Article Text

Abstract
BACKGROUND Activated T lymphocytes are one of the characteristic features of sarcoidosis. The mechanism of T cell activation, expressing various activation markers including interleukin 2 receptor (IL-2R), has been extensively investigated but the precise mechanism remains unknown. Although thioredoxin (TRX) displays a number of biological activities including IL-2R inducing activity, its role in the induction of IL-2R expression on T cells in sarcoidosis has not been determined. The expression of TRX and IL-2R in granulomas of patients with sarcoidosis has been studied to clarify a possible role for TRX in the induction of IL-2R expression.
METHODS Granulomas in specimens of lung tissue and lymph nodes from five patients with sarcoidosis were immunohistochemically stained with anti-TRX antibody and anti-IL-2Rα chain antibody and the concentration of TRX in the bronchoalveolar lavage (BAL) fluid from 20 patients with pulmonary sarcoidosis was measured.
RESULTS Granulomas in lung and lymph node tissue from patients with sarcoidosis showed strong reactivity with anti-TRX antibody. Positive staining was present in the macrophages, epithelioid cells, and Langhans' type giant cells but not in lymphocytes. IL-2R was expressed on lymphocytes in the same granulomas. By contrast, positive immunoreactivity was not found in lung tissue specimens from 12 control subjects. Concentrations of TRX in BAL fluid were higher in patients with pulmonary sarcoidosis (median (range) 122.6 (20.9–303.3) ng/ml) than in control subjects (32.9 (16.8–52.8) ng/ml, p<0.05).
CONCLUSIONS TRX is highly expressed and is locally produced by granulomas in patients with sarcoidosis. The coexistence of immunoreactive TRX and IL-2R in the same granulomas suggests that TRX might act as a local inducing factor for IL-2R expression on T cells.
- thioredoxin
- sarcoidosis
- granulomas
- IL-2Rα
Statistics from Altmetric.com
Sarcoidosis is a systemic granulomatous disorder of unknown origin characterised by a chronic T lymphocyte/macrophage inflammatory process, granuloma formation, and distortion of normal architecture.1 ,2 It is characterised, at least in part, by the accumulation of activated T lymphocytes and macrophages in the affected organ.1 ,2 The activated T cells are primarily of the CD4 positive phenotype and express various activation markers on their cell surface including interleukin 2 receptor (IL-2R).1-4 Although it has been suggested that activation of CD4 positive T cells is a pivotal step in the events leading to the formation of granulomas in sarcoidosis,1 ,2its aetiology and the precise mechanism of T cell activation at the disease sites are still unknown.
Human thioredoxin (TRX) was initially identified from the culture supernatants of an HTLV-1 infected cell line as an IL-2Rα chain/Tac inducer.5 ,6 Cloning of the cDNA of this factor, ATL derived factor (ADF), showed that it is a human homologue of sulfhydryl reducing enzyme, TRX, first found in prokaryocytes.7 ,8There is increasing evidence that TRX has a variety of biological activities9 including synergism of IL-1 and IL-2 induced proliferation of Epstein-Barr virus transformed B cells,10enhancement of the proliferative response of lymphocytes to IL-2,11 and the binding of several transcriptional factors including AP-1 and NF-κB.12-14 Thus, TRX may play a crucial role in lymphocyte activation including IL-2R expression and proliferation. However, its role in the induction of IL-2R expression on lymphocytes in patients with sarcoidosis has not been determined. We have therefore immunohistochemically stained granulomas from patients with sarcoidosis with anti-human TRX antibody and measured the concentrations of TRX in bronchoalveolar lavage (BAL) fluid to assess the role of TRX in sarcoidosis. We simultaneously stained the granuloma tissue with anti-IL-2R antibody to determine its IL-2R inducing activity.
