Article Text

Abstract
BACKGROUND Historically, 10 TU has been employed in Australia and the United Kingdom to perform the tuberculin skin test (TST). However, this makes it difficult to compare the rates of TST positivity with other countries such as the USA who use 5 TU. To assess the impact of the dose of tuberculin on the TST a comparison was made of TST responses in health care workers given a TST with both 5 and 10 TU.
METHODS Two TSTs were performed simultaneously in each health care worker using 5 and 10 TU. Each dose was randomly assigned in a blinded manner to the right or left forearm and read at 48–72 hours by a single nurse who was blinded to the assignment of the 5 and 10 TU doses.
RESULTS A total of 128 health care workers were enrolled, 119 (93%) of whom had a past history of BCG vaccination. The overall mean difference in paired reaction sizes for the two doses was 1.5 mm with 95% limits of agreement of –3.6 to 6.5 mm.
CONCLUSION A slightly larger TST reading was seen with 10 TU than with 5 TU. The mean difference of 1.5 mm between the two doses should be considered when comparing rates of TST positivity between countries who use different doses of tuberculin to perform the tuberculin skin test.
- tuberculin skin test
- health care workers
- dosage
Statistics from Altmetric.com
The tuberculin skin test (TST) is the most commonly used test to detect previous Mycobacterium tuberculosis infection, being used in epidemiological surveys, clinical evaluation of patients with suspected active tuberculosis, and assessment for preventive antituberculous drug therapy. Unfortunately the TST has many variables that may affect its interpretation and result. These include variation in tuberculin dose and formulation, experience and technique in application, the effect of previous BCG vaccination, subject age, recent vaccination with live vaccines, and underlying immunosuppression.1
In the 1940s and 1950s the “optimal” dosage of tuberculin was determined. Persons with and without a history of exposure to tuberculosis were tested with increasing doses of tuberculin and the cumulative proportion of reactors was calculated. From these studies it was concluded that 5 TU was the dose that gave the “best” balance between sensitivity and specificity.2
Historically, 10 TU has been employed in Australia and the United Kingdom to perform the TST,3 ,4 while in the United States 5 TU is the standard dose used.5 Because of these dosage differences in performing the TST, comparison of TST results between countries may be difficult. In particular, comparisons of large multicentre TST studies of health care workers in different countries have been complicated by these differences in TST dosage.6 ,7 To assess the impact of the tuberculin dose on the TST we compared the TST responses in a cohort of BCG vaccinated and unvaccinated health care workers who received a TST with both 5 and 10 TU simultaneously.
Methods
Health care workers within the Southern Healthcare Network were informed of the study via table drops and individual mailings. Those who had previous TST readings of 5–19 mm were particularly encouraged to enrol. This was aimed at increasing the likelihood of positive results to both the 5 and 10 TU doses. The upper limit of 19 mm was chosen to decrease the risk of large reactions occurring in individuals who had previously tested positive. Health care workers completed a questionnaire at the time of TST placement documenting age, occupation, and prior BCG status and timing.
TSTs were given by one of two trained personnel. Two TSTs were performed simultaneously in each health care worker using a 5 and 10 TU dose. Each dose was assigned to the right or left forearm based on whether their home address was an odd or even number. To minimise reader variability all results were read by a single nurse who was blinded to the assignment of the 5 and 10 TU doses. The transverse diameter of induration at 48–72 hours was measured by the palpation method.1
The study was approved by the ethics committee of the Southern Healthcare Network.
The results of the 10 TU test were used to assess whether the individual needed further investigation and follow up. According to the Australian and British guidelines, a TST was classified as strongly positive if induration of ⩾15 mm was detected in a person who had previously received BCG and ⩾10 mm in those without such a history.4 ,8 These individuals underwent chest radiography and were offered individual consultation with a specialist physician.
Data were analysed using the two tailed paired samplest test. A residual-like plot of the difference between the measurements against their mean as described by Bland and Altman9 was also employed since this method allows the detection of differences between the two doses at different diameters of induration.
