Article Text

Statistics from Altmetric.com
In recent years there has been a rapid growth of interest in the use of non-invasive ventilation (NIV) in the management of patients with acute and chronic ventilatory failure. This paper reviews the evidence for the effectiveness of NIV in the management of chronic hypercapnic ventilatory failure and discusses possible mechanisms by which NIV has an effect.
Evidence base for the use of NIV in chronic ventilatory failure
SLOWLY PROGRESSIVE NEUROMUSCULAR DISEASE AND CHEST WALL DISORDERS
Several uncontrolled studies have shown benefit from nocturnal NIV in terms of improvement in daytime arterial blood gas tensions, relief of the symptoms of nocturnal hypoventilation, and improved survival compared with that which would be expected without treatment in patients with neuromuscular and chest wall diseases.1-5In a large case series Leger et al 6 reported on 276 patients with chronic ventilatory failure. In patients with kyphoscoliosis or sequelae of previous tuberculosis (usually thoracoplasty) they found a significant improvement in diurnal arterial oxygen and carbon dioxide tensions (Pao 2 and Paco 2) and a reduction in the need for hospitalisation for respiratory illness following the introduction of NIV; 62% of the patients reported improvement in their quality of sleep and 70% reported improvements in activities of daily living. NIV was continued for two years by 80% of the kyphoscoliosis group, 76% of the patients who had sequelae of previous tuberculosis, and 56% of the patients with