Article Text

Statistics from Altmetric.com
Primary pulmonary hypertension is characterised by a progressive increase in pulmonary artery pressure which eventually leads to right ventricular failure and death. Patients with severe right heart failure—for example, New York Heart Association functional class IV—have the worst prognosis.1 Although several haemodynamic parameters such as pulmonary artery pressure, right atrial pressure, and cardiac index have been shown to correlate with mortality, right atrial pressure reflecting right heart function correlates best with survival. Furthermore, patients with primary pulmonary hypertension in whom the foramen ovale is patent have been reported to live longer than those without a patent foramen ovale.2 These observations led several groups of investigators3-7 (following early animal studies by Austen et al 8 which showed that an interatrial communication allowed decompression of a hypertensive right ventricle and augmentation of systemic blood flow, particularly during exercise) to evaluate the effects of atrial septostomy on clinical signs and symptoms, haemodynamics, and survival in patients with severe primary pulmonary hypertension as well as pulmonary vascular obstructive disease associated with other conditions.
Blade balloon atrial septostomy was first reported by Rich and Lam in 1983 as palliative treatment for refractory primary pulmonary hypertension.9 Several uncontrolled studies subsequently demonstrated clinical and haemodynamic improvement and suggested increased survival in selected patients with severe pulmonary vascular disease.3-6 The limitations of these studies were: (1) the series were all uncontrolled, (2) the indications for performing the procedures varied between the studies, (3) the aetiology of the pulmonary vascular disease was not the same in all patients, and (4) the medical treatment for pulmonary vascular disease has changed over the past 15 years. Despite the significant limitations in these published series, atrial septostomy appears to be a therapeutic modality for advanced pulmonary vascular disease when no other therapeutic options exist and a patient has persistent indications for performing an atrial septostomy.
The acute haemodynamic effect of creating an atrial septostomy is to increase systemic oxygen transport by increasing cardiac output. In addition, the decrease in right atrial pressure reduces systemic venous congestion thereby improving right heart failure. With exercise, right to left shunting will increase further with increased oxygen transport although at the expense of the systemic arterial oxygen saturation. Because the pulmonary vascular bed is unaffected by the procedure, the long term effects of an atrial septostomy must be considered palliative. The reasons why patients improve clinically and haemodynamically following atrial septostomy remain incompletely understood. In addition to resolution of syncopal episodes and a decrease in right heart failure, patients report resolution of ischaemic chest pain following atrial septostomy, suggesting improved right ventricular coronary perfusion due to a decrease in right heart filling pressures.
