Article Text

Abstract
The case histories are presented of four men with multiple large upper zone lung bullae but otherwise relatively preserved lung parenchyma. Each had a history of significant exposure to marijuana. In three of the four cases the tobacco smoking load had been relatively small, suggesting a possible causal role for marijuana in the pathogenesis of this unusual pattern of bullous emphysema.
- lung bullae
- marijuana
- smoking
- emphysema
Statistics from Altmetric.com
Multiple large lung bullae (variously termed primary bullous disease of the lung or “vanishing lung syndrome”) have been described in young male smokers.1 In this case series the average smoking history was 26 pack years. High resolution computed tomographic (CT) scans showed that these bullae were paraseptal in distribution and hence quite distinct from the more uniformly distributed bullae of centrilobular emphysema which are the typical changes associated with a lifetime of tobacco smoking.2Whilst marijuana smoking has been seen to replicate some of the clinical and pathological consequences of tobacco smoking, an association with bulla formation has not previously been described. We present the cases of four men, smokers of both tobacco and marijuana, who were found to have multiple large peripheral bullae at their lung apices with little parenchymal disease elsewhere in the lung. Our cases are of particular interest, not just because of their young ages, but also because of the unusual pattern of emphysema and the relatively low level of exposure to tobacco smoke compared with that more commonly associated with emphysema.
Case 1
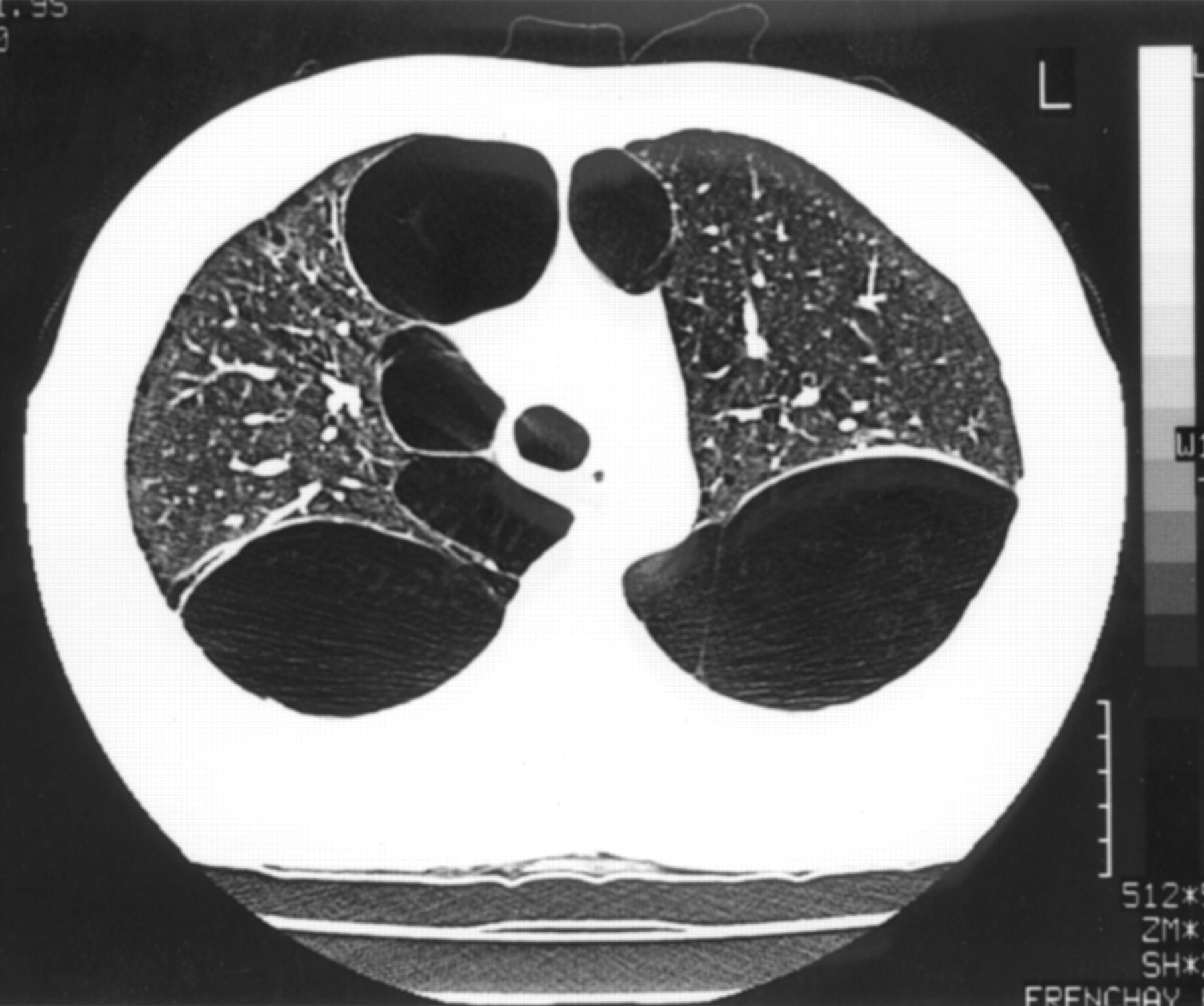
A 27 year old Caucasian man who worked as a diesel engine tester presented initially with a small right sided pneumothorax which was treated by aspiration. At that time a large bulla at the left apex was noticed and two years later he returned with a complete left pneumothorax which required a chest drain. He returned again four years later with pleuritic chest pain but no pneumothorax. He gave a tobacco smoking history of 15 pack years. He had smoked several pipes of marijuana per day for four years but five years previously he had cut down to approximately one per month. Examination was unremarkable except for bilaterally reduced breath sounds at the apices. His α1-antitrypsin level was normal, the chest radiograph showed bilateral upper zone bullae, and a high resolution CT scan of the thorax confirmed extensive peripheral bullae in both upper lobes with some lingular involvement but normal lower lobes (fig 1). Forced expiratory volume in one second (FEV1), forced vital capacity (FVC), carbon monoxide lung transfer factor (Tlco) and diffusion coefficient (Kco) were within normal limits (table 1).

