Article Text

Abstract
BACKGROUND This study was designed to establish the number and area (as a percentage) of bronchial wall vessels in subjects with and without asthma, to obtain information on the morphology of the vessels, and to see whether changes differed in patients with mild, moderate, and severe asthma.
METHODS Biopsy specimens were taken using a rigid bronchoscope from the carina of the middle lobe bronchus of 20 patients with allergic asthma and 20 non-asthmatic controls. Specimens were sectioned and stained with haematoxylin-eosin, Masson trichrome, PAS, alcian blue-PAS, and orcein. The vessels were counted and the vascular area was calculated as a percentage in the lamina propria, in blind conditions, on PAS stained sections in 50 microscopic fields (magnification ×1000, 0.02 mm2 per field). The vascular area was calculated using the points counting procedure (Chalkley point array). The vascular morphology, intravascular cells, and the perivascular area were also studied using a magnification up to ×1200.
RESULTS Patients with asthma had more vessels (mean (SD) 226.70 (74.53)v 172.05 (30.58), p=0.0043) and a larger percentage vascular area (8.61 (2.38)% v6.81 (2.25)%, p=0.028) than non-asthmatic subjects. Patients with severe asthma had significantly more vessels than those with mild or moderate disease (p=0.0044). Asthmatic capillaries and venules had oedematous walls and thickening of the subendothelial basement membrane, and hypotrophic or atrophic myocytes and fibrosis in the arterioles. Vessels from asthmatic subjects showed eosinophil recruitment, activation, and intravascular lysis. Intense eosinophil recruitment was associated with more marked vascular structural changes. Muscular formations protruded into the lumen in the arterioles of both groups, and in asthmatics these had hypotrophic or atrophic myocytes and fibrosis.
CONCLUSIONS Morphometric analysis showed that the bronchial lamina propria of asthmatic subjects had a larger number of vessels, occupying a larger percentage area than in non-asthmatic subjects. The number of vessels was correlated with the severity of the asthma. Marked alterations to the vascular structure appeared to be associated with intense eosinophil recruitment and intravascular activation. This is the first report of asthmatic and non-asthmatic bronchial wall specimens containing intra-arteriolar muscular formations, presumably to regulate blood flow to the capillary network and/or sinusoids. This function might be impaired when these structures are remodelled in asthmatic patients.
- asthma
- bronchial vasculature
- eosinophils
Statistics from Altmetric.com
Our knowledge of bronchial histopathology in asthma has grown enormously in the last 10 years, but our understanding of the vasculature is still scant. There are reports of expansion of the vascular bed, endothelial swelling,1 ,2 and endothelial gaps in the postcapillary veins.3 Interest in asthmatic bronchial vessels has been aroused recently in the light of their possible role in asthmatic bronchial obstruction. It has been suggested that expansion of the vascular bed may contribute to bronchial wall thickening and, as a consequence, to bronchial hyperreactivity.4 ,5 Quantitative studies to verify this possibility have given conflicting results. For example, Carroll,6 but not other researchers,7-10found no difference in the total number of vessels and vascular area per mm2 between asthmatic subjects and non-asthmatic controls.
The present quantitative and morphological study was designed to clarify these points and to obtain information on the vasculature in bronchial biopsy specimens from subjects with asthma of varying severity and non-asthmatic controls.
Methods
Patients were premedicated with diazepam (10 mg) and atropine (0.5 mg) and local anaesthesia was induced with xylocaine 2%. Using a rigid bronchoscope, biopsy specimens of adequate size (⩾3 mm) and quality were taken from the carina of the middle lobe bronchus of 20 patients with allergic asthma and 20 non-asthmatic subjects.