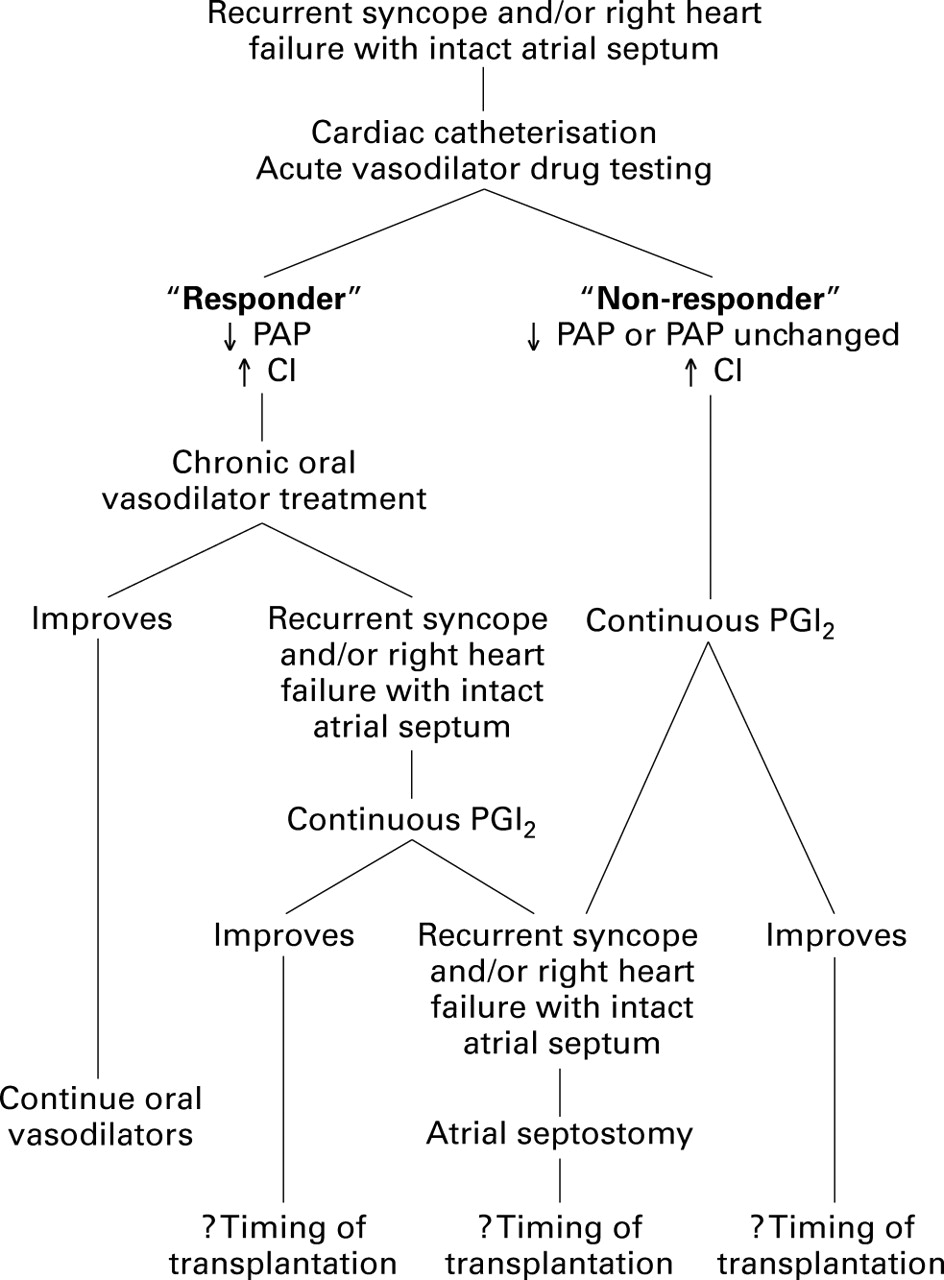
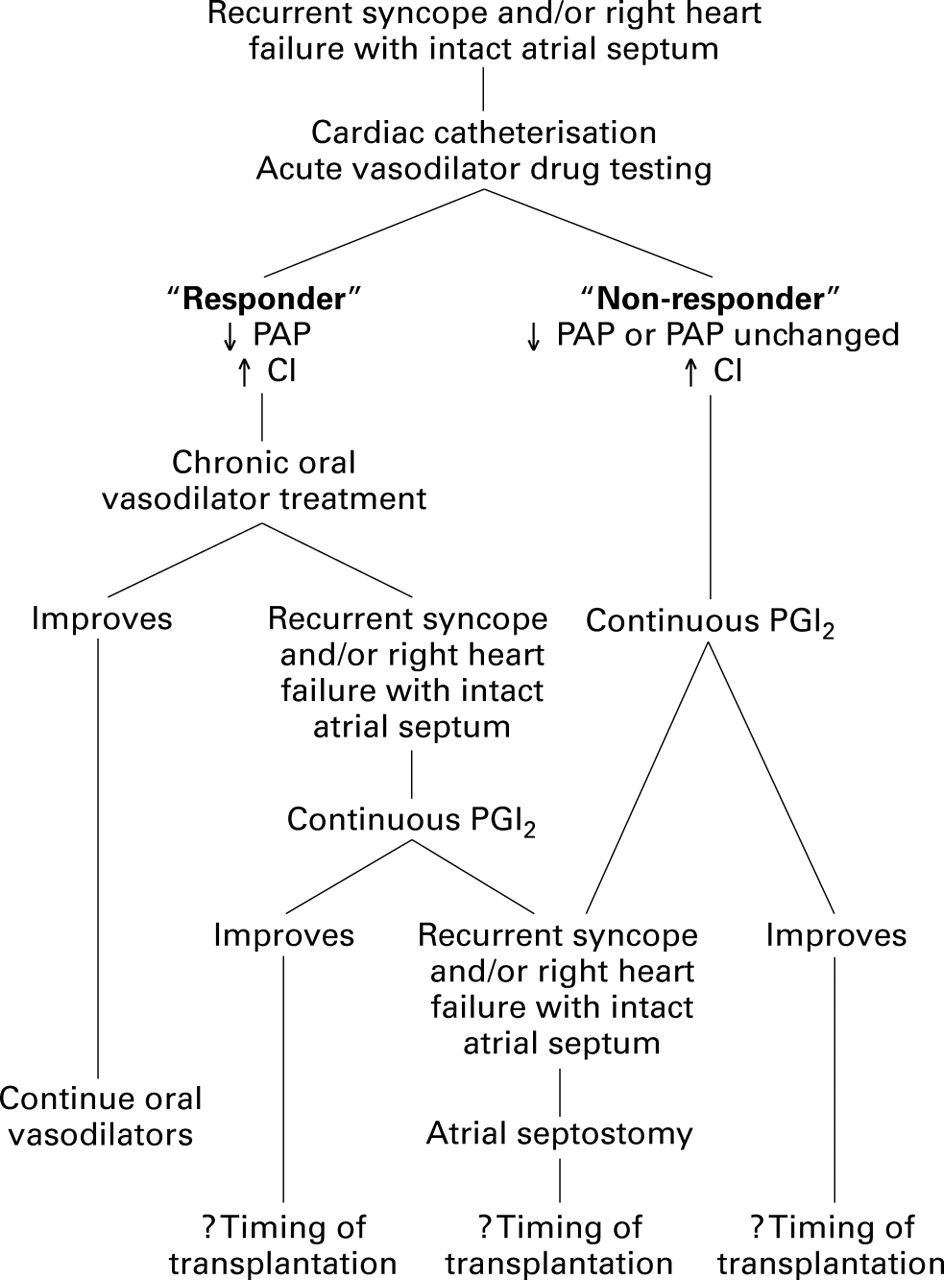
A therapeutic algorithm with suggested indications for performing an atrial septostomy is shown in fig 1. Whether or not a patient has recurrent syncope and/or right heart failure with an intact atrial septum or a restrictive patent foramen ovale, initial evaluation with acute vasodilator drug testing in order to initiate medical therapy with a chronic vasodilator agent is recommended rather than performing an atrial septostomy. If a patient is an acute “responder”, defined by a significant decrease in pulmonary artery pressure with no change or an increase in cardiac index,10 ,11 chronic oral vasodilator therapy with, for example, calcium channel blockade usually results in clinical and haemodynamic improvement as well as resolution of recurrent syncope and/or right heart failure. For patients who are acute “non-responders” with acute vasodilator drug testing—for example, an increase in pulmonary artery pressure or no change in pulmonary artery pressure—several studies have reported clinical and haemodynamic improvement as well as increased survival with continuous intravenous prostacyclin therapy.12-17 Similar to the experience with acute “responders” treated with oral calcium channel blockers, most patients with recurrent syncope and/or significant right heart failure treated with chronic intravenous prostacyclin because they are acute “non-responders” with vasodilator testing no longer have syncope on chronic prostacyclin. In addition, their right heart failure often improves. Based on these studies it is recommended that a palliative atrial septostomy should only be performed in patients who have recurrent syncope and/or significant right heart failure despite optimal chronic vasodilator therapy. The indications for atrial septostomy will vary throughout the world based on the availability of chronic vasodilator treatments such as continuous intravenous prostacyclin or other prostacyclin analogues.
{kind=link}
Indications for performing a palliative atrial septostomy in selected patients with advanced pulmonary vascular disease. PAP = pulmonary artery pressure; CI = cardiac index; PGI2 = prostacyclin I2.
Although many patients with pulmonary vascular disease have shown clinical improvement following atrial septostomy, the procedure is not without risk. Based on the collective experience in the literature,3-7 the 1998 World Symposium on Primary Pulmonary Hypertension published guidelines for performing an atrial septostomy in patients with pulmonary vascular diseases.18Because the procedure related mortality with atrial septostomy in patients with pulmonary hypertension is high, the following recommendations were made to minimise the risk: (1) atrial septostomy should only be attempted in institutions with an established track record in the treatment of advanced pulmonary hypertension and an experience in performing atrial septostomy with low morbidity; and (2) atrial septostomy should not be performed in a patient with impending death and severe right ventricular failure on maximal cardiorespiratory support.