High resolution CT scan of the thorax showing bilateral apical peripheral bullae in a 27 year old man.
Baseline data
Case 2
A 46 year old West Indian video shop owner was referred as a tuberculosis contact. He had no respiratory symptoms but was known to have multiple sclerosis and Peyronie's disease. He smoked half an ounce of tobacco a week (estimated 7 pack years) and two or three joints of marijuana per day. Examination of the respiratory system was unremarkable. Investigation revealed a normal α1-antitrypsin level. Bullae in both lung apices were an incidental finding on chest radiography. A high resolution CT scan of the thorax showed multiple large emphysematous bullae distributed peripherally in both upper lobes with normal residual parenchyma and sparing of the rest of the lung (fig 2). The patient had a normal FVC and FEV1 but low Tlco and Kco(table 1).

High resolution CT scan of the thorax showing multiple large peripheral bullae in the upper lobes of a 46 year old man.
Case 3
A 44 year old West Indian taxi driver was referred with a 12 year history of occasional night sweats. He had been treated empirically for tuberculous pericarditis 12 years earlier. He smoked only two tobacco cigarettes per day but admitted to smoking two to three joints of marijuana daily. Examination and α1-antitrypsin level were normal. His chest radiograph showed bilateral apical bullae, larger on the right, and a CT scan of the thorax verified extensive peripheral apical bullae whilst the middle and lower zones were unremarkable (fig 3). FEV1 and FVC were reduced but gas transfer was preserved (table 1).

CT scan of the thorax showing bilateral apical peripheral bullous emphysema in a 44 year old man.
Case 4
This 35 year old West Indian man was the brother of case 3. He originally presented at the age of 20 with malaise and abdominal distention. On examination he was found to be pyrexial with a right sided pleural effusion, underlying consolidation, and ascites. Despite investigation, no infective cause was found and he was treated empirically with antituberculous treatment. His compliance with medication was poor but nevertheless he made a full recovery and was noted to have a normal chest radiograph at the time of discharge from the chest clinic.