STUDY SUBJECTS
Asthmatic subjects
This group comprised 20 subjects (11 men) of mean (SD) age 35.5 (9.8) years (range 20–55) with atopic asthma in accordance with the American Thoracic Society diagnostic criteria11 of differing severity: eight mild (symptoms less than once a day, peak expiratory flow (PEF) >80% predicted, daily variability <20%), six moderate (symptoms every day, PEF 60–80% predicted, daily variability <30%); and six severe (repeated attacks during the day and night, PEF <60% predicted, variability >30%). Their clinical characteristics are shown in table 1. None had chronic obstructive pulmonary disease (COPD) and all had reversibility of >15%. The skin prick test was positive for house dust mite in 18 patients and for pollen in two. The duration of their asthma ranged from <1 year to 23 years (mean 6 years). Patients with mild asthma took β agonists as needed and occasionally theophylline. Those with moderate and severe asthma were taking oral or inhaled corticosteroids discontinuously (in 20–30 day cycles) because of adverse reactions to the drug or a personal dislike of it; they also took aminophylline and β agonists. Corticosteroids were not used in the 10–15 days before bronchoscopy.
Characteristics and vascularity of asthmatic patients
Non-asthmatic subjects
This group comprised 20 subjects (18 men) of mean (SD) age 60.3 (13.3) years (range 23–77) who had no history of either asthma or COPD. Bronchoscopy was indicated for haemoptysis in three cases with normal radiographic findings (normal bronchoscopic findings); four cases with interlobar pleural effusion; and 13 with nodular opacity in the left lung (neoplastic in eight, tubercular in three, not determined in two). The clinical characteristics of this group are shown in table2.
Characteristics and vascularity of non-asthmatic subjects
The study was carried out in accordance with the guidelines of the Declaration of Helsinki and all patients took part voluntarily after giving informed consent.
SAMPLE PROCESSING AND MICROSCOPY
Sections 4 μm thick were stained with haematoxylin-eosin, Masson trichrome, PAS (McManus), alcian blue-PAS, and orcein (Unna) for microscopic examination.
Morphometric study: PAS stained sections were examined blind. A ×100 objective was used with a ×10 eyepiece working on a 160 μm diameter grid field corresponding to an area of 0.02 mm2divided into four sectors by cross lines. The vessels in the lamina propria down to a depth of 160 μm from the subepithelial basement membrane were counted. Ten successive microscopic fields were examined in five histological sections 40 μm apart. This means that, for each patient, 50 microscopic fields were examined equivalent to 1 mm2. The proportion between the vascular and non-vascular areas was calculated with a points counting procedure12 using a ×10 eyepiece on a Chalkley point array grid (G22, Graticules Ltd, Tonbridge, Kent, UK), and a ×100 objective. The grid was placed over each of the 50 fields examined and the sum of the points coinciding with a vessel was used to calculate the total vascular area as a percentage.
Morphological study: the morphology of the vessels, intraluminal cells, and perivascular area was studied at a magnification of ×1200.
STATISTICAL ANALYSIS
Vascular findings in the two groups were compared using one way analysis of variance (ANOVA). The p value for the numbers of vessels was obtained with the t test for independent data, and the Wilcoxon rank sum test was used to compare the percentage vascular areas. One way ANOVA was used to establish the correlation between the number of vessels, the percentage vascular area, and the severity of asthma (mild, moderate, severe); if the result was significant, multiple comparisons were made with the Tukey-Kramer HSD test to see which subgroup of asthmatics was significantly different. A p value of <0.05 was considered significant.
Results
The mean number of vessels in 1 mm2 and the percentage vascular area were both significantly greater in asthmatic subjects than in non-asthmatic controls (table 1). Patients with severe asthma had a significantly higher mean number of vessels than those with moderate or mild asthma (303.7 (76.9) v205.0 (59.5) v 185.3 (29.7), p=0.0044 on logarithmically transformed data). The mean (SD) difference between the percentage vascular areas was 9.7 (1.6)%, 9.1 (2.9)%, and 7.5 (2.2)% in the severe, moderate, and mild asthma groups, respectively (p>0.05). The vascular network was not distributed uniformly in the two groups, its density varying in different subjects and microscopic fields. It was more dense in the lamina propria and sparse between the muscle bundles. Most of these vessels were capillaries and venules whose lumen was no more than 40 μm in diameter. There were sinus veins in the lamina propria and/or submucosal layer of two asthmatic and six non-asthmatic subjects; their diameter was 50 μm or more and their walls were thin and irregular. Only one sinus vein of diameter 160 μm had isolated myocytes in the wall.