Methods
STUDY POPULATION
The study group comprised 20 consecutive non-smoking patients with pulmonary sarcoidosis (12 men) of mean age 40 years (range 20–75). The diagnosis of sarcoidosis was established by clinical and radiographic findings and histological evidence of non-caseating granulomas from diagnostic lung biopsy specimens taken by transbronchial, thoracoscopic, or open biopsies. Active sarcoidosis at the time the biopsy specimen was taken was determined by the following criteria1-3 ,15: (1) an increase in lymphocytes in the BAL fluid and an increased CD4/CD8 ratio of lymphocytes in BAL fluid; (2) increased levels of serum angiotensin converting enzyme; and (3) positivity to 67-labelled gallium scan. On the basis of these criteria, all patients in this study were regarded as having active disease; one had pulmonary involvement proved by lung biopsy with normal radiography (radiographic stage 0); eight had bilateral hilar lymph node (BHL) enlargement (stage I); nine had BHL and parenchymal shadowing (stage II); and two had parenchymal shadowing without BHL (stage III). The characteristics of the patients are summarised in table 1. None of the patients had been treated with corticosteroids.
Characteristics of patients with sarcoidosis
For immunohistochemical analysis, histologically normal specimens of lung tissue from eight patients (four men) of mean age 63 years (range 51–68) who had undergone surgery for lung cancer (all patients had adenocarcinoma) and from four patients (two men) of mean age 30 (range 26–48) who underwent surgery for pneumothorax because of localised bulla were used as controls. For the determination of TRX concentrations in BAL fluid, four patients with lung adenocarcinoma (two men) of mean age 57 (range 39–68) and six patients with haemoptysis (two men) of mean age 31 years (range 26–58) were recruited as controls.
Neither the patients nor the control subjects had ever smoked. Informed consent was obtained from all subjects participating in the study.
DESIGN OF STUDY
BAL fluid was obtained by the standard technique. Briefly, the lingula or right middle lobe of patients with pulmonary sarcoidosis was washed with 150 ml saline prewarmed to 37°C. Recovered BAL fluid was filtered through two layers of sterile gauze, centrifuged at 1.500 rpm, and the supernatants were collected and stored at –70°C until assay. BAL fluid was recovered from the opposite side of the lung in patients with localised lung carcinoma. In those with haemoptysis, BAL fluid was recovered from the right middle lobe or lingula after confirming by bronchoscopic examination that there were no abnormalities of the bronchial mucosa.
IMMUNOHISTOCHEMICAL ANALYSIS
Immunohistochemical analysis of TRX and IL-2R expression was performed using the immunoperoxidase technique. Serial tissue sections were deparaffinised in toluene and dehydrated in graded alcohol. Deparaffinised sections were treated with 3% H2O2 in absolute methanol to inhibit endogenous peroxidase for 20 minutes and then incubated with normal horse serum immunoglobulin for 10 minutes to block non-specific antibody binding. The primary antibody was mouse anti-human TRX monoclonal IgG antibody which was established by immunising Balb/c mice with recombinant human TRX (rTRX) (Fujirebio Inc, Tokyo, Japan) for analysis of TRX expression or rabbit anti-IL-2Ra chain polyclonal IgG antibody (Santa Cruz, Santa Cruz, California, USA) for analysis of IL-2Ra. For analysis of TRX expression the sections were incubated for two hours with the primary antibody or the primary antibody that had been pretreated with saturable rTRX for the absorption procedure. For analysis of IL-2Rα the sections were incubated for two hours with the primary antibody or with non-immune normal rabbit IgG as a negative control. Thereafter, the sections were incubated with the secondary antibody (biotinylated and affinity purified anti-mouse IgG) for 30 minutes, followed by incubation with avidin-biotin amplification for 30 minutes, and stained with a solution containing 3-amino-9 ethylcarbazole and 0.15% H2O2.
All the reagents except the primary antibody were obtained from Histostain SP Kit (Zymed Laboratories Inc, San Francisco, California, USA). Counterstaining was performed with haematoxylin. To evaluate TRX and IL-2R expression, two different investigators blindly analysed at least five sections for each case.
