Article Text

Abstract
BACKGROUND Although it is presumed that exacerbations of chronic obstructive pulmonary disease (COPD) are associated with increased airway inflammation, there is little information available on inflammatory markers during an exacerbation and the relationship with severity or time course of recovery. A study was undertaken to investigate the sputum cell and cytokine characteristics of COPD when stable and during an exacerbation.
METHODS Induced sputum samples from 57 patients with moderate to severe COPD were analysed (44 samples were taken during a stable period and 37 during an exacerbation). The patients recorded daily symptoms on diary cards. Cell counts and sputum levels of interleukin (IL)-6 and IL-8 were measured.
RESULTS Patients with ⩾3 exacerbations/year had higher median stable sputum levels of IL-6 (110 (95% CI 11 to 215) pg/ml) and IL-8 (6694 (95% CI 3120 to 11995) pg/ml) than those with ⩽2 exacerbations/year (22 (95% CI 12 to 93) and 1628 (95% CI 607 to 4812) pg/ml, respectively). Median IL-6 levels were increased during exacerbations compared with stable conditions. The levels of IL-6 during exacerbations were related to the presence of a cold and to the total cell count and eosinophil and lymphocyte numbers, while IL-8 was positively correlated with all sputum cell counts. Sputum cell counts and cytokine levels during an exacerbation did not predict the size and duration of lung function changes in the exacerbation.
CONCLUSIONS Patients with more frequent exacerbations have higher baseline sputum cytokine levels, which may predict the frequency of future exacerbations.
- chronic obstructive pulmonary disease
- cytokines
- induced sputum
Statistics from Altmetric.com
Patients with chronic obstructive pulmonary disease (COPD) are prone to exacerbations that cause a decline in health status.1 Exacerbations are diagnosed usually on clinical grounds when there is a deterioration in specific symptoms or a reduction in lung function.1 ,2 However, in patients with COPD, spirometric changes associated with exacerbations may be small.1 Although it is presumed that exacerbations are associated with increased airway inflammation, as in patients with asthma,3 there is little information available on the nature of inflammatory markers at exacerbation, especially when studied close to onset of symptoms. The relation of these airway changes to symptoms and changes in lung function is unknown. It is also not known whether the degree of the inflammatory response affects the severity or the recovery from exacerbation.
In one study in which bronchial biopsy specimens were taken at exacerbation in patients with chronic bronchitis, airway eosinophilia was found although the patients studied had a mean baseline forced expiratory volume in one second (FEV1) of 76% predicted.4 There is no information available on inflammatory markers at exacerbation in patients with moderate to severe COPD, as biopsy specimens are difficult to take in these patients during an exacerbation. The technique of sputum induction allows study of these patients at exacerbation and we have shown that this is a safe and well tolerated technique in patients with COPD.5 Concentrations of inflammatory cytokines in induced sputum have been shown to be increased in patients with COPD when stable,6 but changes in induced sputum at exacerbation have not been studied.
In order to assess the significance of airway inflammatory markers in patients with COPD we prospectively followed a cohort of patients and examined induced sputum when stable and close to onset of an exacerbation. We related inflammatory markers to symptoms and physiological parameters, both at baseline and during an exacerbation. Patients in this study were all followed with daily diary cards and thus we could also relate the degree of airway inflammatory changes produced by the exacerbation to recovery of symptoms and lung function after the exacerbation.
Methods
STUDY SUBJECTS
Fifty seven patients with a diagnosis of moderate to severe COPD, recruited from the outpatient department of the London Chest Hospital, volunteered to participate in the study. These patients are part of a cohort of patients with COPD followed long term since October 1995 in the East London COPD study. COPD was defined as an FEV1 of <70% predicted for age and height, salbutamol reversibility of <15% or 200 ml with airflow obstruction evidenced by an FEV1/forced vital capacity (FVC) ratio of <70%.7 Patients with a history of asthma, bronchiectasis, carcinoma of the bronchus, or other significant respiratory disease were excluded. All patients had received influenza immunisation as recommended for this patient group. Smoking and treatment history was taken. Patients were recruited when stable—that is, when they had not had any evidence of an exacerbation for at least three weeks. Baseline measurements were made of FEV1, FVC, and peak expiratory flow (PEF) by rolling seal spirometer (SensorMedics Ltd, Yorba Linda, California, USA), reversibility to salbutamol, and ear lobe capillary blood gas tensions (Model 278 Blood Gas Analyser, Ciba-Corning, Medfield, Maine, USA).1 ,8 The study was approved by the City and East London Health Authority research ethics committee and written informed consent was obtained from each patient. The treatment received by the patients was not changed during stable periods.