Asthmatic subjects had numerous capillaries immediately beneath the subepithelial basement membrane, often (in 10 cases) consisting of only one endothelial cell. The capillary and venule endothelial cells were swollen and protruded into or were free in the lumen, 4.8–6.4 μm thick at the site of the nucleus (13 cases). The subendothelial basement membrane was thickened in 12 cases, and in nine the perivascular structures showed wide gaps between the collagen fibrils as in oedema (fig 1).

Bronchial biopsy specimen from an asthmatic subject showing a dense vascular network in the lamina propria, numerous capillaries immediately beneath the subepithelial basement membrane, thickening of the subendothelial basement membrane, and perivascular oedema. Stain: PAS; original magnification ×200.
In the lumen of the 4534 vessels examined from the 20 asthmatic subjects (table 1) there were 112 neutrophils in 1 mm2, 8.9% of them adhering to the endothelium. Numerous capillaries and venules from seven asthmatic patients contained isolated or clustered eosinophils, frequently adhering to the endothelium, with coarctated nuclei. In one patient with severe asthma the intravascular eosinophils had vacuoles, with cell lysis and clusters of free extracellular eosinophil granules (Cfegs) in the lumen of the venules and capillaries (fig 2). There were also eosinophils infiltrating the oedematous walls of microvessels and perivascular tissue, frequently with a non-lobated nucleus. Four of the asthmatic subjects had isolated intravascular basophils, nine had perivenular lymphomononuclear infiltration, and three had perivenular fibrosis.
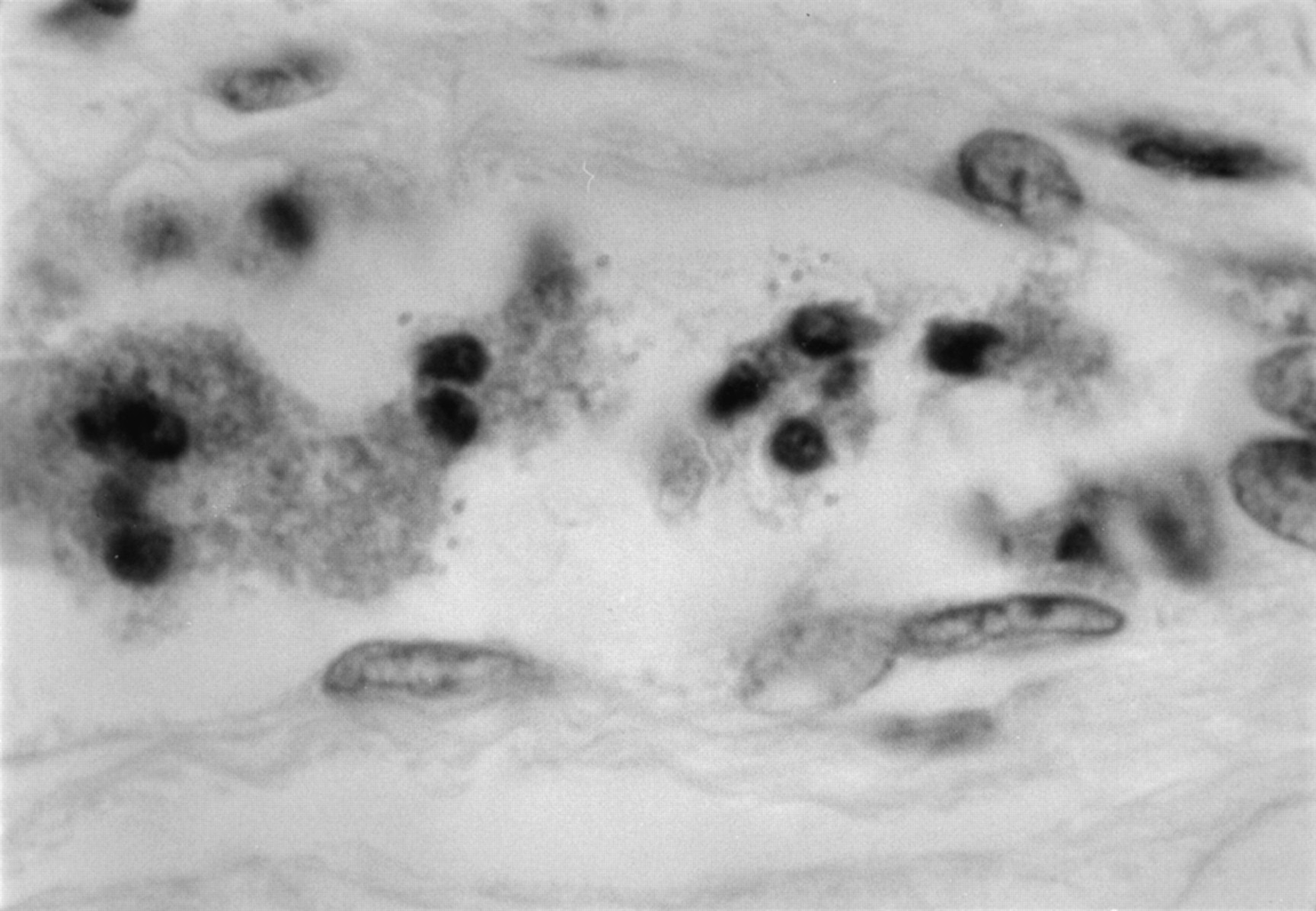
Intravascular eosinophil cytolysis and Cfegs. Stain: H & E; original magnification ×1000.
Non-asthmatics had fewer capillaries in contact with the subepithelial basement membrane; endothelial cells were fine and only exceeded 3–4 μm in two cases. In the 3441 vessels counted in 1 mm2 from these subjects (table 2) there were 165 neutrophils, 9% of which were adhering to the endothelium. None of the non-asthmatic samples had intravascular eosinophils, although one had rare intravascular basophils. Both groups had mast cells close to or in actual contact with the vessels; these cells were usually elongated and some had ramifications on the vessel wall.
Arterioles were rare but were more numerous in asthmatic patients than in controls. The internal elastic lamina extended into the arterioles of about 10 μm diameter. The tunica muscularis consisted of layers of myocytes arranged in circles, with about one layer every 20 μm internal diameter. In vessels from asthmatic patients these were atrophic or hypotrophic with sclerohyalinosis, particularly in two patients with intense eosinophil recruitment.
