Article Text

Abstract
BACKGROUND Low attenuation areas (LAA) on computed tomographic (CT) scans have been shown to represent emphysematous changes in patients with chronic obstructive pulmonary disease (COPD). However, the significance of LAA is still controversial in patients with asthma. This study was undertaken to assess the usefulness of lung CT densitometry in the detection of airspace enlargement in association with asthma severity.
METHODS Forty five asthmatic subjects and 15 non-smoking controls were studied to determine the influence of age, pulmonary function, and asthma severity on mean lung density (MLD) and the relative area of the lung showing attenuation values less than –950 HU (RA950) on high resolution CT (HRCT) scans.
RESULTS In asthmatic patients both MLD and RA950 correlated with parameters of airflow limitation (%FEV1, FEV1/FVC, %FEF25–75) and lung volume (%TLC, %FRC, %RV), but not with lung transfer factor (%Tlco, %Tlco/VA). The results of HRCT lung densitometry also correlated with patient age and severity of asthma.
CONCLUSIONS Decreased CT lung density in non-smoking asthmatics is related to airflow limitation, hyperinflation and aging, but not with lung transfer factor.
- high resolution computed tomography
- asthma severity
- lung function
- age
Statistics from Altmetric.com
Asthma is a disease characterised by airflow limitation that reverses spontaneously or in response to treatment.1 The nature of asthma as a chronic inflammatory disease of the airways is well recognised.2 This inflammation process leads to irreversible changes in the airway.3-5 Frequent airway and lung parenchymal changes associated with asthma are considered to be responsible for the irreversibility of airway obstruction, an outcome that is observed in many severe asthmatics. Emphysema, on the other hand, is defined pathologically as a process that results in the increase of distal airspaces with destruction of their walls without obvious fibrosis.6 The evidence for the presence of emphysema in asthmatic patients is controversial.
Numerous studies have demonstrated the usefulness of computed tomographic (CT) scanning and high resolution CT (HRCT) scanning to detect and quantify pulmonary emphysema in patients with chronic obstructive pulmonary disease (COPD),7-19 and a quantitative method using digital data as well as visual assessment of the scan are used to analyse the CT images. Low attenuation areas (LAA) on CT scans in vivo have been shown to represent macroscopic and/or microscopic emphysematous changes in the lungs of patients with COPD.7-12 However, one report has suggested that mean lung density (MLD) gives a good indication of hyperinflation rather than of emphysema.20
Some studies have investigated the use of CT lung densitometry in non-smoking asthmatic patients.21-24 One study suggested that the percentage of pixels below –900 Hounsfield Units (HU) at full expiration reflects air trapping in asthmatic patients and correlates with pulmonary function.21 Gevenois et al showed that acute expiratory airflow limitation and chronic hyperinflation did not influence the MLD or the relative area of the lungs showing attenuation values less than –950 HU (RA950) in non-smoking asthmatic patients.22They also found that CT lung densitometry was influenced by the total lung capacity (TLC) and age in healthy subjects. Biernackiet al observed that some patients with chronic stable asthma develop a reduction in CT lung density.23 In a previous study we reported that the MLD and RA950 correlated significantly with the forced expiratory volume in 1 second (FEV1), but not with the transfer factor for carbon monoxide (Tlco) in 10 non-smoking asthmatic subjects.24 However, to our knowledge, the relationship between the findings of CT lung densitometry and asthma severity has not been studied.
The purpose of this study was to evaluate the use of HRCT lung densitometry in detecting distal airspace enlargement in asthma. We investigated the influence of age, pulmonary function tests, and asthma severity on the results of HRCT lung densitometry. We examined MLD and RA950 by HRCT scanning and correlated the findings with lung function in 45 asthmatics and 15 healthy non-smoking controls.