Results
One hundred and twenty eight health care workers were enrolled (102 women) of overall median age 42 years (range 21–65), 119 (93%) of whom had a past history of BCG vaccination (mean number of years since BCG = 26; range 2–47). There were 70 nurses (55%), seven physicians (6%), 12 laboratory workers (9%), and 40 allied health workers (30%). Thirty one had readings for both the 5 and 10 TU doses recorded as zero; the remaining 97 had a least one recordable response for either the 5 or 10 TU dose.
Eight BCG vaccinated health care workers had TSTs of ⩾15 mm with 10 TU and ⩾10 mm with the 5 TU dose. An additional subject without a history of BCG vaccination had TSTs of 10 mm and 11 mm with the 10 TU and 5 TU doses, respectively. All nine individuals had normal chest radiographs and no evidence of active tuberculosis.
Using the USA guidelines10 to determine TST positivity (⩾10 mm regardless of BCG status), 40 (31%) subjects would have been considered positive with 10 TU and 26 (20%) positive with 5 TU. In comparison, using the Australian and UK guidelines4 ,8(⩾10 mm if no history of BCG vaccination; ⩾15 mm if previously vaccinated), eight (0.06%) and seven (0.05%) would have been positive with the 10 TU and 5 TU doses, respectively.
A comparison of the diameter of induration obtained from the two doses is shown in table 1. Most of the health care workers (66%) had a TST of <10 mm. Generally, the 10 TU dose gave a larger TST reading than the 5 TU dose, but in 16 cases (13%) the 5 TU reading was greater. The overall mean difference in paired reaction sizes for the two doses was 1.5 mm (95% CI 1.0 to 1.9; p<0.001). In the 97 health care workers who had a least one recordable TST response to the 5 or 10 TU doses, the mean difference in reaction was 1.9 mm (95% CI 1.4 to 2.5; p<0.001).