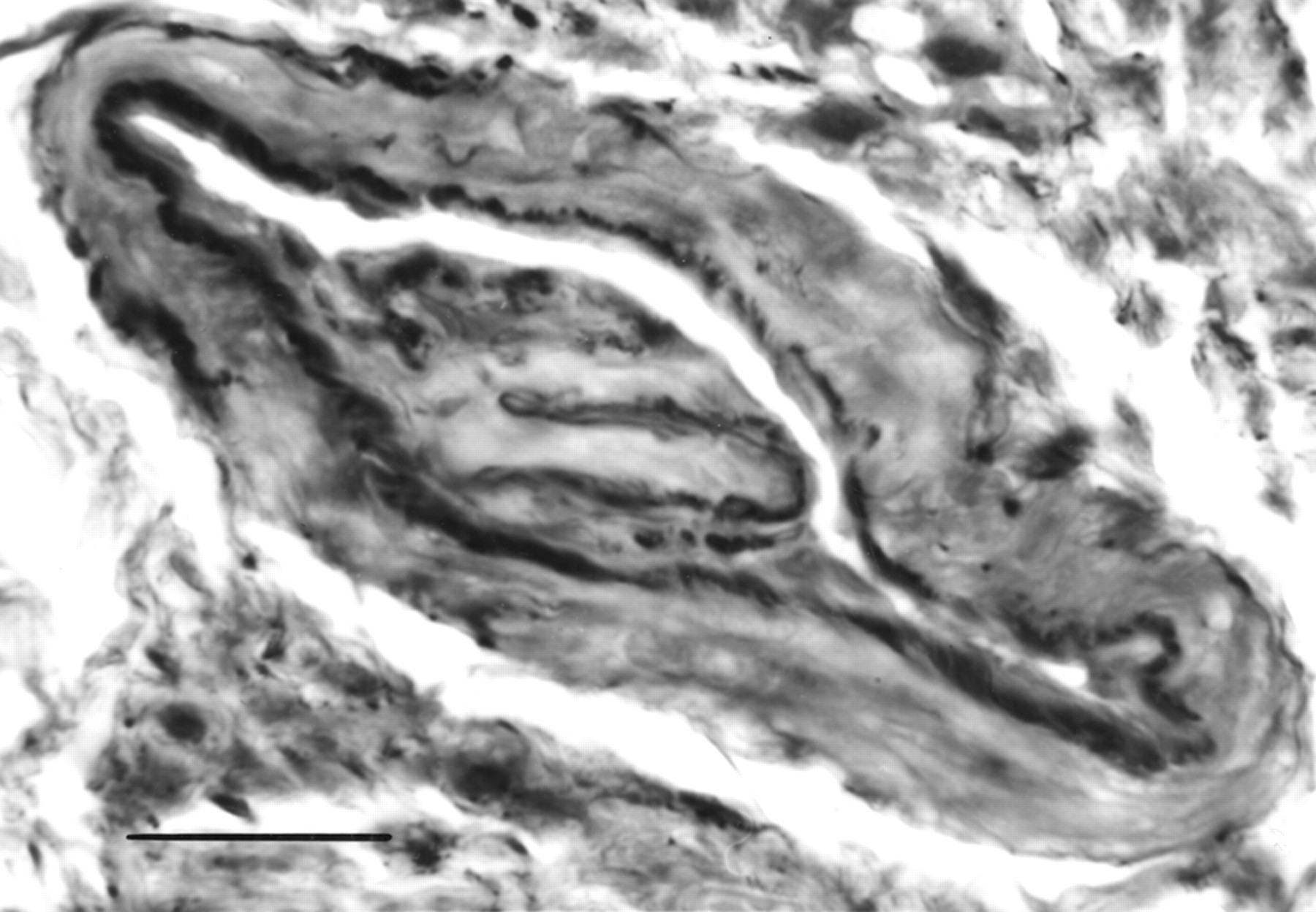
Periarteriolar sclerosis was common in the patients with asthma. An arteriole in one non-asthmatic patient (no 39) and in four with asthma (nos 1, 9, 10, and 20) had muscular protrusions into the lumen which differed in appearance. In the non-asthmatic patient the arteriole had sphincters of muscle fibres wrapping the vessel outside the internal elastic lamina. In the four asthmatic patients the protrusions looked like muscular thickening of the intima and were of two different patterns. The first comprised broad muscular cushions growing out into the lumen from a wide base on the intima. The internal elastic lamina was split at the end of these cushions and the outer abluminal layer was continuous with the circumferential internal elastic lamina while the other layer extended along the surface of the cushions under the endothelium. The cushions consisted of longitudinal and oblique smooth muscle fibres (patients 1 and 9, figs 3 and 4). The second type looked like pyramids or pillars of muscle inside the internal elastic lamina. They were about 10–12 μm high and wide and consisted of longitudinal smooth muscle fibres (patients 10 and 20). Both types were seen in arterioles of asthmatic patients, with hypotrophy or atrophy of the myocytes and very evident sclerohyalinosis in one patient with severe disease.