Duchenne-type muscular dystrophy (DMD). In a further uncontrolled study Simonds and Elliott7 reported the five year actuarial probability of continuing NIV in patients with scoliosis, previous polio, post tuberculous lung disease, and generalised neuromuscular disorders to be 79%, 100%, 94%, and 81%, respectively. After one year of NIV arterial blood gas tensions recorded during spontaneous breathing by day showed that, compared with the pretreatment value, Pao 2 increased by a mean (SD) of 1.8 (1.9) kPa and Paco 2 decreased by 1.4 (1.3) kPa. Quality of life, assessed on one occasion following the introduction of NIV, showed mental health, energy and vitality scores of the short form 368 similar to the UK population norms; the remaining domains were similar to other patients with chronic disease, except physical functioning scores which were lower. Masaet al,9 in a two week comparison of NIV with overnight supplemental oxygen, showed that, although oxygen therapy resulted in a greater improvement in overnight oxygen saturation, it did not ameliorate symptoms of morning headache, lethargy, or dyspnoea. By contrast, NIV was effective in ameliorating symptoms and improved diurnal arterial blood gas tensions. Of the 21 patients studied, 19 opted to continue with NIV, one with oxygen, and one declined both.
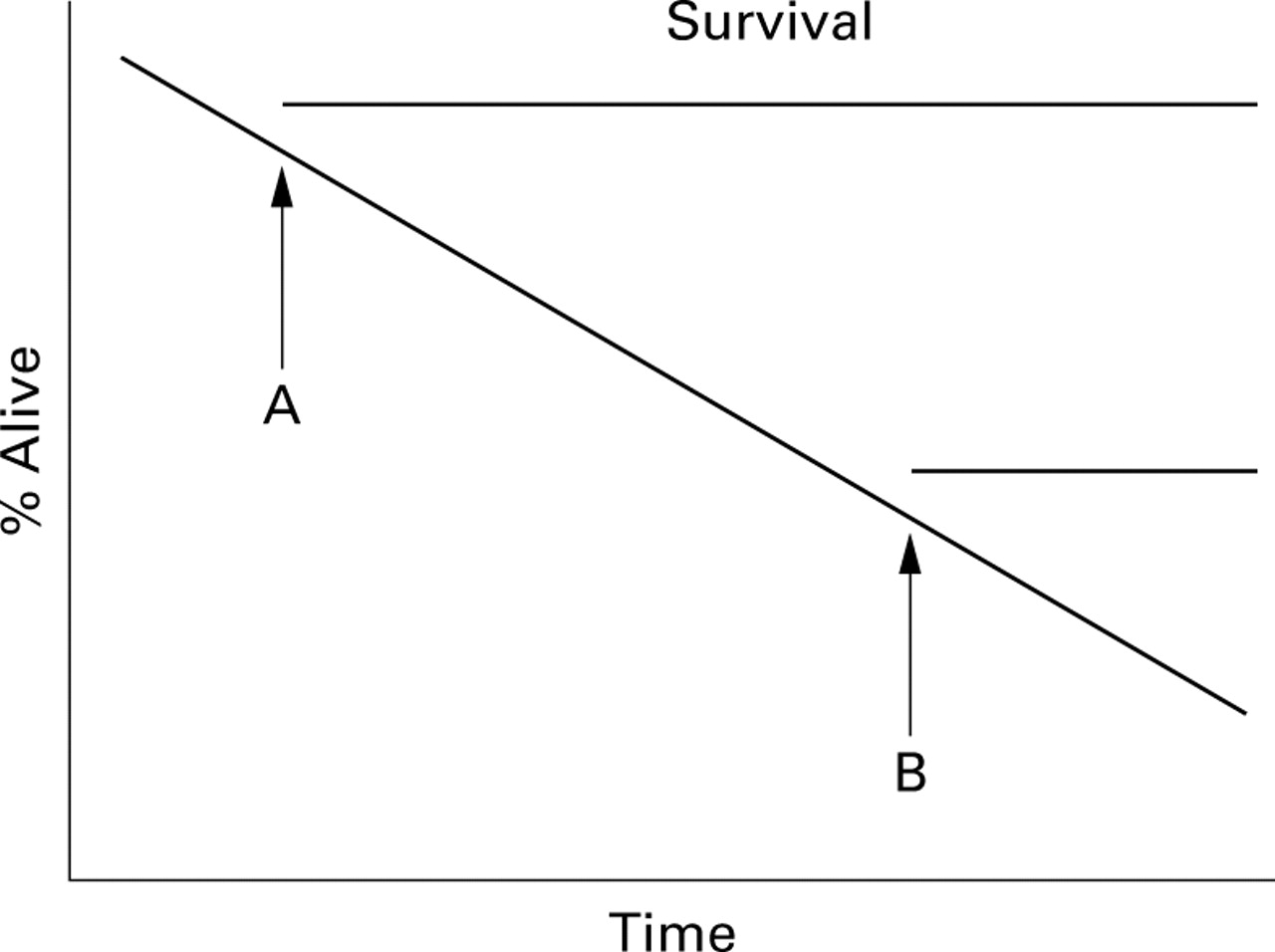
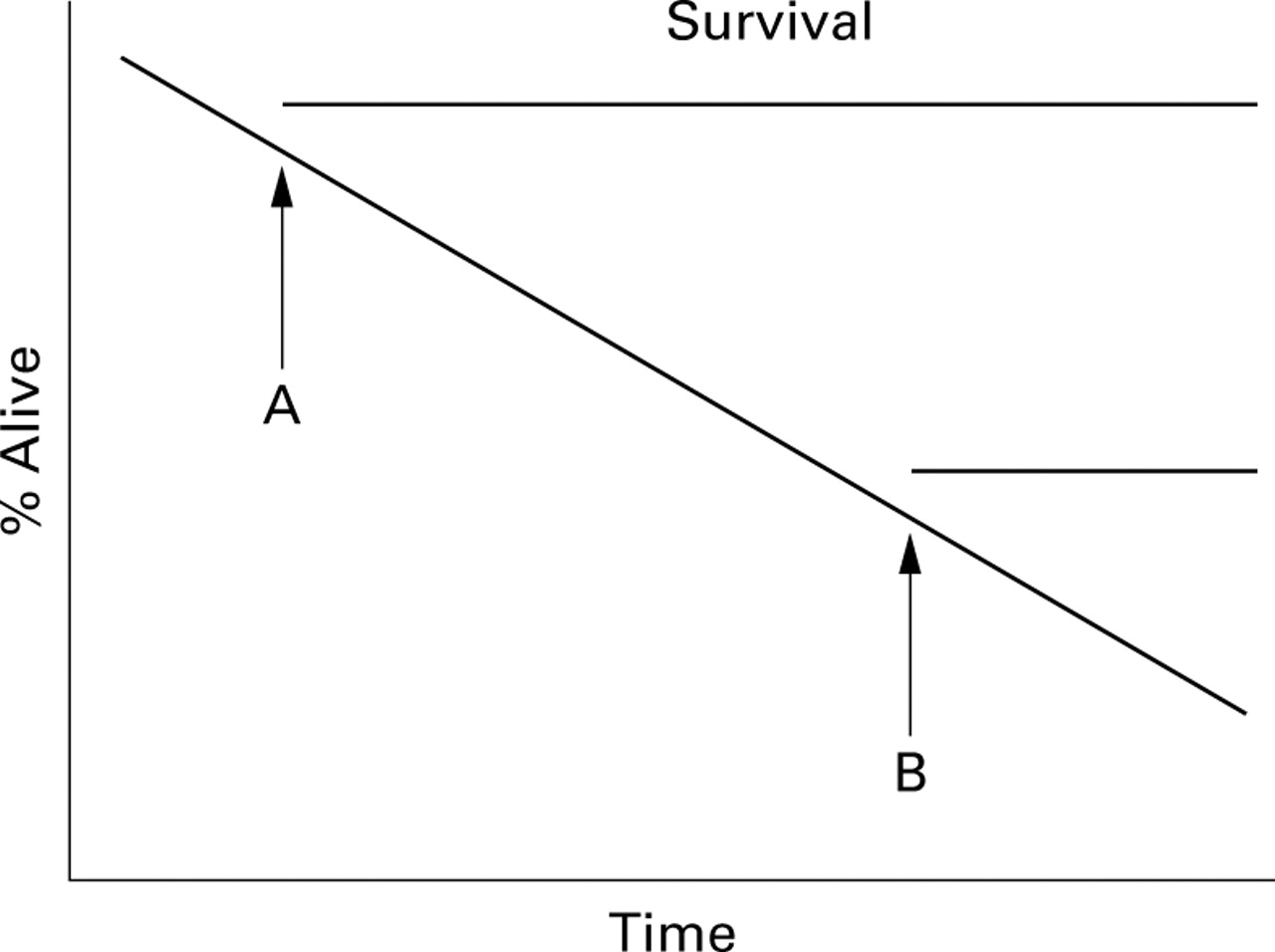
Increasingly, at least one, and preferably more, double blind placebo controlled trials are required as proof of the effectiveness of an intervention and, for obvious reasons, such data are lacking in this area. Retrospective or non-controlled studies potentially bias the literature for a number of reasons. Firstly, negative results are often not published and the literature therefore reflects the experience of a few enthusiastic units, usually tertiary referral centres, which, by their very nature, receive a highly selected group of patients, limiting the generalisability to routine practice. Secondly, the time at which NIV is initiated may affect length of survival—the earlier NIV is started, the longer survival is likely to be. As an example, fig1 shows the theoretical natural history of decline in respiratory function in an individual; if NIV is initiated at point A, a much longer survival will be achieved than if initiated at point B, though the patient still dies at the same point in the natural history of the disease and in time. The improved survival is therefore cosmetic. Thirdly, for ease of analysis and presentation, patients with a variety of different disorders are placed in the same group and good results in one disorder may mask a lack of benefit in another when all are analysed together. Caution should therefore be exercised in the interpretation of survival data in uncontrolled studies.
{kind=link}
Schematic representation of the natural history of a condition showing that, although survival is apparently longer in A than in B, this is cosmetic and the patient dies at the same time, independent of the intervention. Reproduced from Elliott70with permission of the publishers.