MEASUREMENT OF TRX CONCENTRATIONS IN BAL FLUID
TRX was measured by a sandwich ELISA using two monoclonal antibodies (ADF21 and ADF11) which recognised different epitopes of TRX (Fujirebio Inc, Tokyo, Japan). ELISA was performed as described previously.16 Monoclonal antibodies were purified from the ascites of BALB/c mice injected intraperitoneally with hybridoma producing monoclonal antibodies to human recombinant TRX by fractionation with ammonium sulfate precipitation, followed by ABx column (Bakerbond, Mallinckrodt Baker, Philipsburg, New Jersey, USA). ADF21 antibody immobilised plates were incubated with 100 ml of the sample in 100 ml of first reaction buffer (50 mmol/l Tris-HCl buffer, pH 7.5, containing 1.0% bovine serum albumin and 0.1% NaN3) for two hours at room temperature. The plates were washed five times with 0.85%NaCl and were then incubated with 100 ml horseradish peroxidase conjugated ADF11 for one hour at room temperature. After incubation the plates were washed again; 100 ml of substrate solution (150 mmol/l citrate phosphate buffer, pH 4.2, containing 0.2% H2O2 and 0.13% ABTS) was added and incubated for one hour at room temperature. The reaction was then stopped by the addition of 100 ml 1% oxsaloric acid solution and the absorbance at 405 nm was measured in an ELISA reader.
STATISTICAL ANALYSIS
Statistical significance was analysed using the Mann-Whitney U test. A p value of <0.05 was considered significant.
Results
TRX IN SARCOIDOSIS