He presented again 13 years later complaining of shortness of breath. In the intervening years he had worked as a welder and he described some exposure to stone dust and asbestos. He kept two cockatiels at home. He was a smoker of cigars and marijuana, admitting to an intake of approximately two joints per week for 20 years, but denied smoking cigarettes. On examination he had some dullness at the right lung base. The α1-antitrypsin level was normal and avian precipitins were negative. The chest radiograph showed extensive bullous changes in both upper zones. A CT scan of the thorax showed gross paraseptal emphysema mainly affecting the upper lobes and the apical segment of the lower lobe (fig 4). There was no fibrosis but there was right sided pleural thickening. Spirometric tests showed reduced FVC and FEV1 with a reduced FEV1/FVC ratio suggesting mild airways obstruction (table 1). Tlco and Kco were 35% and 49% of predicted, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
High resolution CT scan showing gross paraseptal emphysema affecting the upper lobes in a 35 year old man.
Discussion
The harmful effects of tobacco smoking, especially with regard to the aetiology of chronic obstructive pulmonary disease, are well documented.3 Large emphysematous bullae may develop, usually in the context of significant tobacco exposure over many years, and tend to be associated with airway obstruction, reduced gas transfer factor and diffusion coefficient, and evidence of centrilobular emphysema elsewhere in the lungs.2 In young male smokers a more uncommon form of bullous disease has been documented,1 which has a paraseptal distribution and a marked predisposition for the upper lobes. The chronic pulmonary effects of marijuana smoking are less well described and there are as yet no reported associations with large lung bullae. This lack of data may in part be due to difficulties in collecting accurate information from individuals who are likely to be reluctant to give details about smoking a substance which is illegal in most countries.
Other than the psychoactive compound delta-9-tetrahydrocannabinol and other cannabinoid compounds in marijuana, and nicotine in tobacco, smoke from the two substances is virtually identical.4However, there are some fundamental differences when comparing the physical dynamics of smoking marijuana with smoking conventional tobacco. A draw on a marijuana “joint” involves on average a volume two thirds larger, a depth of inspiration a third greater, and a breath holding time four times longer than a draw on a cigarette.5 Indeed, barotrauma in the form of pneumomediastinum has been reported to occur whilst smoking marijuana.6 When this smoking practice is combined with the lack of filter tips on marijuana cigarettes, it leads to a fourfold greater delivery of tar and a five times greater increase in carboxyhaemoglobin per cigarette smoked.5
Regular marijuana smokers experience more cough, sputum, and wheeze than non-smokers and similar levels of symptoms to tobacco smokers. Three to four “joints” of marijuana per day have been reported to give as many symptoms as an average of 22 tobacco cigarettes.7 The physiological effects of marijuana in terms of pulmonary function abnormalities are predominantly in the large airway, producing measurable airways obstruction which returns to normal if the smoking habit is short lived. In a North American longitudinal study8 the effect of marijuana smoking on both FEV1 and Vmax50 was significantly deleterious and at least equivalent to, if not greater than, that of tobacco smoking. There is a less measurable effect than tobacco on the peripheral airways and alveoli but the two substances used concurrently have an additive effect.7 ,9
Smoking three to four marijuana cigarettes per day produces a comparable histological effect on the airways to smoking 20 tobacco cigarettes daily. Changes include basal and goblet cell hypertrophy, cellular disorganisation, and basement membrane thickening.10 All cases of joint marijuana and tobacco smokers showed squamous metaplasia compared with only 50% of cases when either substance was smoked in isolation. There are also differences in alveolar macrophage activity. Whilst both substances increase the numbers of these cells, only tobacco promotes release of superoxide anion, a factor thought to be involved in the pathogenesis of emphysema and of smoking related small airway disease.11
Although tobacco smoking has been implicated in the aetiology of large lung bullae, there are no data to suggest a similar role for marijuana. In three of the four cases described here tobacco consumption was less than that more commonly associated with the development of emphysema. Whereas we are unable to implicate marijuana definitively as an aetiological agent, the relatively young age and the low tobacco exposure in three of the cases does raise the possibility of at least an additive role for this illicit substance in the development of giant upper zone bullae. If this is the case, the pathophysiological mechanism for bulla formation in susceptible individuals is likely to be a combination of direct pulmonary toxicity together with pleural pressure swings and airway barotrauma associated with the high inspiratory pressures deployed in marijuana smoking. There is a public perception that marijuana smoking has little adverse effect on physical health and, given the growing political lobby to legalise marijuana and associated substances in the UK, we hope that our case reports will stimulate further study into their potential lung toxicity.