NIV is often started to improve symptoms. In some cases the improvement is dramatic and symptoms return consistently when NIV is withdrawn, but often it is non-specific and includes an improved sense of wellbeing and reduced breathlessness. There are few data comparing quality of life objectively using appropriate scales after NIV or objective confirmation of end points which are important to patients such as breathlessness during exercise. NIV during sleep is often considered to be an unpleasant treatment, and the fact that patients use it is considered evidence of benefit since it is assumed that patients would not continue if they did not perceive that the advantages were greater than the disadvantages. The same has been thought to be true for continuous positive airway pressure (CPAP). However, a recent double blind randomised controlled trial comparing active with sham CPAP showed a significant placebo effect upon symptoms, particularly energy and vitality, although the improvements were substantially and significantly less than those seen in the actively treated group.10 The placebo effect of a “breathing machine” on an individual with breathing problems who has been told that he or she has potentially life threatening ventilatory failure should not be underestimated.
Observational studies are valid, however,11 and the place of NIV in these patient groups is now well established and most would consider it unethical to perform a prospective randomised controlled trial with survival, or even quality of life, as end points. However, questions remain regarding the appropriate timing of intervention and further data are needed.
RAPIDLY PROGRESSIVE NEUROMUSCULAR DISEASE (E.G. DUCHENNE MUSCULAR DYSTROPHY, MOTOR NEURONE DISEASE)
Death from ventilatory failure is common in these patients and assisted ventilation may be instituted when the patient is in extremis, sometimes before a firm diagnosis has been made, when there is little doubt from short term trials of spontaneous breathing that the patient cannot sustain sufficient ventilation to support life. A number of studies have shown symptomatic benefit in patients at an earlier stage in the natural history of their disease.12-16 In a non-randomised controlled trial Pinto et al 15 compared the outcome in 10 patients with motor neurone disease (MND) treated with NIV and 10 control patients who had refused NIV. Although the forced vital capacity (FVC) of the NIV treated group was lower, suggesting more severe respiratory muscle weakness, 50% were alive at two years whereas all the control patients had died within eight months. Raphael et al 17 randomised patients with DMD to receive NIV or conventional treatment and found that there was a trend towards an increased mortality with NIV. However, this study should be interpreted with some caution; in the light of current knowledge such patients might not be expected to benefit from NIV because they did not have evidence of hypoventilation either by day (Paco 2 normal) or at night (not measured but unlikely given normal daytime Paco 2). However, uncontrolled studies6 ,18 have shown excellent results in terms of survival in patients with DMD, with one reporting a 73% five year survival in 24 patients with severe hypercapnic ventilatory failure (mean Pao 2 7.6 (2.1) kPa, Paco 2 10.3 (4.5) kPa, VC 306 (146) ml) at presentation.18
In patients with rapidly progressive disease there are a number of possible problems related to extending life by mechanical ventilation. These include life of marginal quality, loss of dignity, inability to communicate, disruption to the lives of other family members, and difficulty in stopping high technology life sustaining care once it has been started.13 For most patients and their carers it is not just a question of longer life, but better quality of life. Few data have been published on the quality of life of patients with MND receiving home mechanical ventilation (HMV). Howardet al reported significant symptomatic improvement without distressing prolongation of life.12Moss et al 19 found that 90% of patients were glad that they had chosen HMV and would do so again. Ninety four percent of carers were glad that the patient had chosen HMV and 83% would encourage the patient to choose it again. However, only 50% said that they would choose HMV for themselves, and the main reason cited was not wanting to be a burden to others. However, this was a highly selected group of subjects; of 355 patients with MND in Northern Illinois (the potential study population) only 15 (4.2%) were on home ventilation. In the study of patients with DMD by Simondset al,18 although the physical function domain of the SF-36 questionnaire was markedly reduced, domains such as mental health, role limitation related to physical and emotional factors, and social function did not differ significantly from age matched male controls.