EXACERBATIONS
The patients maintained daily diary cards after completing their morning medication on which they noted their daily PEF using a mini-Wright peak flow meter (Clement Clarke International Ltd, Harlow, UK) and any changes in symptoms from their baseline conditions. Exacerbations were diagnosed according to criteria modified from Anthonisen and colleagues and used in our previous studies.1 ,2 The following symptom patterns had to be experienced for at least two consecutive days for the diagnosis to be made: any two of three major symptoms—increase in dyspnoea, sputum purulence, and increased sputum volume; or at least one major symptom together with at least one of the following minor symptoms—a cold (increase in nasal discharge or congestion), wheeze, sore throat, cough, or fever. When patients noticed deterioration in symptoms they telephoned a member of the clinical team and were seen by a doctor within 48 hours. The diagnosis of the exacerbation was confirmed in each case by a doctor in the study team. Spirometric parameters were measured and induced sputum samples were taken. No treatment was started for the exacerbation, either antibiotics and/or oral corticosteroids and/or increased inhaled steroids, prior to sampling. After sampling such treatment as would normally have been prescribed was started on an outpatient basis.
The exacerbation frequency was defined as the number of exacerbations suffered by each patient during the previous year. Patients had been under follow up by our team for one year prior to sampling and this information was obtained from the diary cards. The number of symptoms which appeared or showed an increase in intensity on any day, out of those major and minor symptoms listed above, was the symptom count for that day. Changes in PEF, FEV1, FVC and increase in daily symptom count were calculated as the difference between the day of onset and the baseline value. The baseline PEF was calculated as the mean PEF from 14 days to seven days prior to the onset of symptoms. The time course for recovery of symptoms and lung function was studied in these patients. Recovery times were calculated for these parameters to ascertain whether there was any relationship between recovery time and the levels of various sputum markers.
SPUTUM INDUCTION
Stable induced sputum samples were collected from the patients at least two months away from an exacerbation where possible. In one patient it was impossible to obtain a stable sample because of the frequency of the exacerbations. Ten patients dropped out of the study or withdrew consent for sputum induction before a stable sample could be obtained; 20 patients did not have any exacerbations during the study period. In cases where stable samples could not be obtained prior to exacerbation, samples were taken at least three weeks following the exacerbation. Samples were also obtained at exacerbations before treatment was prescribed.
Sputum induction was performed according to the protocol described previously.5 Patients arrived at the clinic in the morning. Measurement of oxygen saturation (Minolta Pulsox 7, DeVilbiss Healthcare, Heston, Middlesex, UK) and spirometric tests were performed on arrival and repeated 10 minutes after premedication with 200 μg inhaled salbutamol via a multidose inhaler. Nebulisation with 3% saline was commenced using a procedure modified from that of Pinet al,3 using the DeVilbiss UltraNeb 2000 ultrasonic nebuliser (DeVilbiss Healthcare). This nebuliser produced an aerosol output of approximately 2 ml per minute with a mean particle size of 0.5–5 μg in diameter. After seven minutes of nebulisation, measurement of oxygen saturation and spirometric tests were performed and nebulisation continued if the FEV1 had not fallen by more than 20%. After a further seven minutes measurements were repeated and the procedure stopped. Patients were instructed to blow their noses and rinse their mouths out with water before expectorating sputum into a sterile pot.
