Article Text

Abstract
The case history is presented of a patient with acute respiratory failure complicated by nasal obstruction resulting in intolerance of nasal ventilation. Urgent insertion of nasal stents permitted restoration of ventilation with resolution of breathlessness and stabilisation of arterial blood gases.
- cystic fibrosis
- respiratory failure
- nasal stents
- nasal intermittent positive pressure ventilation
Statistics from Altmetric.com
Type II respiratory failure is common in patients with cystic fibrosis with advanced disease and may respond to long term nasal ventilation. We report a case of acute respiratory failure complicated by nasal obstruction resulting in intolerance of nasal ventilation which required urgent insertion of nasal stents.
Case history
The 28 year old mam with cystic fibrosis had diabetes mellitus, mild liver disease, aminoglycoside induced renal tubulopathy, sputum colonised with Pseudomonas aeruginosa, and type I (hypoxic) respiratory failure requiring long term oxygen therapy. His spirometric test results when well gave forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) of 0.95/2.67 l with stable capillary blood gases as in table 1 (column A).
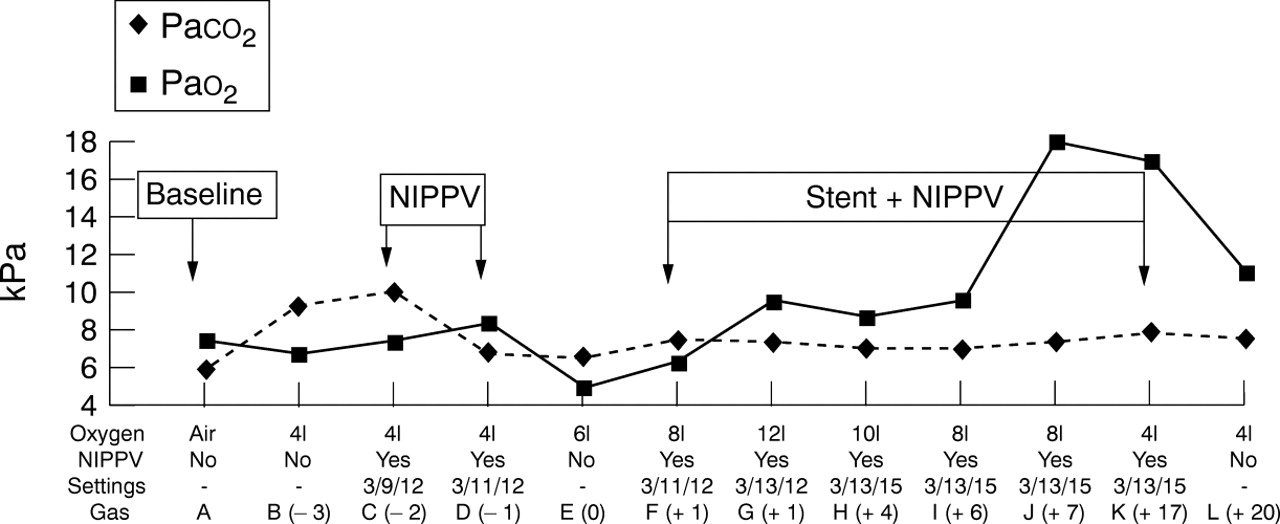
Blood gas tensions during nasal ventilation in relation to placement of stents
He was admitted with an FEV1/FVC of 0.55/1.80 l and an oxygen saturation of 84% breathing room air. His nebulised medication included DNase (Pulmozyme®), β2 agonists, and colistin sulphate with inhaled fluticasone. He received supplemental nasogastric feeding and required Creon 8000, cisapride, ranitidine, metoclopramide, and Humulin insulin.