It is important to realise that healthcare professionals may significantly underestimate their patient's satisfaction with life.13 Physically able healthcare professionals are not the best people to make decisions about what is or is not an acceptable quality of life for patients with severe neuromuscular disease.13 ,20 Bach et al 21 surveyed 82 ventilator assisted individuals with DMD and found that 12% of responding patients expressed dissatisfaction with their lives in general compared with 9% of the surveyed healthcare professionals and 7% of the general population. The healthcare professionals significantly underestimated the patients' scores in the life satisfaction and general affect instruments and significantly overestimated the patients' assessment of the relative hardship associated with ventilator dependence. They concluded that most severely disabled chronic ventilator assisted individuals with DMD had a positive affect and were satisfied with life despite the physical dependence which precluded many of the activities most commonly associated with perceived quality of life for physically intact individuals. They concluded that healthcare professionals should not use their judgement of a patient's quality of life to justify withholding life sustaining therapy.
Thus, there is unlikely ever to be prospective randomised controlled trial data to support the use of NIV in these patient groups since it would be unethical to deny treatment which, certainly in advanced disease, unequivocally prolongs life of acceptable quality. However, further data are needed about the timing of initiation of NIV and the appropriate therapeutic goals (see below). There are no firm guidelines but NIV should be considered when symptoms of hypoventilation develop with an FVC of less than one litre or abnormal overnight oximetry or daytime hypercapnia, with or without hypoxia.22 ,23Abnormal overnight oximetry has been defined as more than five minutes with an oxygen saturation of less than 88%, although this is not based upon any published evidence.23 For patients with rapidly progressive neuromuscular disease it has been suggested that NIV should be considered when the maximal inspiratory mouth pressure falls below –60 cm H2O or the FVC is less than 50% predicted.23 Patients admitted as an emergency with an episode of acute respiratory failure should also be considered for long term domiciliary ventilation.22
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD)
A number of studies in patients with COPD2 ,6 ,7 ,24-29 have shown that NIV is feasible at home during sleep and that it can be used to correct abnormal physiology; gas exchange during sleep can be improved,24excessive respiratory muscle activation reduced,30 ,31 and exercise capacity and diurnal arterial blood gas tensions can be improved.24 ,28 The use of healthcare resources is also reduced.29
However, there have been few controlled trials and most of these had small numbers of patients followed for only a short period of time. Strumpf et al 32 performed a randomised controlled crossover study in 19 patients with COPD and found that seven were unable to tolerate the nasal mask and a further five withdrew because of intercurrent illness. In the seven who did complete the study there were significant differences only in the neuropsychological tests. Acclimatisation was performed as an outpatient, but with regular visits from a respiratory therapist, and ventilation was assessed during wakefulness by measurement of end tidal CO2 tensions, though this measure is unreliable in patients with severe COPD. No measurements were made during sleep and it is therefore difficult to come to any definite conclusions since adequate ventilation was not confirmed. In addition, the patients were not particularly hypercapnic (mean Paco 26.13 kPa). Meecham Jones et al 33 performed a similarly designed crossover study of the use of nasal pressure support ventilation and oxygen with oxygen alone and showed statistically significant improvements in daytime arterial blood gas tensions, sleep quality, and quality of life during the pressure support limb of the study. The improvement in daytime Paco 2 correlated with a reduction in overnight transcutaneous CO2 pressure.
Lin34 studied 12 patients in a prospective randomised crossover study of oxygen alone, NIV alone, and oxygen plus NIV each for two weeks. There were no differences in tidal volume, minute volume, spirometric parameters, diurnal arterial blood gas tensions, mouth pressures, or ventilatory drive. Sleep efficiency was worse during NIV than with oxygen alone. However, the maximum tolerated inspiratory pressure ranged from only 8 cm H2O to a maximum of 15 cm H2O. No data were given about the effect of NIV on blood gas tensions during ventilation and there was no statistically significant improvement in sleep hypoventilation with NIV. Given this, it is perhaps not surprising that no effect on daytime function was seen. Because negative studies are difficult to interpret if no data are given about whether the treatment was applied appropriately, the therapeutic goal of NIV must be defined in future outcome studies and it should be confirmed whether or not it was achieved.
