Article Text

Abstract
The spectrum of nitrofurantoin lung injury continues to widen. The case histories are presented of two patients who developed lung disease associated with the use of nitrofurantoin with histological features of bronchiolitis obliterans organising pneumonia (BOOP), a rare but recognised form of drug induced injury. The two middle aged women presented with respiratory symptoms after prolonged treatment with nitrofurantoin. Both had impaired lung function and abnormal computed tomographic scans, and their condition improved when nitrofurantoin was withdrawn and corticosteroid treatment commenced. The favourable outcome in these two patients contrasts with the fatal outcome of the two other reported cases of nitrofurantoin induced BOOP. We suggest that the previous classification of nitrofurantoin induced lung injury into “acute” and “chronic” injury is an oversimplification in view of the wide variety of pathological entities that have subsequently emerged.
- bronchiolitis obliterans organising pneumonitis
- drug induced pulmonary disease
- nitrofurantoin
Statistics from Altmetric.com
An increasing number of drugs are recognised as causing lung injury and the spectrum of their adverse effects is widening. A recognised but uncommon form of drug induced lung disease is bronchiolitis obliterans organising pneumonia (BOOP).1 We report two cases of nitrofurantoin induced pulmonary disease with histological features of BOOP.
Case 1
A 34 year old female non-smoker with recurrent urinary tract infections presented with increasing dyspnoea and cough over several months. She had been taking nitrofurantoin 50 mg at night for more than two years. She had no other significant exposures and was on no other medications. Examination was normal. The chest radiograph showed diffuse bi-basal reticulonodular shadowing. Baseline blood tests were normal, except for ANA 1:1280, with a diffuse staining pattern. Lung function tests showed forced expiratory volume in one second (FEV1) of 2.09 l with forced vital capacity (FVC) of 2.33 l (predicted 3.18/4.04). Carbon monoxide transfer factor (Tlco) was reduced to 67% predicted. High resolution computed tomographic (HRCT) scans of the thorax showed patchy peribronchial interstitial thickening, especially of the medium and small sized bronchi, with very little fibrosis. Open lung biopsy specimens showed that many respiratory bronchioles were distorted and largely occluded by fibroblastic tissue with associated mucus plugging and outgrowth of respiratory epithelium into surrounding alveolar tissue, consistent