Methods
SUBJECTS
Forty five asthmatic subjects (27 women) of mean (SD) age 60.0 (12.1) years (range 24–80) and 15 normal subjects (10 women) of mean (SD) age 64.2 (10.4) years (range 44–79) were recruited from Misasa Medical Branch. Asthma was diagnosed according to the definition proposed by the American Thoracic Society.25 All subjects with asthma had episodic symptoms of wheezing and coughing and experienced symptomatic relief and reversible airway response with an accompanying increase in FEV1 exceeding 20% following treatment with β2 adrenergic agonists. None of the asthmatics had a history of clinically demonstrable tuberculosis or allergic bronchopulmonary aspergillosis as defined by the criteria of Rosenberg et al.26 The asthmatic subjects were stable with no changes in asthma symptoms and medication for at least 1 month, except for the use of short acting inhaled β2 agonists. Normal subjects had no chest symptoms with FEV1 >90% predicted. All subjects were lifelong non-smokers. No subjects had a history of upper respiratory tract infection within the month prior to entry to the study. Subjects underwent a chest HRCT scan and pulmonary function tests on the same day.
Patients were classified into three groups based on severity of asthma according to the guidelines of the National Institutes of Health/World Health Organization (NIH/WHO).27 Mild asthma was defined as symptoms occurring less than once a day, night-time symptoms less than once a week, and FEV1 ⩾80% predicted; moderate asthma was defined as patients having daily symptoms, requiring daily use of inhaled short acting β2 agonists, and pretreatment FEV1 of 60–80% predicted; severe asthma was defined as patients having continuous symptoms, frequent exacerbations, limited physical activity, frequent night-time symptoms, and pretreatment FEV1 ⩽60% predicted.
All the asthmatic patients were considered to be stable within the above classification; stability was defined as follows: subjects with mild asthma maintained on a short acting inhaled β2agonist on an “as needed” basis; those with moderate asthma maintained with scheduled medium dose inhaled corticosteroids (beclomethasone dipropionate (BDP) 400–1000 μg daily) and short acting β2 agonist on an as needed basis for daily breakthrough symptoms; and subjects with severe asthma on oral prednisolone and high dose inhaled corticosteroids (BDP 1000–2000 μg daily).