Case series of patients with COPD suggest survival comparable to that seen in the oxygen treated patients in the MRC and NOTT studies.28 ,35 ,36 Although direct comparison cannot be made with historical controls from 20 years ago, it is important to note that the patients with COPD selected for home ventilation were often those who had “failed” (not rigorously defined) on oxygen therapy and were usually hypercapnic. A number of studies suggest that hypercapnia is a poor prognostic sign.35 ,37 ,38 The MRC study suggested that the presence of hypercapnia was a marker for a lack of benefit from oxygen therapy.35 Cooperet al,37 in a long term uncontrolled study, found that 29 of the 57 patients who were hypercapnic at entry died during the course of the study compared with only three of 15 normocapnic patients. Connors et al 38 found that patients with COPD with a Paco 2 of >50 mm Hg (6.6 kPa) at or just before admission to hospital had a 50% mortality at two years. On the other hand, a study from Japan of 4552 patients with obstructive lung disease did not show any difference in outcome between patients with hypercapnia and those who were normocapnic39; indeed, hypercapnic patients who had had a thoracoplasty had a better prognosis than those who were normocapnic. It is therefore possible, though unlikely, that the patients with a better prognosis are being selected out for home NIV. The arguments about uncontrolled trials and survival outlined above are particularly relevant when considering patients with COPD.
The exact place of NIV in chronic ventilatory failure secondary to COPD remains unclear and needs to be evaluated by further large randomised controlled trials with clearly defined end points. Long term oxygen therapy (LTOT) is one of only two interventions that have been shown to prolong life in patients with COPD and remains the gold standard for the treatment of ventilatory failure due to COPD. At present NIV can only be justified in patients who have symptoms of nocturnal hypoventilation (morning headaches, daytime sleepiness, etc) despite maximal bronchodilator therapy or cannot tolerate LTOT, even with careful administration using Venturi masks or a low flow meter. It should also be considered in patients with intractable peripheral oedema because of the possible beneficial effects on renal blood flow of reducing CO2 pressures40 or of repeated admissions to hospital with hypercapnic ventilatory failure. Most studies suggest that it is the patients with more severe hypercapnia who are likely to benefit and there is no place for nocturnal NIV at present in those without sustained daytime hypercapnia. Adequate control of nocturnal hypoventilation should be confirmed since this has been a feature of the studies in which benefit has been seen.24 ,33
Pathophysiology of ventilatory failure
Ventilation requires a balance between the capacity of the respiratory muscle pump and the load placed upon it as well as an adequate central respiratory drive. Any condition that upsets this balance by increasing the load on the respiratory muscles, by reducing their capacity, or by decreasing the central drive to breathe will place an individual at risk of ventilatory failure. This is particularly true during sleep when certain key alterations in respiratory and upper airway function and ventilatory responses lead to a degree of nocturnal hypoventilation even in normal individuals, causing a rise in Paco 2 of up to 3 mm Hg (0.4 kPa).41 Central respiratory drive is decreased due to a reduction in cortical input to the respiratory centres.42 Input to the intercostal and upper airway musculature is also reduced, especially in REM sleep, leading to a reduction in tidal volume and an increase in upper airway resistance.43-45 Ventilatory responses to carbon dioxide are also altered; both the position and slope of the carbon dioxide response curve are modified, resulting in a higher set point for carbon dioxide and a decreased sensitivity to a rising carbon dioxide pressure.46-49 In individuals with neuromuscular disease, chest wall disease, or COPD, abnormalities of load, drive or capacity exacerbate these changes leading to derangement of blood gas tensions firstly in REM sleep, progressing to non-REM sleep and eventually to diurnal ventilatory failure.