Predictors of procedure related failure or death include a mean right atrial pressure of more than 20 mm Hg, a pulmonary vascular resistance index of more than 55 units/m2, and a predicted one year survival of less than 40%. Candidates for atrial septostomy should have a systemic arterial oxygen saturation on room air of more than 90%. During the atrial septostomy procedure it is recommended that a patient should receive mild and appropriate sedation to prevent anxiety, supplemental oxygen, and careful monitoring of haemodynamics with especially close monitoring of the systemic arterial oxygen saturation. The end point for the procedure should be considered a reduction in systemic arterial oxygen saturation of 5–10%. It is also recommended that the procedure be performed in a stepwise manner to create the smallest possible defect that will produce haemodynamic changes. Before and after septostomy transfusion of packed red blood cells or the use of erythopoietin may be necessary to increase oxygen delivery. Chronic anticoagulation is also recommended.
Although there exists a worldwide experience in over 60 patients, many questions remain unanswered including the optimal timing for the intervention, the mechanisms responsible for the observed beneficial effects, and the long term effectiveness and possible adverse effects. Future investigations evaluating the role of atrial septostomy for pulmonary vascular disease should address whether or not the intervention be performed earlier in the course of the disease. In addition, attempts at elucidating the mechanisms responsible for the beneficial effects may also help to determine if and when an atrial septostomy should be considered. Possible mechanisms proposed for the beneficial effects of atrial septostomy include increased oxygen delivery at rest and/or during exercise, reduced right ventricular end diastolic pressure or wall stress, and improvement in right ventricular dysfunction by the Frank Starling mechanism, as well as relief of ischaemia. Hopefully, as more experience is gained with this procedure, our understanding of why an atrial septostomy is efficacious in selected patients will be increased and, in addition, we will be able to assess overall risk-benefit considerations for individual patients.
In summary, despite the limitations of these published series and the morbidity and mortality associated with the procedure, an atrial septostomy should be considered in selected patients in addition to other treatment modalities available allowing deferral of transplantation because of prolonged survival and an improved quality of life, as well as sustaining seriously ill patients awaiting transplantation. Although the early studies were performed using a blade balloon atrial septostomy, several institutions have recently reported their experience with graded balloon dilation atrial septostomy.6 ,7 These investigators suggest that balloon dilation atrial septostomy decreases the risk of procedure related mortality, although it is associated with an increased rate of spontaneous closure resulting in the need for repeat balloon dilation atrial septostomy.