The onset and duration of asthma were established by careful review of patient history and complete physical examination. Atopy was evaluated by a combination of history of allergies, skin tests, and the presence of serum IgE antibodies specific to 12 common aeroallergens including house dust mite, pollens, moulds, and animal danders. Serum specific IgE was measured using the Pharmacia CAP system (Pharmacia Diagnostics AB, Uppsala, Sweden). Atopic patients were defined as those who had a positive skin test and/or the presence of allergen specific IgE.
Informed consent was obtained from all subjects and the study protocol was approved by the ethics committee of our institution.
PULMONARY FUNCTION TESTS
Spirometric tests were performed using a Chestac 33 (Chest Co, Tokyo, Japan). The following measurements were performed on all subjects: forced vital capacity (FVC), FEV1, FEV1/FVC, and mean forced expiratory flow (FEF25–75). Total lung capacity (TLC), functional residual capacity (FRC), residual volume (RV), and RV/TLC were measured using body plethysmography (Autobox 2800, Chest Co, Tokyo, Japan). The carbon monoxide transfer factor (Tlco) and Tlco/alveolar volume (VA) were measured according to the single breath technique using Chestac 33. FVC, FEV1, FEF25–75, TLC, FRC, RV, Tlco, and Tlco/VA measurements for each patient were expressed as a percentage of their predicted values according to the prediction equations of the Japanese Society of Chest Diseases.28
COMPUTED TOMOGRAPHY
Each patient underwent a non-contrast HRCT scan using a Toshiba Xpeed scanner (Toshiba, Tokyo, Japan) with 2 mm collimation, scanning time of 2.7 seconds, voltage of 120 kVp, and current of 200 mA. All HRCT scans were performed in supine patients following maximal inspiration. The images were reconstructed on a 30 cm field of view (FOV) using a standard algorithm (FC 1). Three HRCT scans were performed for determination of MLD and LAA; an upper section was obtained at the top of the aortic arch, a middle section was taken at the origin of the lower lobe bronchus, and a lower section was taken 3 cm above the top of the diaphragm, as described by Miniatiet al.29
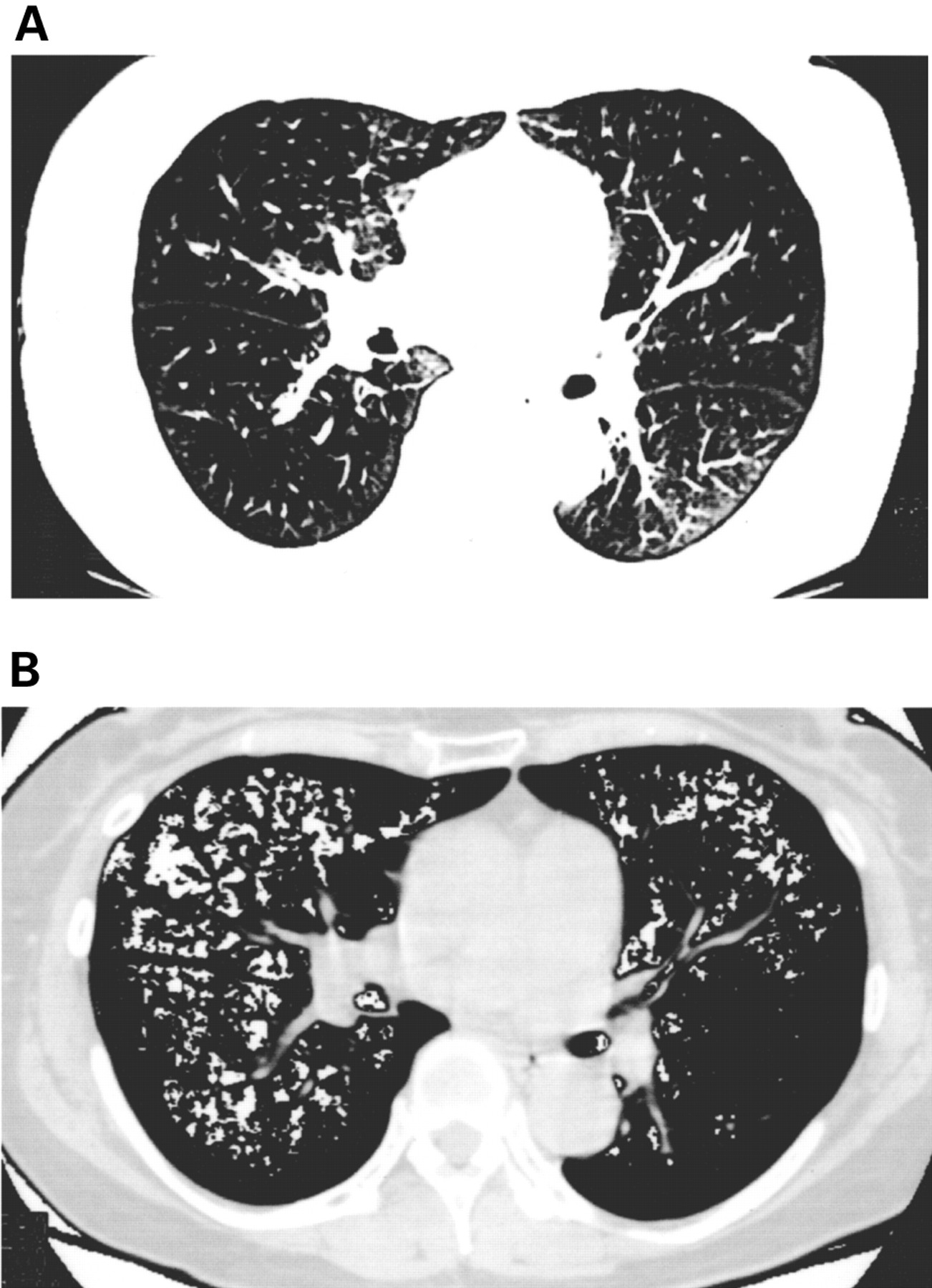
A preliminary study revealed that the density of the lung area was less than –750 HU whereas the density of the chest wall and mediastinum was greater than –750 HU. Using these results, the areas with a density less than –750 HU inside the body were considered to be lung areas. The cut off level between the normal lung density area and LAA was defined as –950 HU because we found that 1 SD below the mean density of the lungs from 15 non-smoking control subjects was –949 HU. An HRCT image and LAA (less than –950 HU) of a representative asthmatic patient are shown in fig 1. The MLD and RA950 were calculated at all three anatomical levels and averaged.