Abnormalities of capacity can arise from intrinsic weakness in the respiratory muscles, as in patients with neuromuscular disease, or where the respiratory muscles are forced to work at a mechanical disadvantage due to chest wall deformity or by hyperinflation in patients with COPD.42 ,50 The capacity of the respiratory muscles is further reduced by hypoxia, hypercapnia, and acidosis.51 Increases in load are caused by airway obstruction and reductions in lung compliance due to loss of lung elasticity as a result of chronic underinflation of alveoli and reduced chest wall compliance.42 Airway obstruction may cause the development of intrinsic positive end expiratory pressure (PEEPi) because alveolar emptying is incomplete by the end of expiration. Gas flow into the alveoli occurs only when the pressure within them falls below the pressure at the mouth and nose. In the presence of PEEPi there is an inspiratory threshold load and the first part of each inspiratory effort is wasted because gas decompression occurs without airflow. This increases the work of breathing and decreases ventilatory efficiency. Significant increases in upper airway resistance, which can occur due to bulbar muscle dysfunction in neuromuscular disease or because of coexistent obstructive sleep apnoea, will also increase the load on the respiratory muscles. When excessive rises in Paco 2 occur a transient acidosis will ensue; a compensatory retention of bicarbonate by the kidneys is then established which in turn leads to a secondary reduction in respiratory drive.52
Severe derangements of any one of load, drive, or capacity or small abnormalities of several in combination may lead to the development of ventilatory failure. For instance, it will occur in a normal individual if the respiratory muscle pump is working against an intolerable load, as occurs in acute severe asthma, or if the drive is reduced by large doses of sedative drugs even though the lungs are normal and the respiratory muscles are of normal strength. By contrast, in a patient with severe neuromuscular disease the respiratory muscles may be so weak that they may not be able to sustain ventilation of even normal lungs. Combinations of abnormal load, drive, and capacity may result in severe ventilatory failure even with relatively trivial reductions of each parameter. For example, a patient with severe weakness of the respiratory muscles may be able to maintain effective ventilation and normal arterial blood gas tensions, but a small reduction in lung compliance caused, for example, by a chest infection causes severe decompensation. Similarly, a patient with severe chronic airflow limitation may maintain adequate, though not normal, blood gas tensions until either the load is increased (as in an acute exacerbation) or the drive is reduced (as, for instance, by the injudicious use of sedative drugs). An understanding of the contribution of each of these factors to the development of ventilatory failure (table 1), and the way in which these may change either as part of a normal physiological response or because of disease, will help in formulating a logical treatment strategy of both acute and chronic ventilatory failure.
Load, drive, and capacity in the various conditions treated with non-invasive ventilation (NIV)
Effect of NIV
It has been suggested that NIV “works” by resting chronically fatigued respiratory muscles.53 However, research in this area has been hampered by the absence of good tests of respiratory muscle fatigue and conflicting results have been reported. Small increases in mouth pressure have been cited as evidence of improved capacity though, in the absence of a control group, these may have been due to learning effects and better motivation; other studies54-57 have reported improved daytime arterial blood gas tensions in the absence of changes in the indices of respiratory muscle strength. Shapiro et al 58 studied 184 patients with COPD randomised to receive active or sham negative pressure ventilation at home using a poncho wrap ventilator. They did not show any significant difference between the two groups but compliance with treatment was much less than anticipated. They compared their primary end point, a six minute walking test, with the “dose” of respiratory muscle rest actually delivered and found that there was no relationship. They concluded that respiratory muscle fatigue did not exist and little was to be gained by resting the respiratory muscles. However, six minute walking distance is an unconventional measure of respiratory muscle fatigue and is affected by other factors. Because of the problems with the application of negative pressure ventilation and the use of a crude measure of respiratory muscle fatigue, it is difficult to draw any meaningful conclusions from this study except that the failure of compliance suggests that, if there was any symptomatic benefit, it was outweighed by the disadvantages associated with negative pressure ventilation. Further carefully designed studies in stable patients, controlling for the effects of motivation and learning upon test performance, and newer techniques to assess respiratory muscle function59 ,60 are needed.
There are few data about the effect of NIV upon load. Simondset al 61 did not show any change in accessible lung volume in patients using a device delivering large tidal volumes used for 10–15 minutes per day, which suggests either that atelectasis is not present or is irreversible in these patients. However, there was a sustained improvement in vital capacity and maximum voluntary ventilation and it was suggested that this may have been due to changes in chest wall compliance. In eight patients with COPD Elliott et al 54 showed a small reduction in gas trapping and an increase in dynamic compliance and hypothesised that this was due to a reduction in lung water.