with BOOP. In the absence of other factors a diagnosis of nitrofurantoin induced pulmonary disease was made and the drug was discontinued. Prednisone 30 mg per day, gradually reducing over nine months, resulted in significant symptomatic improvement, significant improvement in lung function (FEV1 3.56 l, FVC 4.20 l, Tlco 82% predicted), and considerable but incomplete clearance of interstitial changes on the HRCT scan.
Case 2
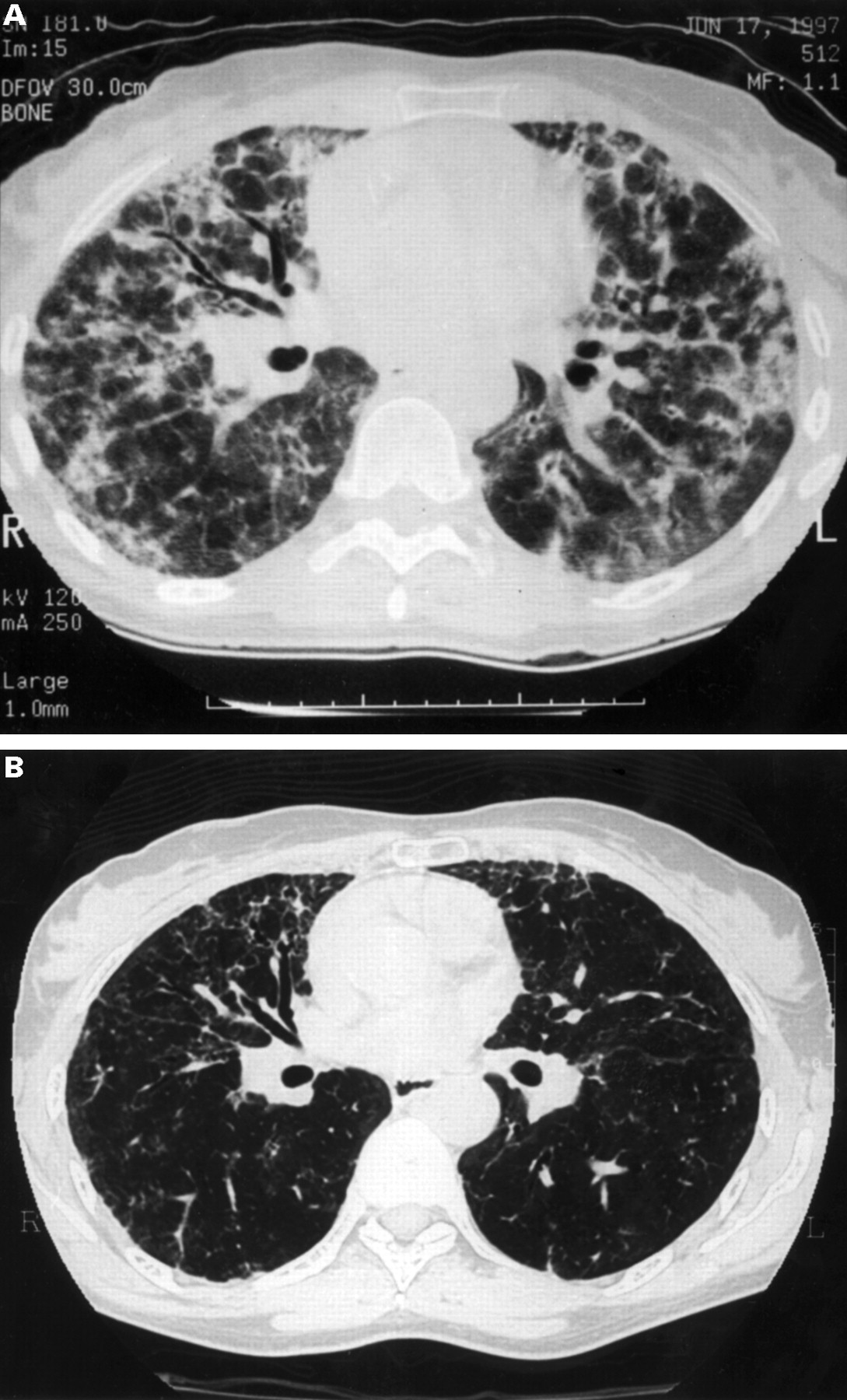
A 50 year old female non-smoker with recurrent urinary tract infections gave a two month history of worsening dyspnoea, fatigue, anorexia, and cough with fevers and night sweats for three weeks. There was no history to suggest an underlying connective tissue disorder. She had been taking nitrofurantoin 50 mg at night regularly for one year. On examination she was tachypnoeic and tachycardic with bi-basal “velcro” crackles. Arterial blood gas measurements showed hypoxia (Pao 2 6.5 kPa) with a wide alveolar-arterial gradient (9.1 kPa). Blood count and renal and liver function were normal, erythrocyte sedimentation rate (ESR) was 81 mm/h, and the ANA was 1:1640 with anti dsDNA negative. Lung function tests showed FEV1 of 0.82 l and FVC of 0.84 l (predicted 2.87 and 3.77 l, respectively). Tlco could not be measured because of breathlessness. An HRCT scan of the thorax showed patches of “ground glass” opacity, interstitial fibrosis with traction bronchiectasis, and scattered areas of dense consolidation (fig 1). Transbronchial biopsy specimens showed loose immature fibrous tissue within air spaces and incorporated into the interstitium, a patchy interstitial infiltrate of mixed inflammatory cells including lymphocytes, plasma cells, and a few eosinophils, and prominent hyperplasia of type II pneumocytes. Pieces of airway wall showed inflammation with peri-airway fibrous and outgrowth of respiratory epithelium into fibrotic lung tissue. The appearance was consistent with BOOP/diffuse alveolar damage. The diagnosis of nitrofurantoin induced pulmonary disease was made; the drug was withdrawn and prednisone 40 mg daily reducing slowly to baseline 10 mg daily was given over three months. At three months a repeat HRCT scan showed marked reduction of the ground glass opacities and areas of consolidation, but with persistent interstitial fibrosis. Repeat lung function tests showed FEV1 had improved to 2.88 l (100% predicted) with FVC 2.89 l (77% predicted) and Tlco 66% predicted. The patient was subsequently weaned off oral steroids with no clinical, radiological, or physiological evidence of relapse.