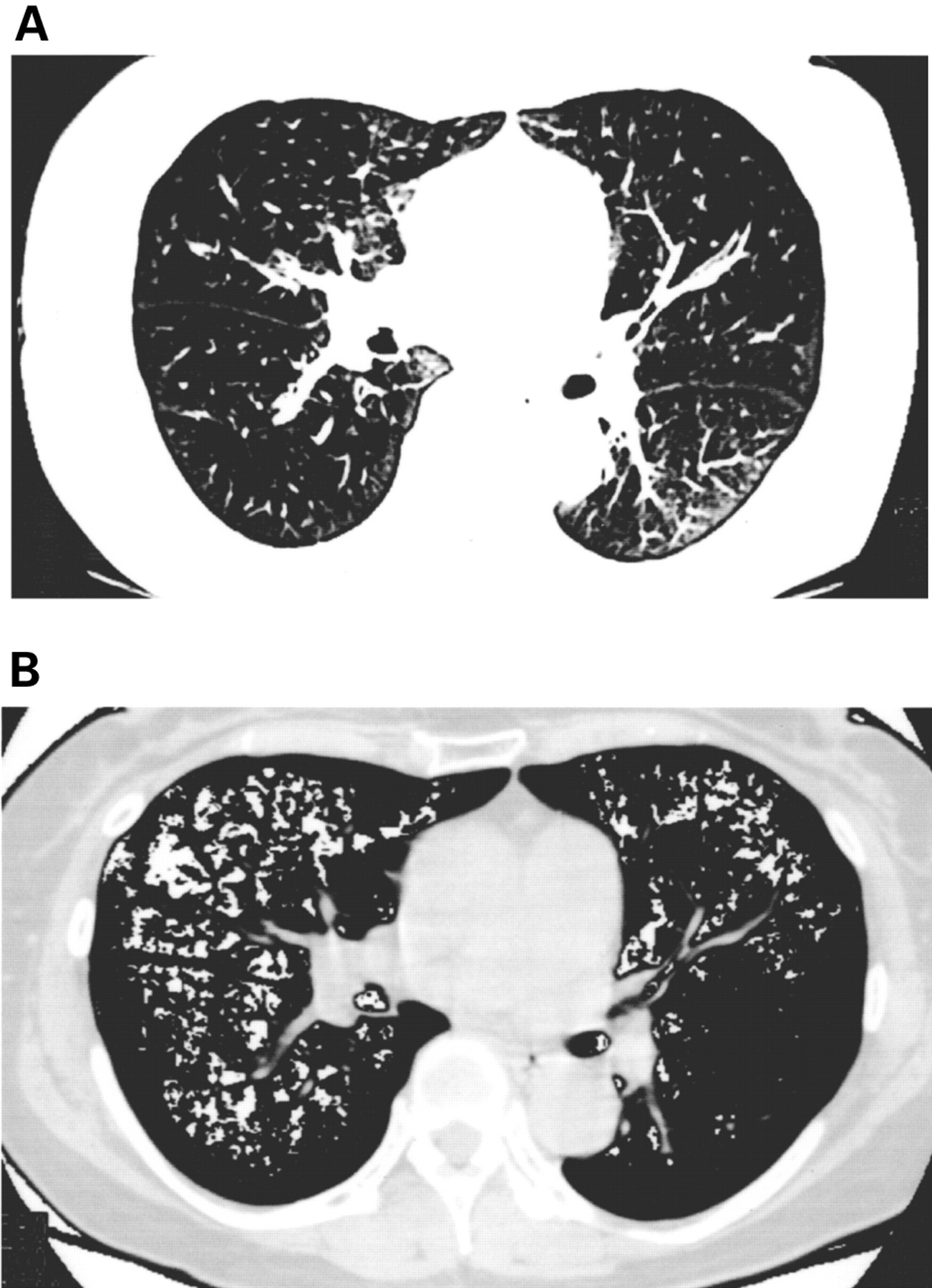
(A) Representative HRCT image of a middle lung section in an asthmatic patient. The mean lung density (MLD) is –906.0 HU and the relative area of the lung showing attenuation values less than –950 HU (RA950) is 15.6%. (B) The same image as in (A) but with the addition of white highlighting of areas with attenuation values less than –950 HU.