SPUTUM EXAMINATION
Sputum samples were examined as soon as possible, within two hours, adapting methods previously evaluated.5 ,9 ,10 The weight of the total sample was recorded. The sputum was then separated from contaminating saliva by macroscopic examination using a pair of disposable plastic forceps. The selected portion of the sputum was placed in a preweighed tube and the weight of the selected portion of the sputum recorded. The sputum was then mixed with four times its weight of freshly prepared 0.1% dithiothreitol solution made by mixing the dithiothreitol powder with Hank's balanced salt solution (HBSS). This was vortexed for 15 seconds and then rocked for 15 minutes. A weight of HBSS equal to that of the sputum plus dithiothreitol was then added and the whole mixture was rocked for another five minutes. The suspension was filtered through 50 μm nylon gauze to remove mucus and debris without removing any of the cells and then centrifuged at 790g (2000 rpm) for 10 minutes. This resulted in the formation of a cell pellet and a supernatant solution. The supernatant was decanted off and stored at –70°C for future analysis and the cell pellet was resuspended in 400–3200 μl (depending on macroscopic estimation of the size of the cell pellet) of HBSS. The total cell count was determined with a Neubauer haemocytometer using the trypan blue exclusion method to determine cell viability, blue cells being counted as non-viable.10 The absolute number of non-squamous cells per gram of the original sputum sample was determined and the percentage of viable and non-viable cells obtained. The cell suspension was then mixed with HBSS to obtain a count of 0.6–1.0 × 106 cells/ml of the suspension and cytospins were made using a Cytotek cytocentrifuge. The cytospin slides were stained with Diff-Quik to obtain differential cell counts made by counting 400 cells per slide. Interleukin (IL)-6 and IL-8 were measured in the supernatant samples using a quantitative sandwich immunoassay (R&D Systems Europe, Abingdon, Oxon, UK) and expressed as pg/ml of the supernatant. The supernatant itself is a tenfold dilution by weight of the original sputum sample minus cells.
STATISTICAL ANALYSIS
Spirometric data and blood gas tensions followed a normal distribution and were expressed as means and standard deviations while interrelationships were examined using Pearson's correlation andt test. Data for non-normally distributed variables were expressed as medians and interquartile ranges and interrelationships examined using Spearman's correlation, Mann-Whitney U test, and Wilcoxon signed ranks test as appropriate. The median exacerbation frequency was three per patient per year, in agreement with previously published results.1 This was taken as a cut off point to divide the patients into two groups: those who had 0–2 exacerbations during the year (infrequent exacerbators) and those who had ⩾3 exacerbations during the year (frequent exacerbators). Differences in IL-6 and IL-8 concentrations between these two groups were examined using the Mann-Whitney U test. Spearman's correlation test was used to determine the relationships between the various physiological and symptomatic parameters and the cell and cytokine levels. Exacerbation values were compared with stable values using the Mann-Whitney U test and differences in cytokine levels in the presence or absence of various symptoms were assessed using the same method.
Recovery times for PEF were calculated as the time by which a three day moving average reached or exceeded the baseline. A moving average was used to avoid false early recoveries when lung function improved for just a single day, but then remained below baseline for a few more days. Daily symptoms were binary coded and summed to give a daily symptom count. The change in the daily symptom count at exacerbation was measured as the difference between the counts on and before the date of onset. Spearman's correlation test was used to assess the relationship between the recovery times for PEF and symptoms and the IL-6 and IL-8 levels observed at exacerbation. Sputum samples taken three weeks or more following an exacerbation were grouped separately and correlations between cytokine levels in these samples and the fall in PEF and change in symptoms were also examined. The statistical package SPSS was used for all data analysis.
