Article Text

Statistics from Altmetric.com
Chronic obstructive pulmonary disease (COPD) is a major cause of ill health and death in adults and straddles the interface between primary and secondary care. There are at least 600 000 people in the UK with COPD, a prevalence of around 1%. The diagnosis is usually made relatively late in the natural history, after the age of 40, when symptoms start to appear.1 The prevalence rises to approximately 5% of men aged 65–74 and 10% of men older than 75. Historically, more men have been affected but women are rapidly catching up. Prevalence figures for COPD from Denmark, where women have smoked longer than men, show that the prevalence is now equal.2 COPD is the fifth most common cause of death in the UK, causing 5.4% of male and 3.2% of female deaths, and is a contributory factor on a further 4% of death certificates.3 In a typical district health authority with a population of 250 000, consultations with general practitioners (GPs) for COPD are similar in number to asthma but more patients with COPD will be admitted to hospital and they will stay in hospital for approximately three times as long . The mortality caused by COPD is at least 14 times that of asthma. It is reaching almost epidemic proportions in the Third World, principally as a result of increased tobacco consumption.4
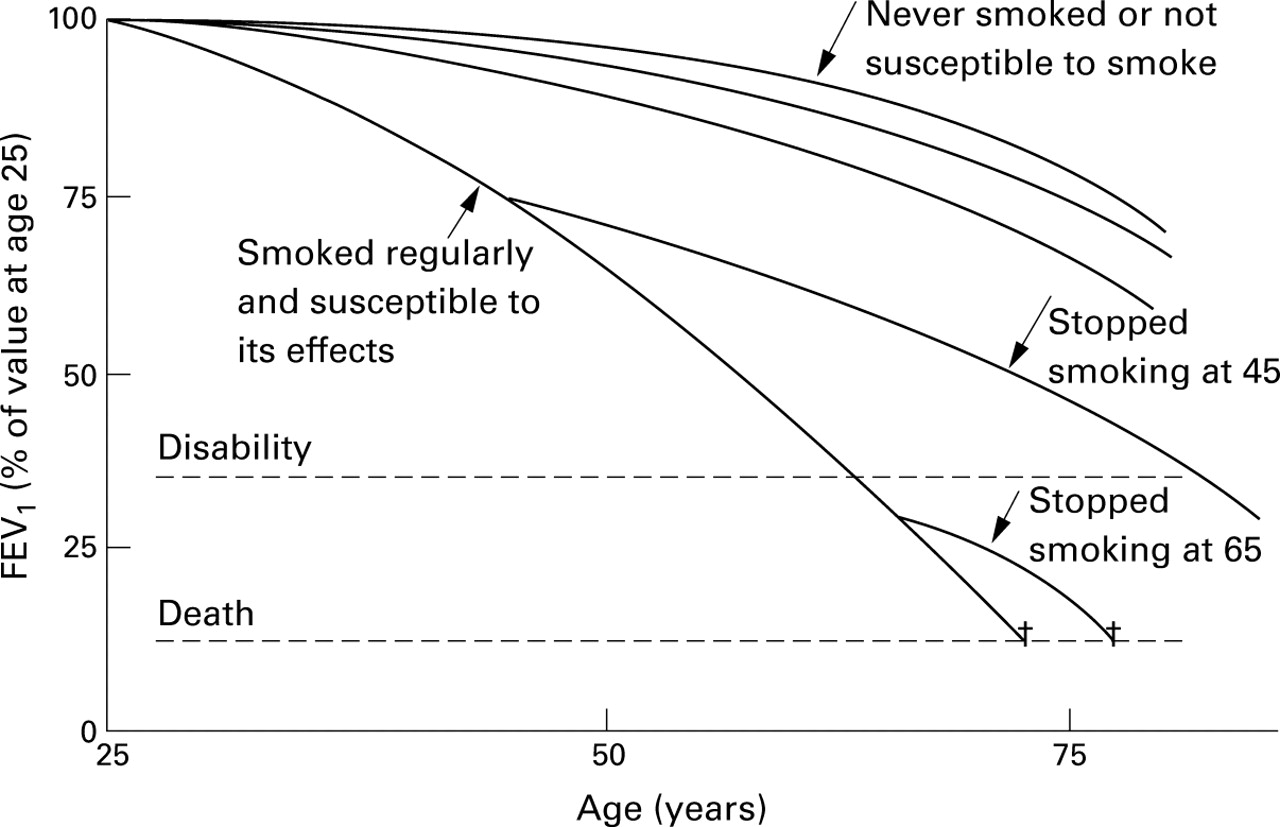
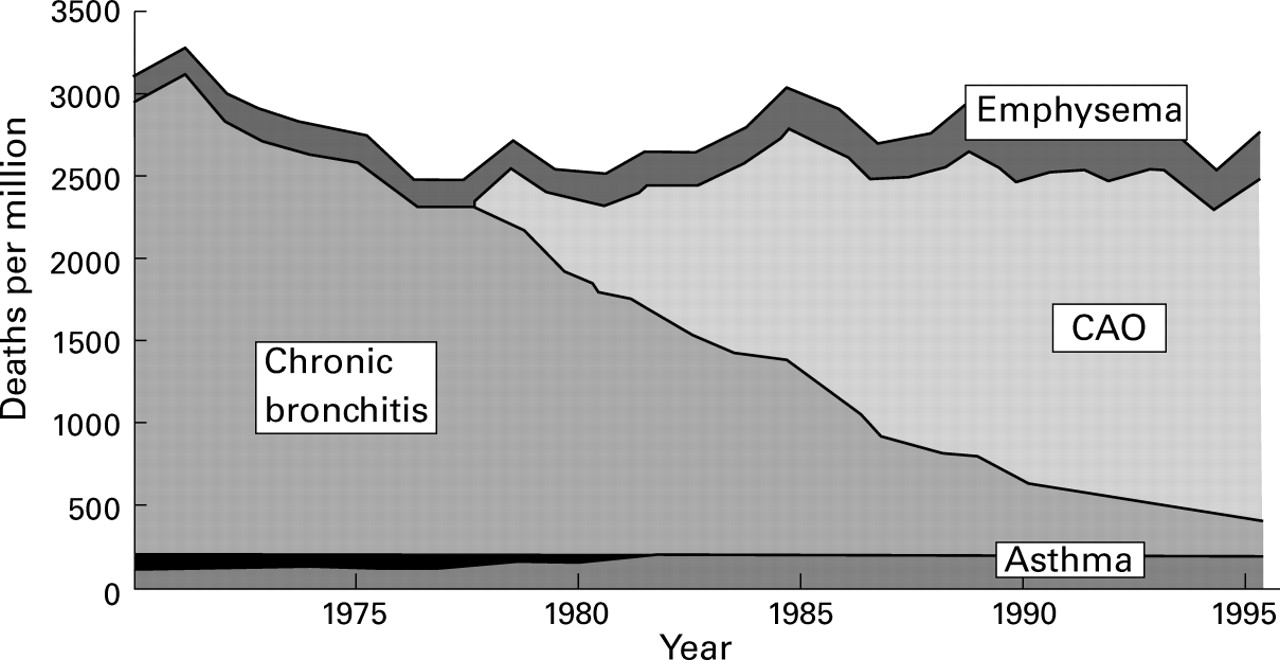
Despite progress in reducing cigarette smoking, the mortality from COPD in the UK has remained constant for the last 20 years (fig 1). Figure 2illustrates some theoretical rates of decline of lung function (and hence disease progression). Approximately 20% of cigarette smokers are susceptible to progressive lung damage for reasons which remain unclear. The accelerated loss of lung function declines when they quit smoking, even in advanced disease. However, the absolute loss of function persists and, even with a relatively normal rate of decline in forced expiratory volume in one second (FEV1) after quitting, significant disability occurs as the patient ages and it is often an important reason for loss of independence in the elderly.
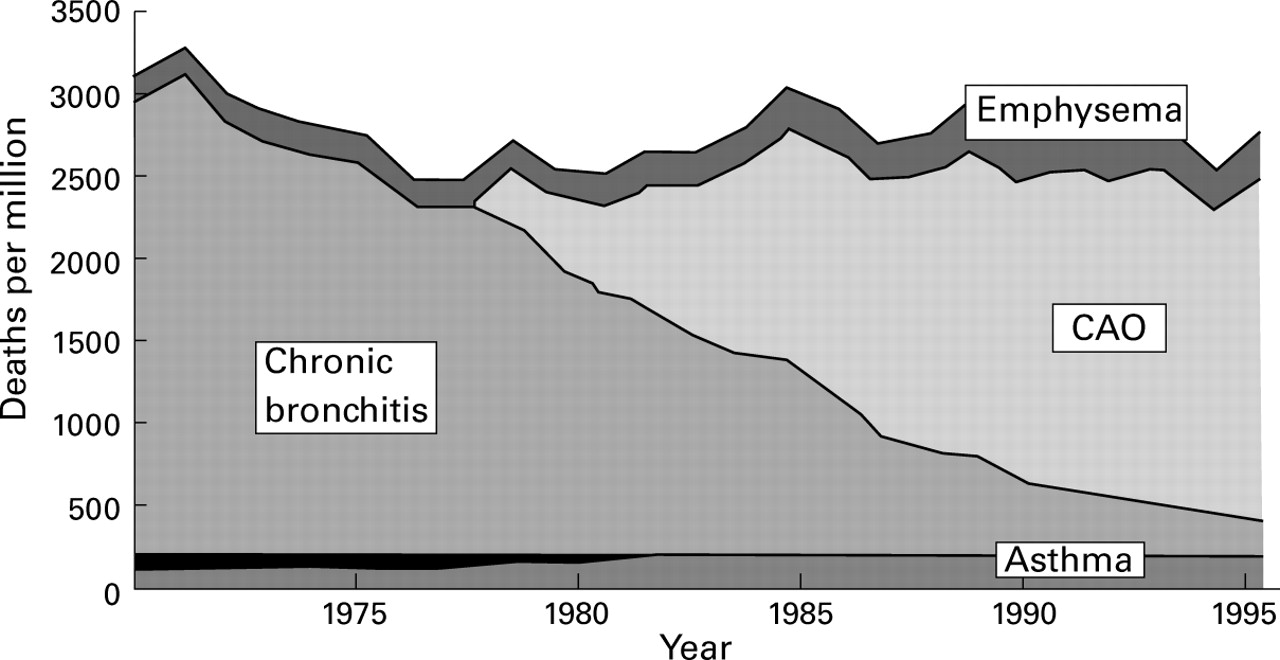
Mortality data from COPD in the UK in patients aged 65−84 years. Note that although the diagnostic label has changed, the overall death rate due to COPD has remained relatively constant over the last 10 years. CAO = chronic airways obstruction. Data derived from the Lung and Asthma Information Agency.