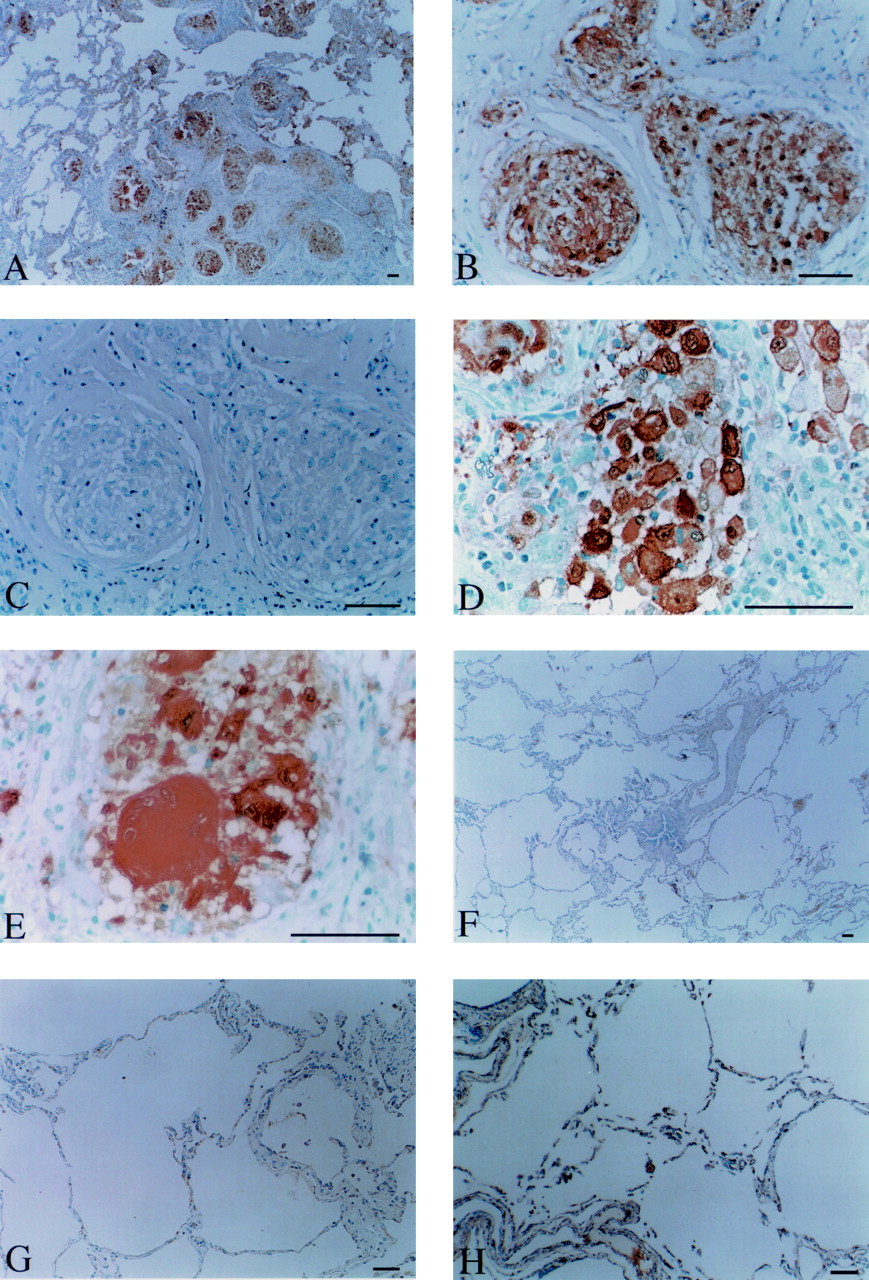
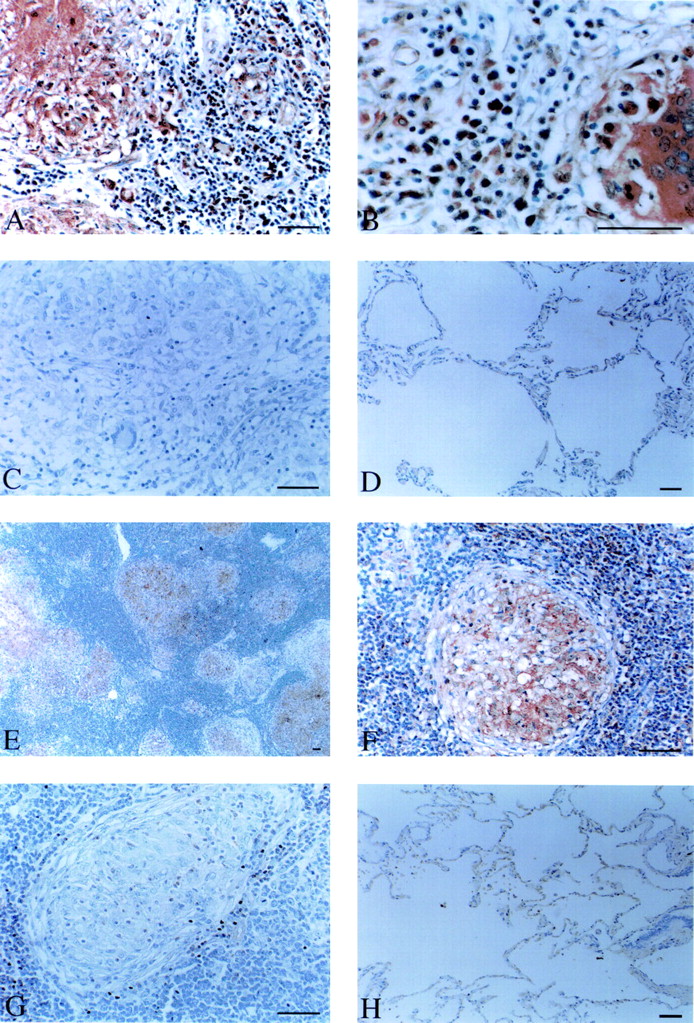
Five specimens of lung tissue and five lymph nodes from patients with sarcoidosis were stained with anti-TRX antibody. Representative results are shown in figs 1 and 2. TRX was highly stained in the granulomas and diffusely stained inside the granulomas of lung tissue specimens (fig 1A and B). Positive staining was present in the macrophages, epithelioid cells, and Langhans' type giant cells but not in lymphocytes (fig 1C and D). TRX was positively stained in granulomas of all other sections. Similar observations were seen in all sections of lung tissue from other patients. Similarly, in the granulomas of lymph nodes from patients with sarcoidosis TRX was highly stained and diffusely stained inside the granulomas (fig 2A and B), and macrophages, epithelioid cells, and Langhans' giant cells were positively stained with anti-TRX antibody (fig 2D and E). TRX was positively stained in the granulomas of all other sections. Similar observations were obtained in all sections of the lymph nodes from other patients. No significant immunostaining was detected in granulomas in the lung tissue and lymph nodes of patients with sarcoidosis when they were stained with anti-TRX antibody that had been preincubated with saturable rTRX (fig 1G and fig 2C), nor was any significant immunostaining detected in histologically normal lung tissue specimens from control subjects stained with anti-TRX antibody (fig 1F, G and H).

