eNO in very young infants with CF in the first few weeks of life, immediately after being diagnosed on neonatal screening, before the onset of respiratory symptoms.
Methods
Infants with CF were diagnosed using a positive neonatal screening test with immunoreactive trypsinogen. They were studied as early as possible, before the onset of any clinical evidence of airway infection. Healthy control infants with no personal or family history of atopy and no previous history of any respiratory illness were studied for comparison.
A customised offline sampling system developed for infants in previous studies was used. This involved a face mask being placed over the infant's mouth and nose which provided a tight seal, and this was connected to a one way, non-rebreathing valve. The infants inhaled nitric oxide free medical air, and mixed expired air was collected into a reservoir bag (Hans Rudolph Inc) during 10 seconds of tidal breathing. The bag was then sealed with a three way tap. Three samples were taken from each infant within a time period of 20 minutes. Nitric oxide was analysed by a chemiluminescence analyser (Model Mk2B, GlaxoWellcome, UK) and the mean value of the three samples was calculated.
Five infants with CF were analysed at a mean age of 48.6 days (range 18–82) and 11 control subjects at a mean age of 48.6 days (range 23–93).
Results
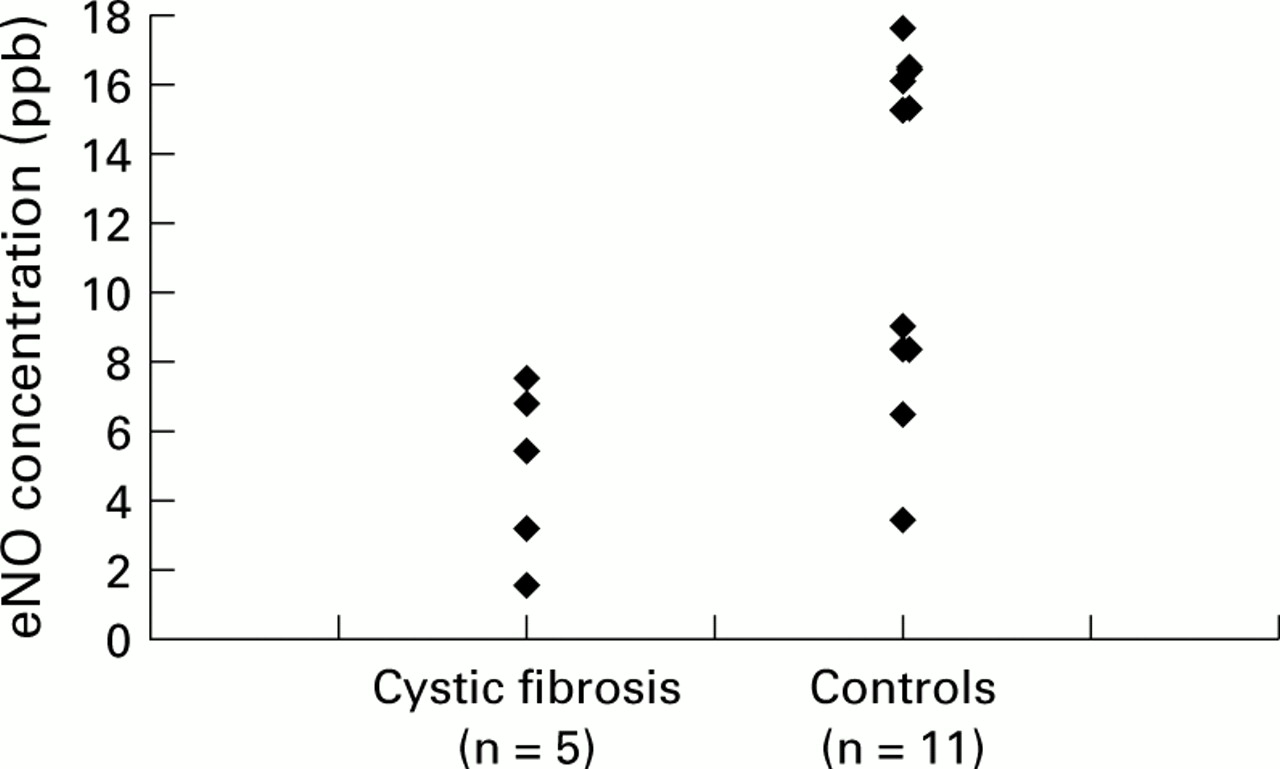
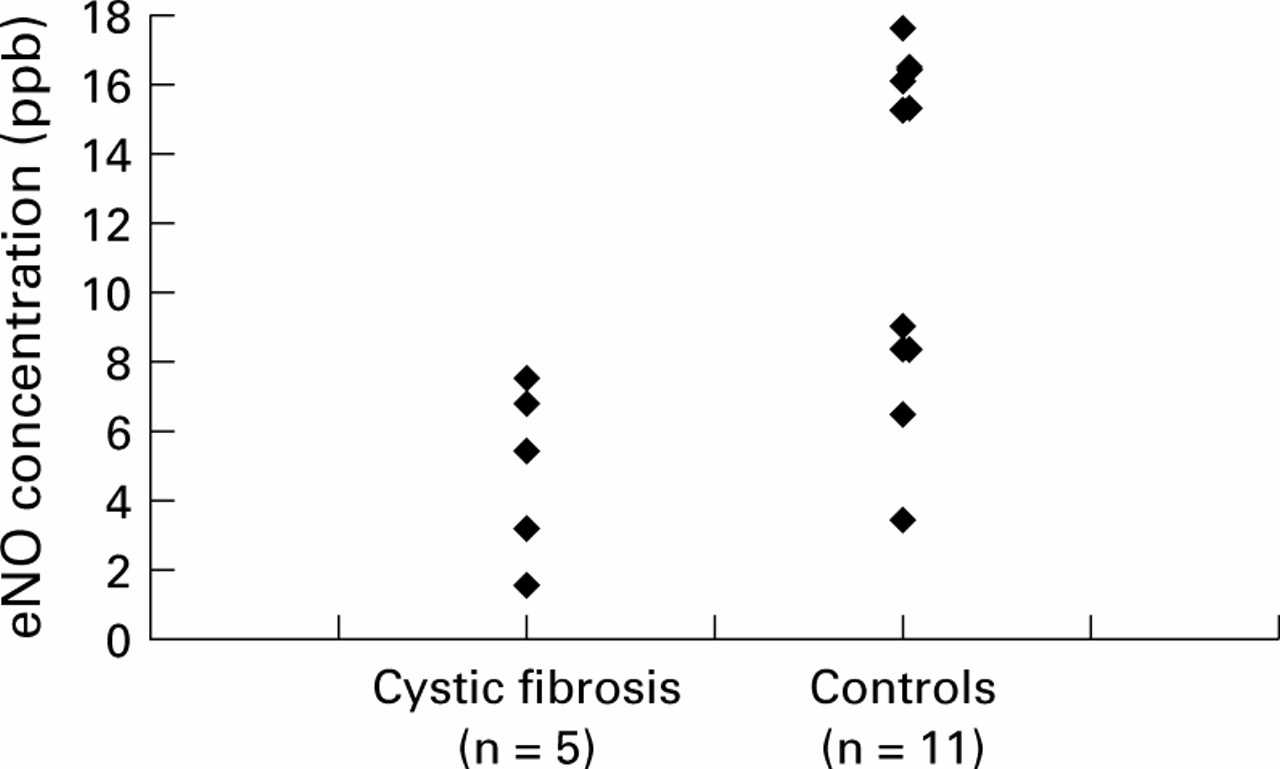