Results
SAMPLES OBTAINED AT STABLE CONDITIONS
The baseline characteristics of the 57 patients (43 men) are shown in table 1. Forty four samples were obtained from stable patients and 37 were obtained during exacerbations. When stable, 33 (58%) of the patients complained of daily cough, 32 (56%) had daily sputum, 22 (39%) had daily wheeze, and 24 (42%) had daily dyspnoea. Twenty one of the patients were current smokers and, as a group, there was a mean (SD) history of 40.4 (12.4) years of smoking. Fifty one of the patients were on inhaled steroids; only five patients were on daily oral prednisolone. Correlations examined in stable sputum samples suggest that those patients with a longer history of smoking had higher IL-6 levels (Spearman's rho = 0.45, p<0.05) and that those with higher IL-8 levels also had higher IL-6 levels at baseline (0.435, p<0.01). Higher levels of IL-8 were also associated with a higher total cell count (0.403, p<0.01) and with higher neutrophil (0.372, p<0.05) and macrophage (0.416, p<0.01) counts. There was no relationship between cytokine levels and the current smoking status. Sets of standard samples of IL-8 and IL-6 were assayed after adding 0.04% dithiothreitol to the samples to ascertain whether this interfered with the assay (this being the amount of dithiothreitol found in the sputum supernatant samples). However, at this concentration there was no significant difference between the standard samples assayed with and without dithiothreitol.
Baseline characteristics of study patients
EXACERBATION FREQUENCY AND SPUTUM CYTOKINE LEVELS
Exacerbation frequency was found to be correlated with stable IL-6 levels (rho = 0.383, p = 0.01) and IL-8 levels (0.311, p<0.05), indicating that patients with higher levels of baseline cytokines in the sputum have more frequent exacerbations. Infrequent exacerbators had a median (95% CI) IL-6 level of 22 (12 to 93) while frequent exacerbators had a median IL-6 level of 110 (11 to 215) pg/ml; this difference was statistically significant (p<0.05; fig 1A). Infrequent exacerbators had a median IL-8 level of 1628 (95% CI 607 to 4812) pg/ml while frequent exacerbators had a significantly higher level at 6694 (95% CI 3120 to 11995) pg/ml (p<0.05; fig 1B). Nine of the 44 stable samples were taken at least three weeks after an exacerbation. The cell and cytokine levels in this group did not differ from the remainder.