TRX expression in the granulomas of lung tissue specimens from patients with sarcoidosis. (A) Low magnification: TRX is highly expressed in the granuloma (original magnification ×40). (B) Higher magnification: TRX is diffusely stained inside the granuloma (original magnification ×200). (C) Reduced immunoreactivity of the granuloma after absorption of anti-TRX antibody with excess human rTRX (original magnification ×200). TRX is positively stained in (D) macrophages and epithelioid cells and (E) Langhans' type giant cells (original magnification ×400). (F) and (G) TRX expression is not found in histologically normal lung tissue from patients with lung carcinoma (controls) (F, original magnification ×40; G, original magnification ×100) nor in (H) histologically normal lung tissue from patients with pneumothorax (controls) (original magnification ×100). Bars = 50 mm.

TRX expression in the granulomas of lymph nodes from patients with sarcoidosis. (A) Low magnification: TRX is highly expressed in granuloma (original magnification ×40). (B) Higher magnification: TRX is diffusely stained inside the granuloma (original magnification ×200). (C) Reduced immunoreactivity of granuloma after absorption of anti-TRX antibody with excess human rTRX (original magnification ×200). TRX is positively stained in (D) macrophages and epithelioid cells and (E) Langhans' type giant cells (original magnification ×400). Bars = 50 mm.
IL-2Rα IN SARCOIDOSIS
Five specimens of lung tissue and five lymph nodes from patients with sarcoidosis were stained with anti-IL-2Rα antibody. Representative results are shown in fig 3. IL-2Rα was positively stained in lymphocytes of granulomas in all lung tissue specimens (fig3A and B) and lymph nodes (fig 3E and F). All sections of lung and lymph nodes from the other patients gave similar results. No significant immunostaining was detected in granulomas of lung tissue and lymph nodes stained with control antibody (normal rabbit IgG; fig3C and G) nor in histologically normal lung tissue specimens from control subjects stained with anti-IL-2Rα antibody (fig 3D and H).

IL-2Rα expression in granulomas of lung tissue specimens and lymph nodes of patients with sarcoidosis. (A) Low magnification: IL-2Rα is highly expressed in granulomas of lung tissue specimens (original magnification ×200). (B) Higher magnification: IL-2Rα is positively stained in lymphocytes (original magnification ×400). (C) Negative control with normal rabbit IgG (original magnification ×200). (D) IL-2Rα expression is not found in histologically normal lung tissue specimens from patients with lung carcinoma (controls) (original magnification ×100). (E) Low magnification: IL-2Rα is highly expressed in the granuloma of lymph nodes (original magnification ×40). (F) Higher magnification: IL-2Rα is positively stained in lymphocytes (original magnification ×200). (G) Negative control with normal rabbit IgG (original magnification ×200). (H) IL-2Rα expression is not found in histologically normal lung tissue specimens from patients with pneumothorax (controls) (original magnification ×100). Bars = 50 mm.