STATISTICAL ANALYSIS
The results are expressed as mean (SD). Pearson's correlation coefficients were calculated to determine the relationship between each variable. Stepwise multiple regression analysis was used to evaluate the relationship between the HRCT parameters, lung function, and age. The Mann-Whitney U test and analysis of variance (ANOVA) with Bonferroni/Dunn correction were used to compare groups. A p value of <0.05 was regarded as statistically significant.
Results
PATIENT CHARACTERISTICS
Patient characteristics, lung function tests, and current medications are shown in table 1. There were no statistically significant differences in age or sex distribution between patients with mild, moderate, or severe asthma and control subjects. The duration of asthma and the prevalence of atopy did not differ between the three asthmatic subgroups. There were significant differences in %FEV1 and %FEV1/FVC among the three asthmatic subgroups. The %RV values were significantly higher in those with severe asthma than in control subjects or those with mild asthma. There were no statistically significant differences in %FVC, %TLC, %FRC, %Tlco, or %Tlco/VA between the groups. All asthmatic patients were treated with inhaled β2 agonists. The mean dose of inhaled BDP was 706 μg/day for patients with moderate asthma and 1120 μg/day for those with severe asthma. The mean dose of oral prednisolone, used only in patients with severe asthma, was 6.8 mg/day. Oral theophylline was administrated to patients with moderate and severe asthma.
Clinical characteristics and pulmonary function tests of study subjects
RELATIONSHIP BETWEEN HRCT LUNG DENSITOMETRY AND PHYSIOLOGICAL FACTORS
The relationships between MLD and RA950 and age and pulmonary function tests in the 45 asthmatic patients examined are shown in table 2. MLD correlated significantly with patient age, %FEV1, FEV1/FVC, %FEF25–75, %TLC, %FRC, and %RV but not with %FVC, RV/TLC, %Tlco, or %Tlco/VA. We also found that RA950correlated significantly with patient age, %FEV1, FEV1/FVC, %FEF25–75, %TLC, %FRC, %RV, and RV/TLC but not with %FVC, %Tlco, or %Tlco/VA. However, there was no statistically significant correlation between HRCT findings and %FEV1, FEV1/FVC, or %FEF25–75 in the 15 healthy controls (data not shown). These data suggest that HRCT lung densitometry in asthmatic subjects has significant correlations with patient age and pulmonary function parameters regarding flow limitation and lung volume, but dose not correlate with lung transfer factor.
Correlation (r values) between lung function and HRCT parameters in asthmatic patients (n = 45)
MULTIPLE REGRESSION ANALYSIS
The results of stepwise multiple regression analysis using MLD and RA950 as dependent variables are shown in table 3. The MLD was predicted by the combination of patient age (p=0.0279), %FEV1 (p<0.0001), and %TLC (p=0.0207). The RA950 was also predicted by the combination of patient age (p=0.0411), %FEV1 (p<0.0001), and %FRC (p= 0.0112).
