Article Text

Statistics from Altmetric.com
Pulmonary emphysema is characterised by permanent enlargement of airspaces distal to the terminal bronchiole accompanied by destruction of alveolar walls. The loss of elastic tissue contained in the interalveolar septa is caused by an imbalance between proteinase and antiproteinase activity, most commonly caused by cigarette smoking. Congenital deficiency of α1-antitrypsin, the most well known antiproteinase, is an important risk factor for the development of premature emphysema. In addition, various other causes have been reported including intravenous drug abuse,1 ,2particularly Ritalin.3 More recently, Johnsonet al 4 reported four cases of bullous emphysema associated with marijuana smoking. We want to report an additional case of severe premature bullous emphysema in a man with a longstanding history of cocaine smoking. To the best of our knowledge, this relationship has only once been reported in the Spanish medical literature.5
A 40 year old man was admitted with progressive dyspnoea, cough, and fever. According to his relatives he had been smoking cocaine (so called “free basing”) for the past 17 years. A reliable history of tobacco smoking could not be obtained because of his respiratory distress and poor level of consciousness. His medical history consisted of recurrent respiratory tract infections. Chest radiographs and computed tomographic scans showed impressive bilateral bullous emphysema with a large air-fluid collection in the right lung, suggesting pulmonary abscess formation (figs 1, 2, 3). Because of progressive respiratory failure he was intubated and mechanically ventilated. Further treatment consisted of intravenous broad spectrum antibiotics (clindamycin and ceftazidime followed by amoxicillin-clavulanic acid) and chest tube drainage because of ventilator associated pneumothorax. The patient eventually died of treatment resistant respiratory failure as a result of pneumonia in the scarce residual pulmonary tissue. Sputum cultures yieldedEnterobacter cloacae andStreptococcus species. HIV infection was excluded serologically. The definitive diagnosis of cocaine induced pulmonary emphysema was established after the concentration of α1-antitrypsin was found to be within the normal range.

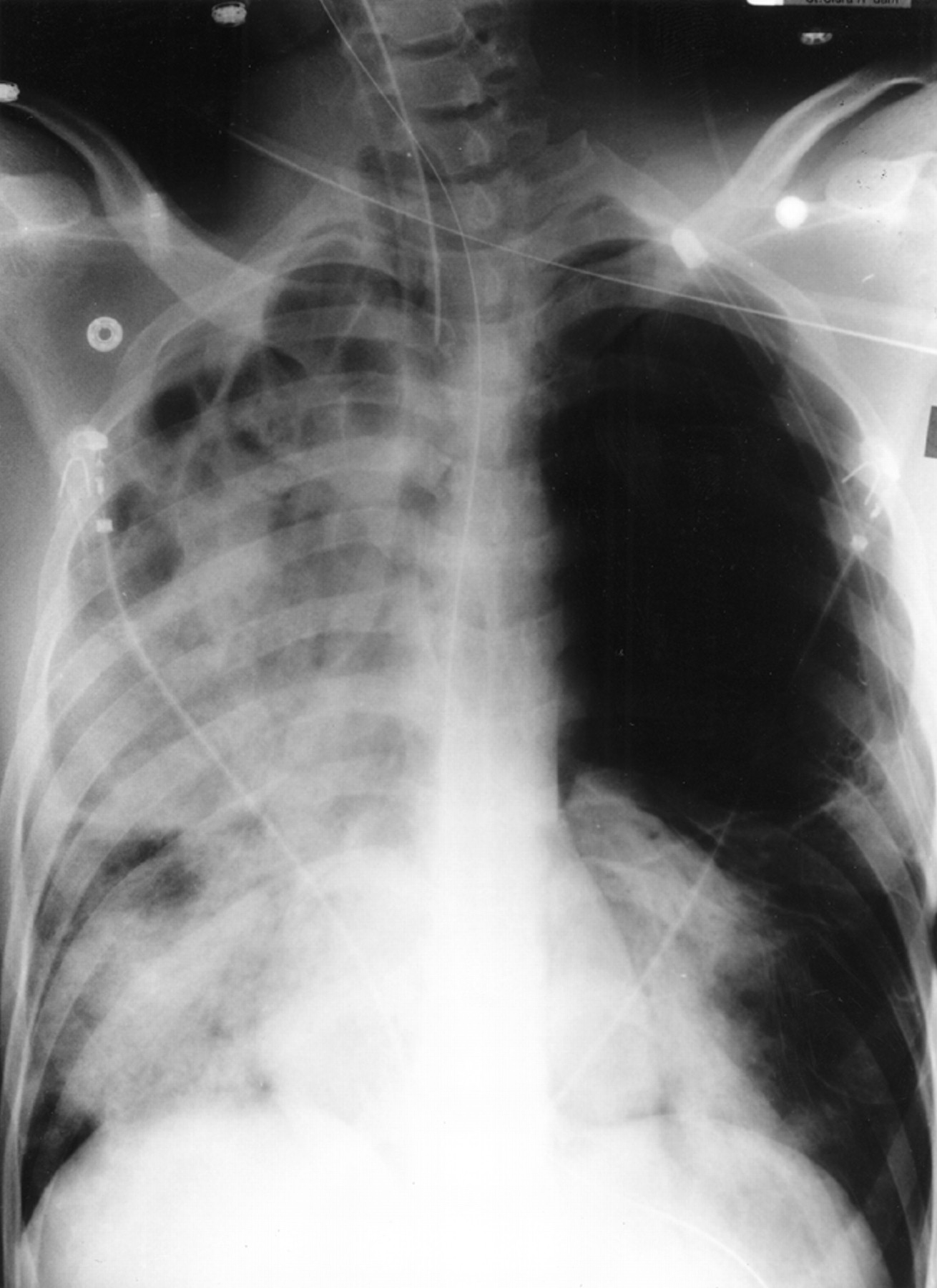
Chest radiograph on admission showing severe bilateral bullous emphysema with a large air-fluid collection in the right lung suggestive of pulmonary abscess formation.

CT scan taken before admission showing bilateral bullous emphysema.

{kind=link}
{kind=link}
{kind=link}
Chest radiograph taken during mechanical ventilation showing a left sided chest tube and infiltrative changes in the scarce residual pulmonary tissue.
Besides congenital α1-antitrypsin deficiency, cocaine smoking should be considered as a possible cause of severe premature bullous emphysema. Abscess formation and rapidly progressive respiratory failure may complicate this condition.