TRX CONCENTRATIONS IN BAL FLUID
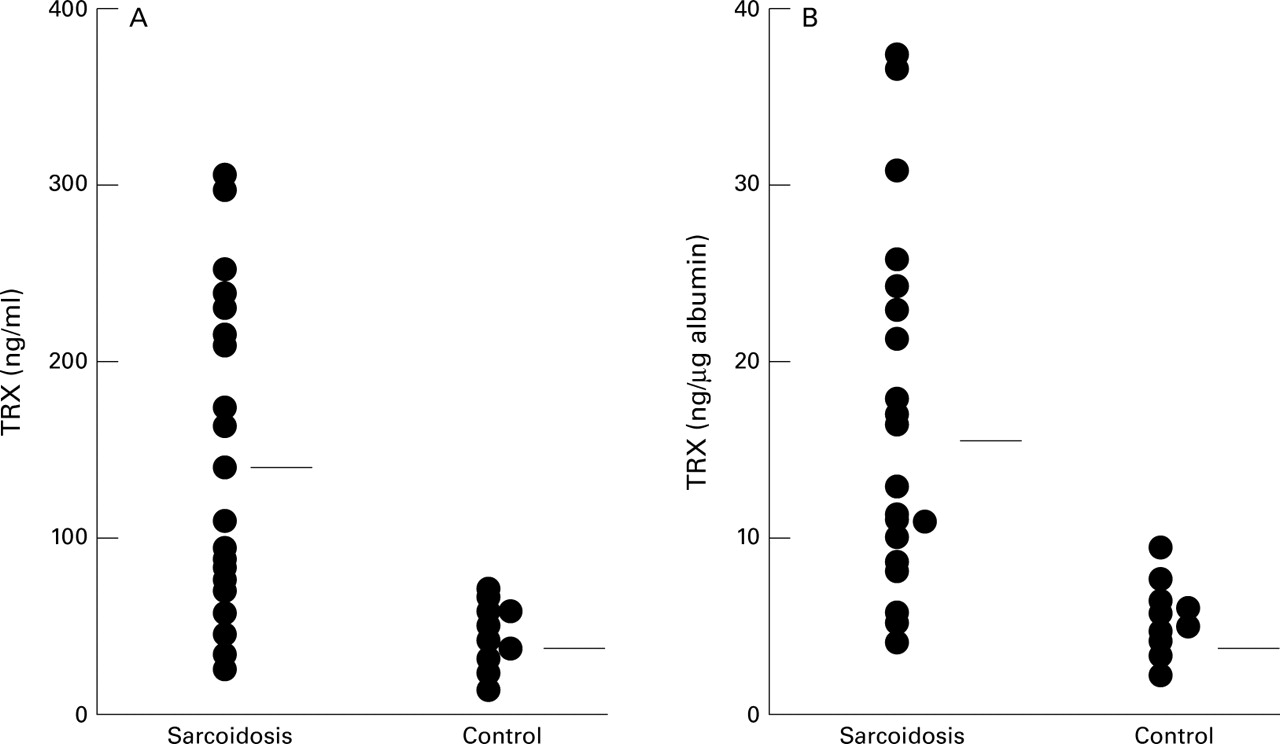
BAL fluid from patients with sarcoidosis contained more TRX (median 122.6 (range 20.9–303.3) ng/ml) than that from control subjects (32.9 (range 16.8–52.8) ng/ml; p<0.05; fig 4A). Similar results were obtained when BAL fluid corrected for albumin concentration was analysed (sarcoidosis: median 15.3 (range 4.3–38.9) ng/μg albumin; controls: 5.2 (range 1.7–9.1) ng/μg albumin; p<0.01; fig 4B). These results indicate that TRX in granulomas is actually secreted in the microenvironment of the granuloma. TRX concentrations in BAL fluid correlated with the absolute number of lymphocytes (r = 0.68, p<0.05), the percentage of lymphocytes in BAL fluid (r = 0.66, p<0.05), and with the CD4/CD8 ratio of lymphocytes in BAL fluid (r = 0.60, p<0.05).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
TRX concentrations in (A) ng/ml and (B) ng/μg albumin in BAL fluid from patients with sarcoidosis and control subjects. The horizontal lines represent median values of each group.
Discussion
Immunostaining with anti-TRX antibody of granulomas in the lung and lymph node tissue of patients with sarcoidosis showed strong reactivity. Positive staining was present in the macrophages, epithelioid cells, and Langhans' type giant cells but not in lymphocytes. IL-2Rα was expressed on lymphocytes in the granulomas. In contrast, positive immunoreactivity was not found in the lung tissue specimens from control subjects. These results show that positive staining of TRX is specific for granulomas from patients with sarcoidosis and that immunoreactive TRX and IL-2R coexist in the granulomas of these patients. In addition, the concentration of TRX in BAL fluid was higher in patients with pulmonary sarcoidosis than in control subjects.