Multiple regression analysis of HRCT parameters using age and pulmonary function tests in asthmatic subjects (n=45)
RELATIONSHIP BETWEEN HRCT LUNG DENSITOMETRY AND ASTHMA SEVERITY
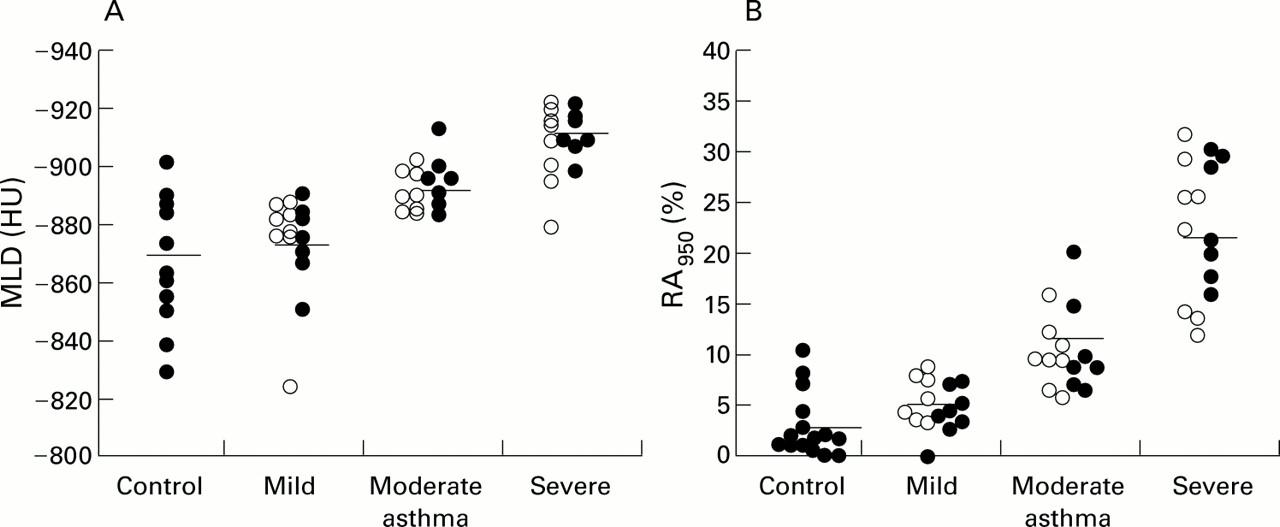
The MLD values for control subjects and patients with mild, moderate, and severe asthma were –867.3 (20.7) HU, –874.8 (17.2) HU, –893.8 (8.1) HU, and –910.5 (11.5) HU. The RA950 was 3.1 (3.2)% in control subjects, 5.1 (2.3)% in patients with mild asthma, 10.2 (3.7)% in those with moderate asthma, and 22.9 (6.6)% in those with severe asthma. Both MLD and RA950 were significantly different between the groups (p<0.001 by ANOVA). There was a significant correlation between asthma severity and MLD or RA950 (p<0.001). However, no significant difference in MLD or RA950 was found between atopic and non-atopic asthmatic subjects with the same asthma severity (fig 2A, B).

{kind=link}
{kind=link}
Relationship between (A) mean lung density (MLD) and (B) relative area of the lung showing attenuation values less than –950 HU (RA950) and the severity and type of asthma. The difference between the four groups was significant by analysis of variance (ANOVA, p<0.001). Open circles = atopic subjects, closed circles = non-atopic subjects. Solid horizontal line = mean.
Discussion
We have examined the relationship between the results of HRCT lung densitometry (MLD and RA950) at maximal inspiration and pulmonary function, patient age, and asthma severity. Our study showed that at least some patients with asthma have decreased attenuation of HRCT lung density which was influenced by age, lung volumes, airflow limitation, and asthma severity, but not by lung transfer factor.
Increases in the LAA of patients with COPD have been reported to reflect the pathological changes of pulmonary emphysema.7-12 The CT measurement of LAA correlates well with transfer factor, a sensitive index of pulmonary emphysema, and measurements of airway obstruction.10-19 ,29 On the other hand, MLD may be linearly related to the fraction of air in the lungs and therefore may not represent the pathological changes of emphysema, given its non-homogenous distribution. Heremans et al found that, in patients with COPD, MLD correlates with pulmonary function indices of airway obstruction and hyperinflation but not with indices that are considered more specific for emphysema (Tlco and static lung compliance).20 It is likely that the relationship between MLD and lung function differs from that between RA950 and lung function.
In efforts to minimise radiation exposure we calculated both MLD and RA950 using three cross sections of the lung (upper, middle, and lower). This was considered adequate as Mishimaet al described an accurate correlation between the percentage of LAA detected from 10 sections (from apex to base of the lung) versus three sections in patients with COPD.19
We used –950 HU as the cut off level between the normal lung density area and LAA. Previous studies have used variable levels ranging from –900 to –960 HU.8-11 ,13 ,14 ,17-19 ,29 ,30 This discrepancy may be attributed to variations between the CT scanning techniques (equipment and reconstruction of images) as well as CT images (conventional v high resolution). Using HRCT scans of 15 healthy controls, we found the mean MLD –1SD to be –949 HU.