Induced sputum levels of (A) IL-6 and (B) IL-8 in patients categorised as frequent exacerbators (⩾3 exacerbations in the previous year) and infrequent exacerbators (⩽2 exacerbations in previous year). Data expressed as medians (IQR).
EXACERBATION SPUTUM DATA
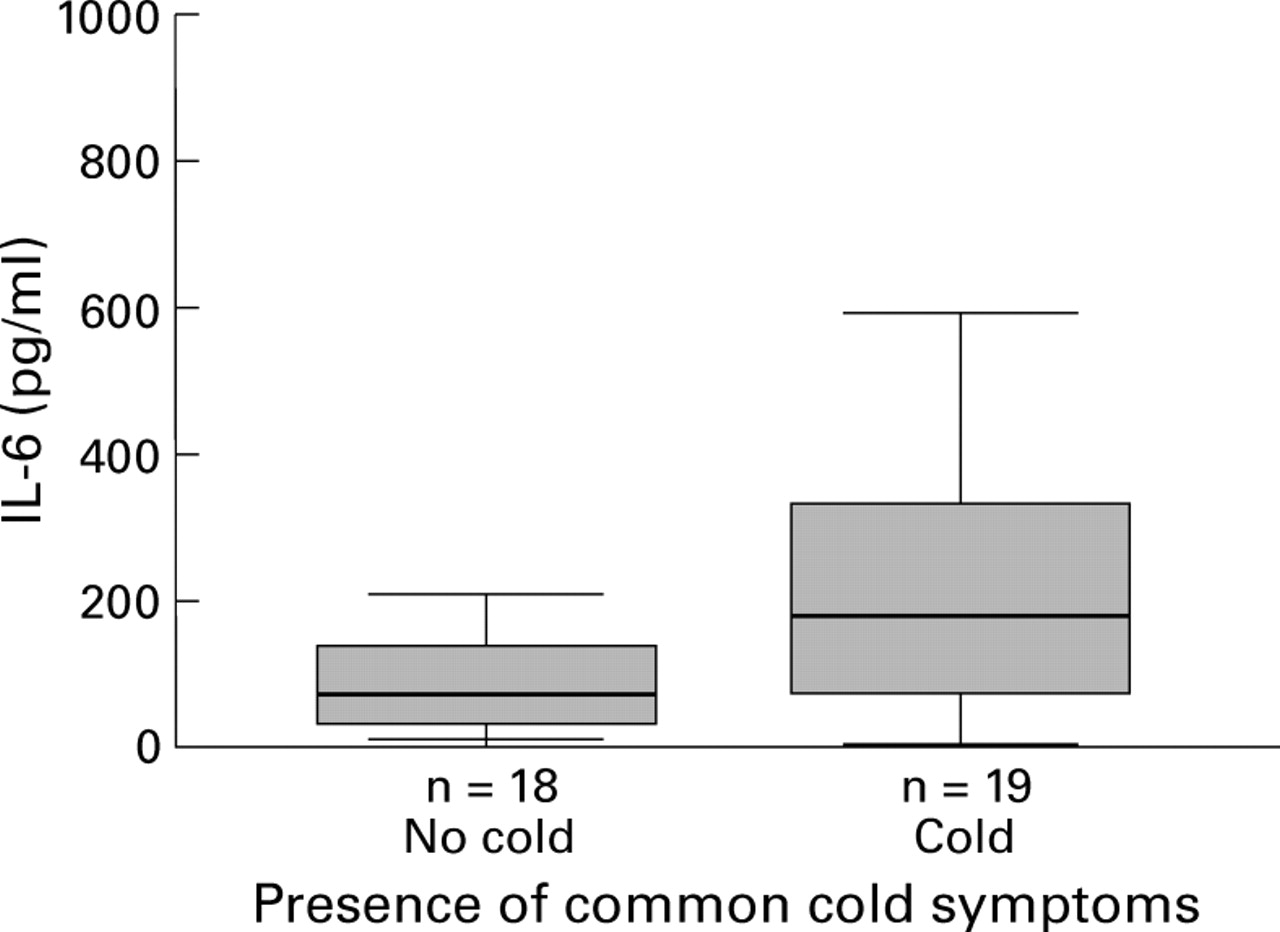
Thirty seven patients had data on exacerbations; data for only the first exacerbation was analysed for each patient to avoid bias in favour of frequent exacerbators. These patients had a median (IQR) of 3 (2–4) exacerbations in the previous year. For the 20 patients who had no exacerbation samples obtainable during the study, the number of exacerbations in the previous year was 2 (1–3.75) and there was no significant difference between the two groups. Patients were seen and sampled a median (IQR) of 3 (1—5) days after the onset of symptoms. Table 2 shows the results of the median IL-6, IL-8 values, and cell counts for the stable samples and the exacerbation samples obtained. The median IL-6 level was significantly higher at the time of an exacerbation (122.7 pg/ml) than during stable conditions (64.0 pg/ml; p< 0.05). The complaint of a common cold (rhinorrhoea and nasal congestion) was associated with increased sputum IL-6 levels (rho = 0.355, p = 0.031), the levels being 177.7 (50.1–344.6) pg/ml with a cold and 70.6 (26.9–138.6) pg/ml in the absence of a cold (fig 2). The differences in IL-8 levels and the cell counts between exacerbations and baseline values did not reach statistical significance (table 3). Those 11 patients in whom it was not possible to obtain stable samples had a median (IQR) IL-8 level of 4085 (1529–20 518) pg/ml which was no different from the group from which stable samples could be obtained (4383 (1401–10 900) pg/ml). Correlations between changes in cell numbers and sputum cytokine levels at exacerbations are shown in table 3. Differential counts could be obtained in 31 of the 37 sputum samples obtained. IL-6 levels were related to the total cell count, total eosinophil count, and total lymphocyte count at exacerbation while IL-8 levels were correlated with total cell count, neutrophil count, eosinophil count, and lymphocyte count.
Levels of IL-6, IL-8, total non-squamous cell count, neutrophil count, macrophage count, eosinophil count, and lymphocyte count in stable and exacerbation samples
{kind=link}
{kind=link}
Induced sputum levels of IL-6 in the absence and presence of a natural cold. Data expressed as medians (IQR).