{kind=link}
(A) Mid thoracic HRCT scan in case 2 showing small residual areas of normal lung, extensive interstitial fibrosis with traction bronchiectasis most marked in the right middle lobe, patchy ground glass opacity, and areas of dense consolidation. (B) Equivalent HRCT scan three months after withdrawal of nitrofurantoin and commencement of treatment with prednisone showing extensive but incomplete clearance of abnormalities.
Discussion
We conclude that both patients had nitrofurantoin induced pulmonary disease on the grounds that there was a lack of an alternative explanation for their lung disease and a good response to drug withdrawal and treatment with an oral corticosteroid. We acknowledge that BOOP of other causes may respond well to corticosteroid treatment, but there was no disease recrudescence on steroid reduction and withdrawal. The establishment of a firm aetiological relationship would require re-challenge with nitrofurantoin. This was considered inappropriate in view of the severity of pulmonary impairment on presentation and the residual and irreversible changes on the HRCT scan.
Relatively few pharmaceutical agents have been associated with BOOP. These include amiodarone, acebutalol, nilutamide, cephalosporins, barbiturates, and cocaine.2 There are only two previously reported cases of BOOP attributable to nitrofurantoin use.3 Both patients were elderly ex-smokers with symptoms of 3–4 weeks duration and both responded well to initial corticosteroid treatment, but rapid tapering led to an irreversible decline and death after failure to respond to increased steroid dosage. Details of drug treatment were not included in the report.
The course of the disease in our patients was rather different. Both were maintained on medium to high dose prednisone initially, gradually reducing over months, and the duration of treatment may have been important in terms of the improved outcome. They were weaned off oral steroids without clinical, radiological, or physiological evidence of relapse.
Nitrofurantoin induced pulmonary disease may present in many forms including BOOP, diffuse alveolar damage, vasculitis, interstitial fibrosis, pleural and airways disease, and pulmonary haemorrhage.1 A final common toxic pathway has not been postulated. Nitrofurantoin induced pulmonary disease may result from immune mediated injury3 ,4 or via hydroxyl radical generation with subsequent free oxidant damage.5 The reduced incidence with the addition of the antioxidant ascorbic acid to nitrofurantoin preparations5 and results of in vitro studies6 suggest that this and other antioxidants may significantly reduce toxicity.
Initial reports suggested that the duration of nitrofurantoin treatment dictated the disease pattern. The “acute” reaction was characterised by marked constitutional symptoms including rash, fever, arthralgia, fatigue, together with pulmonary symptoms of dry cough and dyspnoea.3-5 The “subacute” and “chronic” forms were more insidious, with increased eosinophil count, raised ESR, and vasculitis and interstitial inflammation on histological examination, consistent with a type III immune response.3 ,4 Increased immunoglobulin levels, hepatic transaminases and ANA titres (the so called “drug induced lupus syndrome”7 ,8) was associated with a degree of irreversible fibrosis. Some early reports of biopsy specimens from a patient with nitrofurantoin induced lung disease5 which predate the recognition of idiopathic BOOP as an independent entity are suggestive of a BOOP-like pattern. Cohen3 suggested that BOOP may be a precursor to chronic lung fibrosis, an early and potentially reversible phase in the spectrum of fibrosing lung disease. However, both patients in this report had residual radiological abnormalities although the remaining functional abnormalities were minor. The subsequent variety of pathological entities now shown to be caused by nitrofurantoin suggests that these early categorisations are an oversimplification.
The initial interest in nitrofurantoin induced lung disease has waned as more suitable less toxic agents have been found for chronic urinary infections. However, the drug remains generally available in spite of its high toxic profile and clinicians need to be aware of the spectrum of associated lung disease.