Comparison of TST measurements using 5 and 10 TU tuberculin
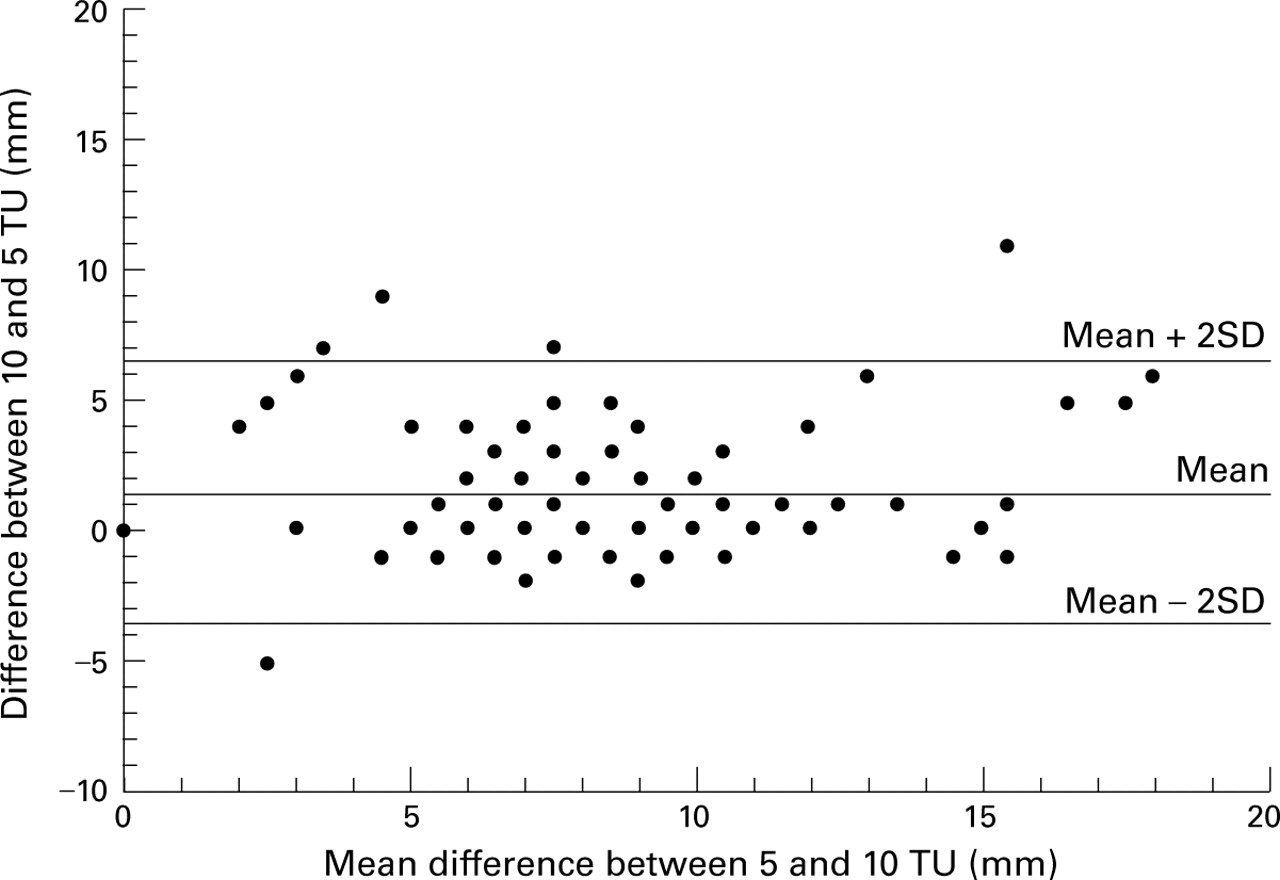
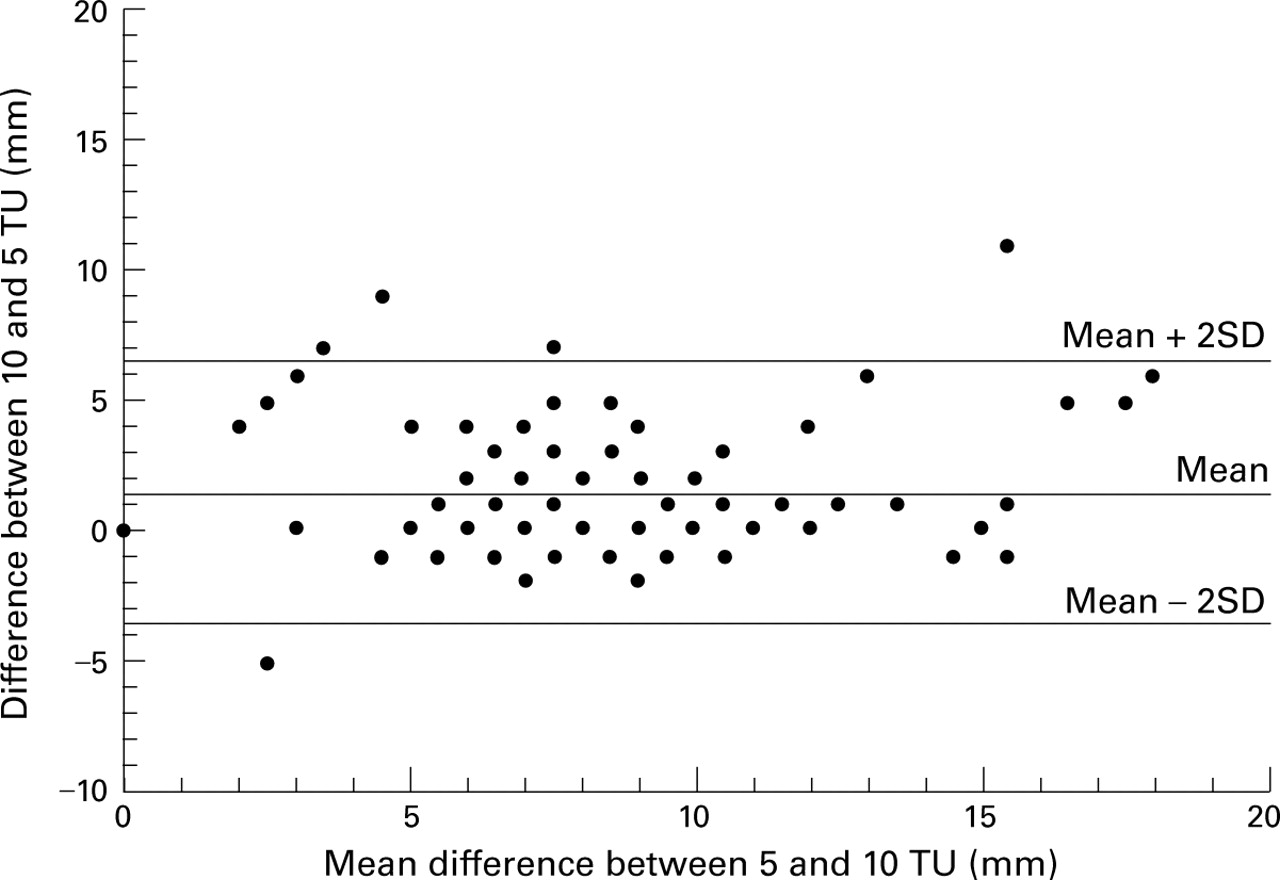
Differences in results between the two doses plotted against the mean of each subject's result are shown in fig 1. Using the Bland-Altman method9 for assessing agreement between the two doses, the 95% limits of agreement were –3.6 to 6.5 mm, meaning that 95% of paired results are expected to have differences within this range. Notably, there was no relationship between this difference in TST response and the mean diameter of induration, suggesting that the difference in 5 and 10 TU results did not change significantly with increasing TST response. There was, however, an association between the mean difference in the results and the age of the health care worker (r = 0.21, p = 0.01), but not with years since last BCG vaccination (r = 0.1, p = 0.29; data not shown).
{kind=link}
Plot of the difference between 5 and 10 TU doses versus mean
Discussion
The tuberculin skin test has long been an important aid in the diagnosis of tuberculous infection and disease. However, different countries use different doses of PPD for screening so that there is no uniformity.3-5 Only one previous study has compared the differences seen when 5 or 10 TU of PPD is employed in the TST.11 However, this 1954 World Health Organisation study assessed a Danish cohort with no history of previous BCG vaccination who received either a 5 or 10 TU TST, but not both doses simultaneously. The average 10 TU TST result was 2–3 mm larger than the 5 TU dose, but the unpaired nature of this study design limited the conclusions that could be drawn from these data.
Our results show that there is a statistically significant but small mean difference of 1.5 mm obtained when the 5 and 10 TU doses are compared within individuals. This small increase in TST result obtained with the use of the 10 TU dose was large enough to increase the number of positive individuals by 11% (14/128) using a 10 mm cut off. If, however, a 15 mm cut off was used, as is recommended in Australia and the UK, only one extra positive reading was seen with 10 TU compared with the 5 TU dose. Given that most of our health care workers had a past history of BCG vaccination, it would be of interest to assess the differences in a group of non-vaccinated individuals. The lack of a gold standard to determine who is truly infected with tuberculosis when interpreting a TST result remains an issue for the significance of our study, as with other authors on this topic.
These data suggest that, in subjects having a TST, the impact of using 5 or 10 TU to perform the test when comparing studies using one or the other of these doses is likely to be limited. Nevertheless, these differences should be borne in mind and our data suggest that studies using 10 TU should be calibrated back by 1.5 mm to enable comparison with studies employing 5 TU. Whether the previously perceived advantages of using 10 TU in countries such as Australia and the UK really justify the potential for confusion when interpreting the result remains uncertain.