Investigations revealed hypokalaemia (K+ = 2.7 (normal range 3.5–5.3) mmol/l), hypomagnesaemia (Mg2+ = 0.68 (normal range 0.7–1.0) mmol/l), and neutrophilia of 11 700/ml. A full blood count and renal and liver function were otherwise normal. Treatment with intravenous aztreonam and tobramycin and K+and Mg2+ supplementation was commenced and he initially improved, but after 14 days his antibiotics were changed to Tazocin, colistin sulphate, and ciprofloxacin for extended cover of a resistant Pseudomonas and metronidazole for possible anaerobic infection.
He continued to improve but on the 40th day of admission he again deteriorated with a fever of 39.6°C with arterial blood gas tensions as shown in table 1 (column B). Nasal intermittent positive pressure ventilation (NIPPV) was commenced at settings of 3/12/12 on 4 l oxygen (expiratory positive airway pressure (EPAP) 3 cm H2O/inspiratory positive airway pressure (IPAP) 12 cm H2O/default rate = 12 breaths/min). He deteriorated overnight (table 1 (column C)) and was treated with intravenous hydrocortisone, increased ventilation (3/14/12 on 6 l oxygen), and physiotherapy for presumed sputum retention. The antibiotics were changed to ceftazidime, tobramycin, and Tazocin and by the following morning he had improved (table 1 (column D)). The following night his nose blocked and, despite fluticasone 50 μg nasal spray, ephedrine 0.5% drops, and saline washes, he was unable to tolerate NIPPV either nasally or via a full face mask. Despite maximal medical treatment including intensive physiotherapy and maximal oxygen by mask his gases deteriorated (table 1 (column E)) and he began to tire. The changes in blood gas tensions are shown in fig 1.
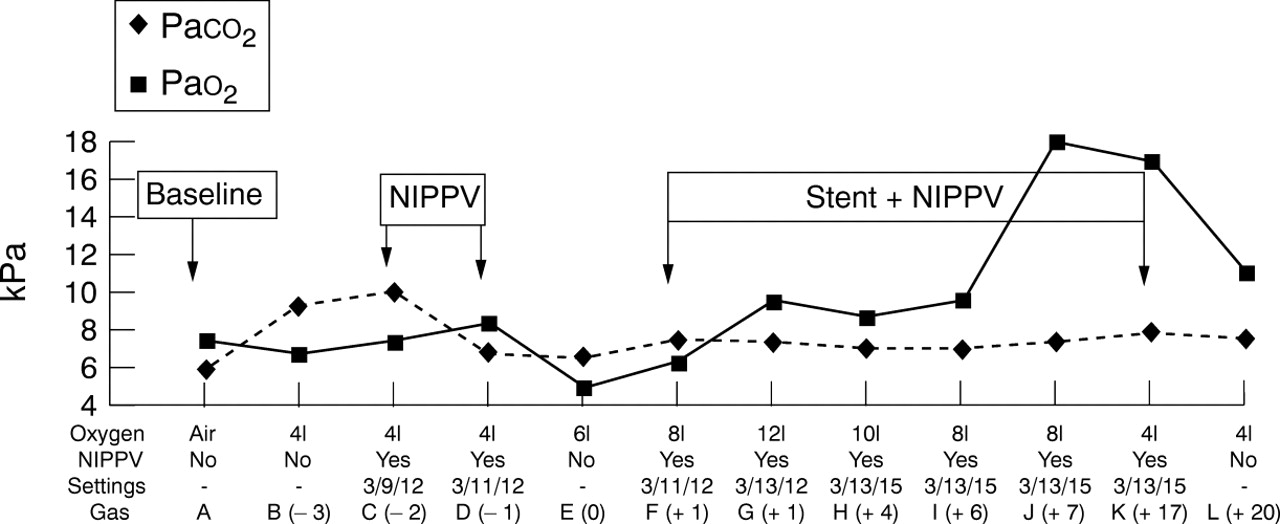
Blood gas tensions during nasal ventilation in relation to placement of stents.