There was a significant difference in eNO between infants with CF and the healthy control group. The mean value of eNO for the CF patients was 4.9 ppb (range 1.6–7.5) compared with 12.1 ppb (range 5.4–15.3) for the controls (p=0.01, Mann-Whitney U test; fig 1).
{kind=link}
Exhaled nitric oxide (eNO) concentrations (ppb) in infants with cystic fibrosis (CF) and healthy controls. eNO levels are significantly lower in the CF group (p=0.01).
Discussion
The finding of lower concentrations of eNO in the CF airway has previously been attributed to diffusion impairment by mucus, or to oxidation of NO to nitrate by reactive oxygen species.3The low values for eNO have been assumed therefore to be due to chronic airways inflammation.
However, recent work has suggested that there is a failure of upregulation of nitric oxide synthase II (NOS II) in patients with CF4 which may be caused by an inherent lack of gene expression related to the CFTR mutation. Our study would support this hypothesis—that is, reduced eNO levels are a primary feature of CF and do not occur as a result of airways inflammation.
If true, we can speculate that the failure of NO release could contribute to the pathogenesis of the airways disease. NO has bacteriostatic properties and has been shown to oppose neutrophil sequestration in the lung.5 An absence or significant reduction in release of NO could reduce the host defences of the airways and lead to early neutrophil infiltration.
Acknowledgments
The authors thank the Action Laboratory Fund and the Astra Foundation for providing funding support for Dr H E Elphick and Miss S Ritson.