There are some data to support the hypothesis that a restoration in central drive is important. Berthon Jones et al 62 showed a left shift of the ventilatory response curve to progressive hypercapnia in patients with severe obstructive sleep apnoea after 90 days of treatment with continuous positive airway pressure. Annane et al 63 found that the improvement in diurnal Paco 2 correlated with the improvement in the slope of the ventilatory response to carbon dioxide in patients with neuromuscular disease and chest wall deformity. In eight patients with severe COPD ventilated non-invasively during sleep for six months Elliott et al 54 showed a reduction in bicarbonate and base excess and a resetting of the ventilatory response to CO2 at a lower level. However, Appendini et al 64 recorded a high occlusion pressure (P0.1), a measure of central drive, in eight ventilator dependent patients with COPD which suggests that an abnormality of respiratory centre output was unlikely in these patients.
So far the discussion has focused on the effect of NIV on diurnal arterial blood gas tensions and, indeed, an improvement in Pao 2 and Paco 2 is usually taken as a marker of successful ventilation. However, patients receiving domiciliary ventilation often report an improved sense of wellbeing and better quality sleep and this may be accompanied by only small changes in arterial blood gas tensions. Severe sleep disruption occurs in patients with both COPD65 and neuromuscular/chest wall deformity,66 and sleep quality is improved during NIV.24 ,33 ,57 ,63 Evidence that the effects of NIV on sleep quality may be important comes from studies in which it was withdrawn for short periods. Hill et al 67 found a return of symptoms of daytime sleepiness, morning headache, and dyspnoea and worsening nocturnal oxygen saturation, but no change in diurnal arterial blood gas tensions or mouth pressures when NIV was withdrawn for one week in six patients with restrictive chest wall disease. Jiminez et al 68 also showed a deterioration in sleep quality, accompanied by severe derangements in oxygen saturation, when NIV was stopped for 15 days in five patients who had been using NIV for at least two months. It is likely that the rate of deterioration will be determined by the severity of the underlying disease.
However, NIV does not have to be administered during sleep to improve physiological variables and sleep quality. Schonhoferet al 69 allocated patients to receive either NIV during sleep or while awake during the day for a one month period. Improved diurnal blood gas tensions, increased respiratory muscle strength, and a slight reduction in P0.1were seen in both groups with no differences between them. Overnight oxygen saturation, transcutaneous CO2 tensions, and sleep quality also improved in both groups at the end of the study during spontaneous breathing overnight. The reduction in P0.1 and improvement in respiratory muscle strength suggests that an improvement in muscle function rather than a restoration of central drive was the important mechanism. Daytime NIV is an option in patients unable to sleep with a ventilator.
In summary, there are conflicting data about the mechanism of benefit from NIV. Further studies are needed with more sophisticated tests, particularly of respiratory muscle function. On the basis of current knowledge NIV should be targeted to improve arterial blood gas tensions, reduce respiratory muscle activity, and improve sleep quality.
Conclusion
NIV is widely considered to be a very effective treatment in patients with chronic ventilatory failure due to chest wall deformity and neuromuscular disease. It is unlikely that prospective randomised controlled trials with survival as an end point will ever be performed in these patients, but this should not be used as an argument against the use of NIV. However, further data are needed about the optimal timing of its introduction. In patients with more rapidly progressive neuromuscular disease data from controlled trials are available to support the use of NIV. Timing is less of an issue because the interval between when NIV might be introduced and when it has to be is usually relatively short; the major concern relates to the appropriateness of the intervention in an individual patient. In contrast, NIV cannot be recommended for most patients with chronic hypercapnia due to COPD at this time, but there is sufficient evidence to warrant treatment in highly selected patients when all other avenues have been exhausted. The mechanism by which NIV “works” remains poorly defined. As a consequence it is not clear whether the ventilator should be set primarily to improve arterial blood gas tensions, rest the respiratory muscles, or improve sleep quality, but fortunately these goals are not mutually exclusive.