Correlations between cells and cytokines at exacerbations (n = 31)
CHANGES IN SYMPTOMS AND LUNG FUNCTION
The mean (SD) baseline PEF was 239 (78) l/min which fell to 225 (73) l/min at the onset of an exacerbation (p<0.05). The mean (SD) FEV1 was 1.07 (0.26) l during stable conditions and 0.99 (0.31) l (p>0.05) at the time of the exacerbation visit. The cell counts and cytokine levels were not proportional to the changes in lung function. Patients had a median of 3 (2–3) symptoms (out of the major symptoms of increased dyspnoea, increased sputum volume, or purulence and the minor symptoms of colds, wheeze or chest tightness, sore throat, cough, or fever) on the day of onset whereas these patients had 0 (0–0) of the new/increased symptoms at baseline. The median (IQR) time taken for recovery of PEF to baseline levels was 7.15 (4.5–17.8) days and that for recovery of symptoms was 13.5 (7–16.5) days. There was no significant relationship between the recovery times for PEF and symptoms and the sputum cell and cytokine levels at exacerbation. The median IL-6 level in samples taken 3–6 weeks after an exacerbation (n = 22) was 94.6 (57.6–172.3) pg/ml and the IL-8 level was 5545 (2921–10 552) pg/ml. Those who had higher levels of sputum IL-6 or IL-8 in these post-exacerbation samples were not found to have more severe changes in lung function or symptoms with exacerbation (IL-6 and fall in PEF: rho = 0.145, p = 0.580; IL-6 and change in symptom score: 0.089, 0.734; IL-8 and fall in PEF: 0.150, 0.567; IL-8 and change in symptom score –0.110, 0.673).
Discussion
This is the first study to examine airway inflammatory markers prospectively in patients with COPD and to relate these to symptoms and physiological parameters, both when the patients were stable and during an exacerbation. Monitoring of these patients on a daily basis enabled us to determine accurately symptomatic and lung function changes associated with the exacerbation and to determine the exacerbation frequency which was similar to that previously reported by our group.1 Patients were instructed to call the study team as soon as they experienced symptomatic change and thus we were able to study patients early in the course of the exacerbation.
An important feature of this study was that we found a relation between the baseline induced sputum IL-6 and IL-8 levels and exacerbation frequency determined from the diary cards. We found increased sputum levels of IL-6 and IL-8 in patients with frequent exacerbations even though there was no relation between these cytokines and baseline lung function as has been reported in one study.6 However, there was a relation between the sputum IL-6 levels and years of cigarette smoking, perhaps due to the increased inflammation associated with prolonged smoking. IL-6 is produced by airway macrophages and bronchial epithelium while IL-8 is also largely produced by neutrophils and macrophages.11-13 The total cell count, neutrophil count, and macrophage count in the sputum were not increased in patients with more frequent exacerbations, which suggests that increased IL-6 and IL-8 expression in the sputum may be due to increased cytokine production by the bronchial epithelium. As expected, IL-8 levels were related to cell counts, both neutrophils and macrophages, but it is likely that a component of the increased sputum IL-8 level in patients with frequent exacerbations is produced by bronchial epithelial cells. Similarly, it is likely that the increase in IL-6 levels during an exacerbation might in part be due to production by the epithelial cells and is thus not proportional to the rise in total non-squamous cell count. Another factor increasing cytokine expression in frequent exacerbators could be the effect of bacterial colonisation. However, there is debate as to the exact role of the interaction between the airway and bacteria as an inflammatory stimulus in COPD.14 There may be a number of possible aetiologies for COPD exacerbations and these may have variable effects on cell counts in the airways.
Exacerbations are triggered by viral infections, especially by rhinovirus, which is responsible for the common cold.15 ,16 Rhinovirus has been shown to increase cytokine production in an epithelial cell line17 and thus repeated viral infection may lead to upregulation of airway cytokine expression. Exacerbations of COPD are also associated with bacterial infections such as Haemophilus influenzae andMoraxella cattarhalis 18 and cultures of bronchial epithelial cells showed increased IL-6 production in response to Haemophilus influenzaeendotoxin.19 An important factor for predicting frequent exacerbations is the number of exacerbations occurring in the previous year, and some patients are more susceptible to exacerbations.1 ,20 Thus, measurement of the cytokines IL-6 and IL-8 in sputum can determine which COPD patients are susceptible to frequent exacerbations so that appropriate education and treatment can be planned. Patients with an increased exacerbation frequency showed worse quality of life scores1 than patients with infrequent exacerbations, although there is little relation between quality of life in COPD and FEV1.21 ,22 The presence of increased inflammatory markers in the sputum may therefore have an important effect on health status in COPD.