Cross section of an arteriole with a cushion with a wide base on the intima. The arteriolar lumen is open. Stain: orcein elastic; original magnification ×1000. Scale bar = 20 μm.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
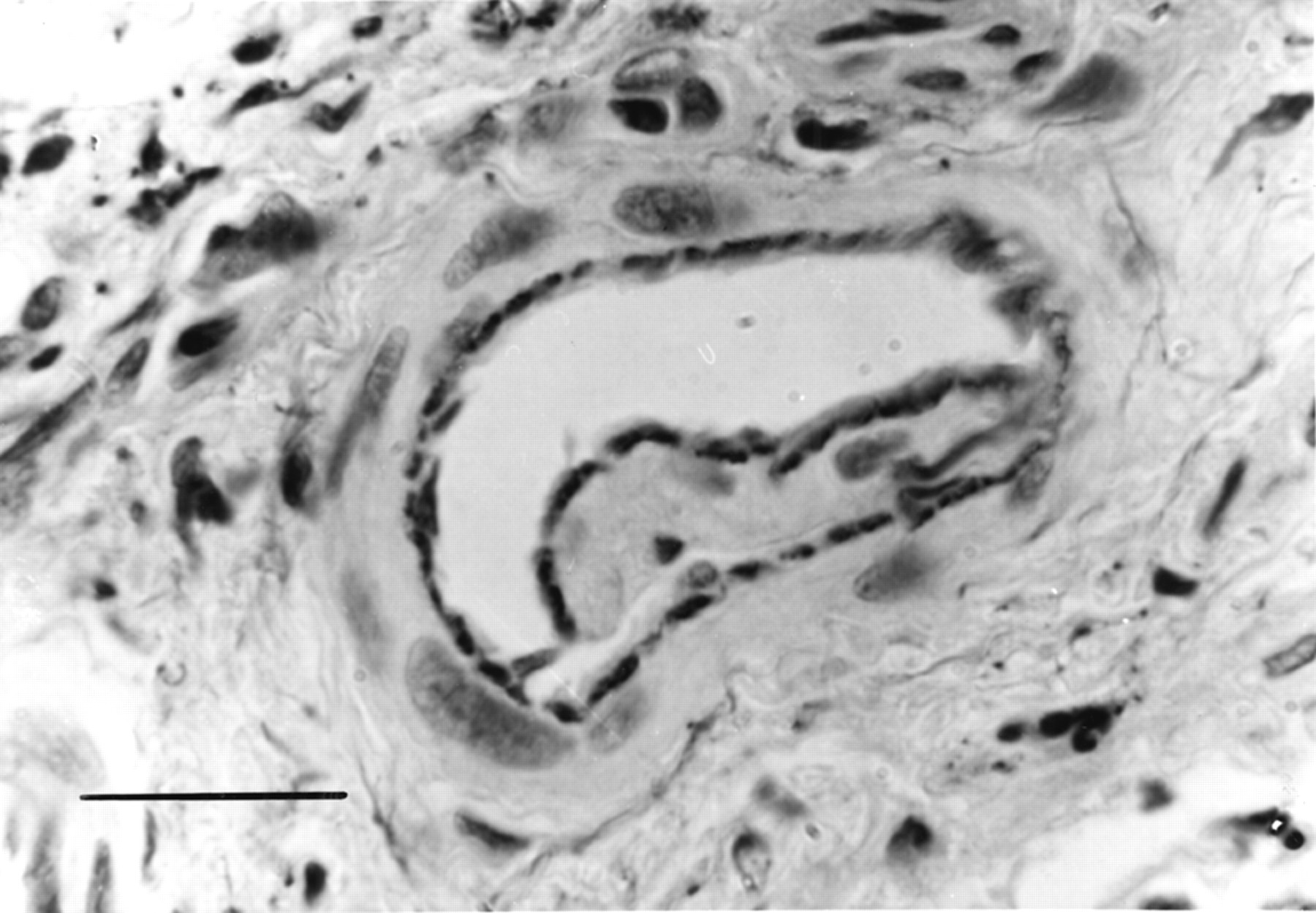
Cross section of an arteriole with a large cushion. The arteriolar lumen is slitlike. Stain: orcein elastic; original magnification ×1000. Scale bar = 20 μm.