We obtained images after deep inspiration. Gevenoiset al reported that inspiratory CT images were more accurate than expiratory images for quantifying pulmonary emphysema.11 They speculated that abnormalities in the expiratory CT scan are more reflective of air trapping than of a reduction in terminal airspace volume. Eda et al 31 found that helical CT images acquired at maximal expiration reflected air trapping whereas CT visual scores at full inspiration showed significant correlation with emphysema. We therefore consider inspiratory CT scans to be more suitable than expiratory CT scans for determining whether emphysema is present in asthma.
We found that both RA950 and MLD strongly correlated with measurements of airflow limitation (%FEV1, FEV1/FVC) and also significantly correlated with indices indicating hyperinflation (%TLC) and air trapping (%RV). RA950 and MLD did not correlate with Tlco or Tlco/VA, two values which have been shown previously to correlate with emphysema.14 ,16 ,32-34 We also found no statistically significant difference in CT lung densitometry between patients with mild asthma and non-atopic controls. However, RA950 increased and MLD decreased significantly with the severity of asthma.
Biernacki et al observed that patients with chronic stable asthma and COPD had a reduction in CT lung density, similar to our results.23 However, they also found that the lowest fifth percentile CT numbers were similar before and after treatment with nebulised β2 agonist, and at the end of an exacerbation and 6 weeks later in five patients with asthma. They concluded that less restricted airflow and diminished chronic overinflation did not affect the lowest fifth percentile CT number. Gevenois et al failed to find any significant changes in RA950 during allergic challenge tests despite a decrease in FEV1 and an increase in RV and FRC.22 The MLD and RA950 of 10 asthmatics with an increased TLC did not significantly differ from those of healthy subjects. They concluded that hyperinflation and airflow obstruction without emphysematous lung destruction does not influence densitometric measurements obtained from inspiratory scans. The difference between the findings of their study and ours may be due to the fact that our subjects are older than theirs.
By multiple regression analysis we have shown that RA950correlates with age, %FRC, and %FEV1, and that MLD correlates with age, %TLC, and %FEV1. Both MLD and RA950 were found to be influenced by age, lung volume, and chronic airflow limitation. Gevenois et alreported that both MLD and RA950 are influenced by TLC and, to a lesser extent, by age in healthy subjects.22 This was further supported by a longitudinal study by Soejimaet al who showed that aging increased airspace abnormalities on HRCT images of non-smoking subjects over a study period of 5 years.35
We found a strong correlation between lung CT density and airflow limitation, a weak correlation with age and lung volumes, and no correlation with transfer factor. The likely reason is that airflow measurements have a wide range whereas age and lung volume measurements have a narrow range. We also speculate that the decreased lung density in non-smoking asthmatic subjects is related to simple gas trapping rather than a significant change in the recoil properties. Further study is needed to examine whether there are significant changes in the recoil properties of asthmatic lungs.
Paganin et al reported a significant increase in the extent of permanent HRCT scan abnormalities with increasing severity and duration of symptoms, both in patients with allergic and non-allergic asthma.36 They further reported that airway remodelling is more common in patients with non-allergic than allergic asthma, even when the duration of disease was similar. They speculated that the anatomical changes in patients with non-allergic asthma were related to advanced age and mechanism of asthma. We observed that RA950 and MLD values were associated with severity of asthma but not with the type of asthma. Our findings may be explained by the fact that our subjects are too advanced in age to show differences between the two groups. Further study is needed to clarify the relationship between asthma type and the results of CT lung densitometry in younger subjects.
We conclude that decreased HRCT lung density in non-smoking asthmatic patients is related to airflow limitation, hyperinflation and aging, but not to lung transfer factor. The decreased HRCT lung density may represent microscopic emphysema or chronic overinflation. We suggest that HRCT scanning may provide useful information about the severity of chronic asthma.
Acknowledgments
The authors thank Mr M Nakai for his technical assistance with CT scanning.
References
Footnotes
No funding in the form of grants, gifts, equipment, or pharmaceutical products was received for this study.
Linked Articles
- Correction