At the time of an exacerbation we found that sputum levels of IL-6 increased, though rises in IL-8 were more variable and did not reach statistical significance. Levels of IL-6 in the sputum were higher in patients when the exacerbations were associated with symptoms of a natural cold, although there were no other relationships observed with individual symptoms and either IL-6 or IL-8 levels. The levels of IL-8 were related to the sputum neutrophil and total cell counts, suggesting that neutrophil recruitment is the major source of IL-8 during an exacerbation. Although there were some rises in sputum cell counts at the time of an exacerbation, there was individual variability and, overall, the cell count showed no change. There was also no relation between the sputum cellular response at exacerbation and symptoms of a cold. Thus, there is considerable heterogeneity in the degree of the inflammatory response at the time of a COPD exacerbation.
In patients with asthma a recent study found that, compared with healthy subjects with colds, exacerbations were associated with a much higher cell count in the sputum, predominantly neutrophilic.23 However, the asthma exacerbations were all associated with influenza while the healthy subjects had viruses such as rhinovirus and coronavirus that are associated with common colds.24 Our COPD patients had all received influenza immunisation and thus it is unlikely that influenza was a trigger of the exacerbations in this study. Exacerbations of COPD were associated with a lower and more variable inflammatory response than in patients with asthma.3 ,23 ,25 This may explain the less pronounced response to steroids during exacerbations of COPD than during exacerbations of asthma.26 ,27 A recent study has suggested that sputum eosinophilia may predict benefit from prednisolone when used in stable COPD patients,28 though there are no studies of the predictive factors for steroid treatment of COPD exacerbations.
Unlike a previous report, we did not detect a rise in eosinophil count in our patients at the time of an exacerbation even though the patients were sampled early and exacerbations were defined on strict criteria.4 In the previous study by Saetta and colleagues, where rises in sputum eosinophils were found during exacerbations, patients had chronic bronchitis with mild airflow obstruction while our patients had moderate to severe COPD with a mean FEV1 of 39.5% predicted. It is possible that the inflammatory response during an exacerbation is different in patients with more severe COPD. Again, in the study by Saetta et al 4the FEV1 fell from 76% predicted to 62% predicted, which is larger than the changes in our study and suggests that some of their patients had reversible airways obstruction.
As the patients in our study were followed prospectively with daily monitoring, we were able to obtain data on recovery from an exacerbation. There was no relation between the sputum cytokine level and degree of inflammatory cell response at exacerbation and the length of the exacerbation symptoms or physiological changes. In the group of patients in whom induced sputum was taken at 3–6 weeks after an exacerbation, again there was no relation between the post-exacerbation cytokine levels and changes caused by the exacerbation. Levels of inflammatory markers in induced sputum at exacerbation do not predict the subsequent course or severity of an exacerbation and thus will be of limited use as a short term outcome measure in the setting of a clinical study. However, this study involved exacerbations in subjects treated as outpatients and an association between sputum markers and the course of the exacerbation may be found in those with more severe exacerbations requiring hospital admission.
This study shows that patients who have frequent exacerbations have increased airway cytokine levels when stable which rise further during an exacerbation, especially in the case of IL-6. COPD is characterised by a progressive decline in FEV1 caused by chronic airway inflammation. Our data suggest that frequent exacerbations may increase airway inflammation and thus could contribute to the decline in lung function. However, previous studies on the influence of exacerbations on long term respiratory function have provided conflicting results.29 ,30 Further study is required of the relationship between frequency of exacerbations, airway inflammation, infection, and long term changes in lung function. Prevention of exacerbations and a reduction in their frequency may have a considerable benefit on the health burden in patients with COPD
Acknowledgments
The authors thank Dr G C Donaldson for his help in data analysis and DeVilbiss Healthcare for the loan of the Ultraneb 2000 nebuliser used in this study.