Discussion
This study has shown that the lamina propria in patients with asthma is more vascular than in non-asthmatic patients. These findings agree with previous reports7-10 in which, however, the number of vessels and the vascular area as a percentage differed over a wide range. The differences reflect differences in the populations studied, methods, and sampling sites. In addition, quantification of vessels in a given area of tissue is open to criticism because of the various factors than can affect the count: uneven distribution of the vessels, clustering because of the fixation, or the opposite effect—that is, rarefaction because of tissue oedema. Then, too, a particularly tortuous vessel may appear more than once in a section. Even considering all these points, however, significant differences were found between asthmatic and non-asthmatic subjects with regard to the number of vessels and the percentage vascular area.
The bronchial vascular network in patients with asthma consisted mainly of capillaries and venules, with oedema of the walls and only a few arterioles, often with fibrohyalinosis of the walls. The network was rich in the lamina propria but scant among the smooth muscle bundles where there was little inflammatory cell infiltration. Patients with severe asthma had a greater vascular density than those with mild or moderate disease, but their vascular area did not occupy significantly more space. This suggests that the inflammatory process underlying severe asthma induces growth of new vessels which, however, remain so small that they do not significantly enlarge the vascular area.
A typical finding in patients with asthma was eosinophil recruitment, activation and lysis, with Cfegs in the vascular lumen. Cfegs have been reported in the sputum of asthmatic patients but were originally considered an artefact and have only recently been interpreted as a real phenomenon.13 They appear to be the result of allergen induced eosinophil cytolysis, leading to the release of pro-inflammatory toxic granular proteins14 such as eosinophil cationic protein (ECP) which is assayed in asthmatic serum as a marker of eosinophil activation. The origin of ECP in serum is not clear. It has been suggested that it is released in inflamed bronchial tissue and passes from there into the blood, but this contrasts with the poor diffusibility of this extremely charged sticky protein.15 It more likely arises directly in the blood, as is apparently confirmed by the intravascular eosinophil lysis observed in this study. Intravascular eosinophil recruitment and activation were seen in cases with more severe vascular alterations. There was no relation between the vascular changes and the intravascular neutrophils seen in the two groups.
There appears to be no previous report of the muscular formations protruding into the lumen of the bronchial arterioles in one non-asthmatic and four asthmatic patients. In shape and structure these resembled the formations described widely by anatomists as normal in the arterioles of various organs. They are taken to be the morphological substrate for regulating blood flow to the capillary network, which is facilitated or impeded by their relaxing or contracting in cooperation with vasomotion.16-20 We still do not know exactly what purpose these formations in the bronchial arterioles serve, and can only presume that they play a role in regulating the speed and volume of flow to the capillary bed and/or in redistributing blood between the capillaries and the sinus veins in the lamina propria and submucosa.
This quantitative analysis has shown that the greater vascularity of the tunica propria in patients with asthma is related to the severity of their disease. Morphological analysis indicated intravascular eosinophil recruitment and activation as possible factors in the severity of vascular wall changes. The investigation also brought to light muscle structures in the bronchial arterioles that presumably help to regulate distribution of blood to the tissues to enable them to adapt functionally. In patients with asthma this hypothetical regulatory activity may be impaired because of structural remodelling with potential consequences on the distribution and removal of inflammatory mediators,21 thus contributing to maintaining inflammation in the bronchial wall.
Acknowledgments
The author wishes to thank Dr Giulio Serra, Biometrics & Pharmacoeconomics Department, SmithKline Beecham SpA, Milano for statistical analysis.
References
Footnotes
Conflicts of interest: none.
Linked Articles
- PostScript