Increased expression of IL-2R on T cells at the site of disease activity is well documented3 ,4; however, the mechanism of induction of IL-2R on T cells has not been clarified. Several mechanisms have been considered. Firstly, macrophage derived cytokines including IL-1 may play a part in the induction of IL-2R expression on T cells since IL-1, which has IL-2R inducing activity,17is reported to be preferentially expressed on macrophages in sarcoid granulomas.18 ,19 Secondly, IL-2 may involve the induction of IL-2R expression since IL-2 per se can induce its receptor on T cells20 and an increased expression of IL-2 on T cells in sarcoid granulomas.21 ,22 Thirdly, antigen presentation to T cells by macrophages may lead to T cell activation resulting in IL-2R induction since antigenic triggering of the T cell receptor has been reported.23 ,24 In any case, the production of cytokines that activate T cells during macrophage activation and activation of antigen presenting cells including macrophages seems to be a pivotal step in the induction of IL-2R expression on T cells. However, the aetiology of sarcoidosis and the mechanism of activation of macrophages are still unknown. In this study we have shown that positive staining of TRX on macrophages and epithelioid cells and positive staining of IL-2R on lymphocytes were present in the same granulomas in patients with sarcoidosis. In addition, the concentrations of TRX in BAL fluid were higher in patients with pulmonary sarcoidosis than in controls. Since TRX has been shown to induce lymphocyte activation including IL-2R expression,5 ,6 these results indicate that local production of TRX may involve the induction of IL-2R expression.
TRX is reportedly a stress inducible protein. Its expression can be induced by a variety of oxidative stresses such as treatment with hydrogen peroxide, x rays and UV irradiation, virus infection, and stimulation with tumour necrosis factor-α.8 ,9 ,25 In addition, the mitogenic stimulation of lymphocytes and the stimulation of macrophages with interferon γ (IFN-γ) induce TRX expression on each cell.26 ,27 We have shown TRX expression on macrophages and epithelioid cells that originated from monocyte lineage—that is, macrophages. There are several possible mechanisms by which TRX is induced on macrophages and epithelioid cells. Alveolar macrophages in patients with sarcoidosis have been reported to release more reactive oxygen species and to express manganese superoxide dismutase.28 ,29 Under these circumstances an oxidative stress inducible protein such as TRX is likely to be induced, while the implication of oxidative stress in sarcoidosis has not been clarified. IFN-γ, which has been described as playing an important part in granuloma formation in sarcoidosis, is positively expressed in these granulomas.19 ,30 It is capable of inducing TRX25 so may play a role in the induction of TRX expression on macrophages and epithelioid cells. However, the precise mechanism of this induction is not known.
We thought it of interest to determine whether the increased concentration of TRX found in patients with sarcoidosis is a result of the disease or a contributory factor to it. We analysed the relationship between TRX concentrations in BAL fluid and the absolute number and the percentage of lymphocytes and the CD4/CD8 ratio of lymphocytes in BAL fluid. The results showed that TRX concentrations correlated with the absolute number of lymphocytes, the percentage of lymphocytes, and CD4/CD8 ratio of lymphocytes in the BAL fluid, indicating a close linkage between TRX concentrations and disease activity. T cells expressed IL-2R which are capable of binding IL-2 and IL-15 proliferate in response to IL-2 and IL-15.31 The accumulation of activated T cells represents the pivotal step in the events leading to granuloma formation. Since TRX has been shown to enhance the proliferative response of lymphocytes to IL-2 and IL-2R inducing activity, increased TRX concentrations may contribute to lymphocyte proliferation. This hypothesis is supported by the correlation of TRX concentrations with the absolute number and percentage of lymphocytes in BAL fluid. Collectively, TRX may act as a contributory factor to the pathogenesis of sarcoidosis rather than a result of this disease. However, further studies are needed to determine whether the increased level of TRX found in patients with sarcoidosis is a result of the disease or a contributory factor to it.
In conclusion, we have found high TRX immunoreactivity in the granulomas of lung and lymph node tissue in patients with sarcoidosis. TRX was prominent in macrophages, epithelioid cells, and Langhans' type cells, and IL-2R was also positively stained in these granulomas. In addition, the concentration of TRX in BAL fluid was increased. These results indicate that TRX, which has IL-2R inducing activity, may play a part in the induction of IL-2R expression on T cells at the sites of disease activity in patients with sarcoidosis. However, the mechanism of induction and the precise role of TRX in sarcoidosis remain to be clarified.