Nasendoscopy performed to determine the cause of the nasal blockage revealed minimal crusting and debris but markedly oedematous nasal mucosa unresponsive to 1:80 000 adrenaline and 5% cocaine spray. An attempt to insert size 6 nasopharyngeal tubes failed due to the extent of the obstruction airway. Portex Blue Line size 4.5 siliconised endotracheal tubes (internal diameter 4.5 mm, external diameter 6.5 mm, Portex Ltd, Hythe, Kent, UK) were therefore placed under direct vision using a nasendoscope to lie in the postnasal space on each side, trimmed at approximately 14 cm with 2 cm projecting externally allowing the tubes to be sutured together anterior to the columella (fig 2A and B). Nasal toilet was then performed with saline douches. Advancing the tubes into the nasopharynx (fig 2C and D) by extending the patient's neck enabled pulmonary toilet via a size 10 suction catheter after which the tubes were withdrawn back into the postnasal space to avoid excessive gagging. After two hours on NIPPV set at 3/11/12 with 8 l oxygen the gases were as shown in table 1(column F) and fig 1, improving overnight (table 1 (column G)) on increased ventilation (3/14/12 and 12 litres oxygen).

{kind=link}
{kind=link}
Nasal stents projecting (A) and (B) 2 cm beyond the nares over which the nasal mask fitted comfortably and (C) and (D) pushed into the nasopharynx to facilitate passage of a suction catheter and nasogastric tube.
Continued maximal medical therapy including physiotherapy five times daily resulted in improved gas tensions despite reducing inspired oxygen. Nasogastric feeding was recommenced via a size 8 Portex infant feeding tube passed through the right sided stent. The left tube was removed on day 18 and by day 20, when no longer reliant on overnight ventilation (table 1 (column L)) the second stent was removed. Fluticasone 50 μg and xylometazolone 0.1% nasal sprays were commenced but the patient reported no nasal stuffiness or blockage and was later able to recommence NIPPV.
No organism was found to account for his pyrexial illness and deterioration. Multiple central and peripheral blood cultures, urine and stool cultures were negative. Tests forLegionella and respiratory viruses including CMV and EBV were also negative. HisPseudomonas remained sensitive to tobramycin and colistin sulphate throughout with intermittent sensitivity to Tazocin. At the time of writing he remains in hospital on intravenous antibiotics and on the active transplant list.
Discussion
Nasal polyposis and chronic rhinosinusitis is not uncommon in cystic fibrosis.1 Nasal ventilation has previously been described in cystic fibrosis2 and, in this centre,3 is used to treat type II respiratory failure in patients awaiting transplantation. Despite routinely prescribed nasal steroids, dryness and crusting is common though recently introduced custom designed warm air humidifiers such as HumidAire (ResMed (UK) Ltd, Abingdon, Oxon, UK) appear to lessen the incidence of nasal problems.
Alternative patient interfaces with NIPPV are available including full face masks, unsuccessful in this case, and mouth only or nose and mouthpieces which have been used extensively elsewhere4but which were not available in this case. Standard nasopharyngeal airways were found to be too soft to bypass the obstruction and hence an alternative was sought. Silicone tubes have been used as stents following surgery for acquired choanal atresia5 in infants and rarely in adults.6 Endotracheal tubes have similarly been used in infants7 but we are unaware of the use of this technique acutely in adults.
In this case, having been unable to oxygenate the patient, urgent insertion of nasal stents permitted restoration of NIPPV which successfully treated the acute hypoxia and improved hypercapnia over time. The procedure was well tolerated; nasal complications such as columellar or septal ulceration, nasal cavity or sinus infection were not seen8 and the nares remained patent after removal of the tubes. We believe the use of urgently inserted nasal stents was life saving in this case.
Acknowledgments
We thank Dr D E Stableforth, consultant physician, for permission to publish on this patient and Dave Thomas, senior ODA, ENT theatres for modelling the nasal stents. Dr Wildman is sponsored by the UK CF Trust.
Footnotes
Funding: none.
Conflicts of interest: none.