{kind=link}
{kind=link}
Schematic representation of theoretical decline in FEV1 with age. These data emphasise the variable rate at which disability and death are reached in the existence of a potentially “susceptible” population in whom the rate of decline in lung function is more rapid. Stopping smoking appears to be beneficial at all stages of the disease.
Despite its clinical and economic importance, COPD remains poorly understood and underdiagnosed. Studies from the UK and Europe suggest that at least half of those affected with COPD are undiagnosed. This is due to several factors. Milder COPD is relatively asymptomatic and patients see a “smokers' cough” or breathlessness as commensurate with smoking. Few GPs as yet perform screening with spirometry on at risk populations (smokers over 40) due to inadequate training and resources.
Certainly, there is little incentive for GPs to identify COPD systematically and to distinguish it from other respiratory disorders. Prescribing approaches are influenced as much by the age and social class of the patient as they are by any objective diagnostic criteria.5 There remains a strong feeling in both primary and secondary care that nothing can be done for these patients other than stopping smoking, advice which is often unwelcome. Blaming the patients for their plight is therefore attractive.
It is important that we should move away from the concept of a single therapeutic intervention towards overall patient management, involving not only smoking cessation and drug prescription but also encouraging greater exercise and attending to psychological and social well being. This is reflected in the British Thoracic Society guidelines which are a convenient source of reference in planning the care of patients with COPD.3
Diagnosis
COPD is now defined differently from previous symptomatic and pathological definitions. The key elements are summarised in the box. COPD almost certainly represents a mixture of pathological processes modified by different degrees of genetically determined host susceptibility. Some of these variants may pursue a sufficiently discrete and characteristic course that, with better cellular and biochemical markers, we may be able to define them as separate diseases. However, our existing tools do not make such a clear distinction possible or even very helpful. Although the term chronic obstructive pulmonary disease may not be perfect, it is likely to remain in use for the foreseeable future and should be encouraged.
Definitions and diagnosis
Chronic obstructive pulmonary disease is a chronic, slowly progressive disorder characterised by airways obstruction (FEV1 <80% predicted and FEV1/FVC ratio <70%) which does not change markedly over several months. The impairment of lung function is largely fixed but is partially reversible by bronchodilator (or other) therapy. In clinical practice the diagnosis involves:
A history of chronic progressive symptoms (cough and/or wheeze and/or breathlessness).
Objective evidence of airways obstruction that does not return to normal with treatment.
Usually a smoking history of more than 20 pack years.
The most important initial step in diagnosis is to consider the possibility of COPD. In most cases the patients will be current or ex-cigarette smokers, often having consumed 20 or more pack years. They will be over the age of 40 and are likely to have attended before with respiratory infections.5 They may not meet all the traditional criteria for chronic bronchitis (a productive cough for at least three months for two consecutive years) but usually have a persistent “smokers' cough”. Breathlessness often precipitates the consultation, either exacerbated by an upper respiratory tract infection or being finally perceived by the patients as affecting their lifestyle.6 The slow pace of development of symptoms mitigates against early diagnosis as the patient first modifies his or her life style—for example, walking more slowly—and is not surprised by the symptoms of breathlessness or cough which are attributed to smoking or “ageing”. They will often have noted similar symptoms amongst fellow sufferers and their smoking parents. Social and health expectations are important determinants both of the prevalence and delayed diagnosis of this illness.7
Confirming the diagnosis requires spirometric tests, ideally before and after an inhaled bronchodilator. This need be performed only once, and has several clear advantages:
- (1)
- it is accurate and, if normal, it excludes COPD;
- (2)
- it helps to exclude significant co-existing asthma in the majority of cases but occasionally a steroid trial may be necessary in addition; and
- (3)
- it can be repeated intermittently to monitor progress.
Measurement of peak expiratory flow (PEF) is familiar and widely available but can grossly underestimate the disease severity and is much more prone to error than measuring FEV1.8 ,9 Serial PEF data are lacking in COPD which makes interpretation of significant changes difficult. Small changes in FEV1 (200–400 ml) after acute treatment with a β agonist and/or ipratropium are relatively common in COPD. Larger changes point to a significant asthmatic element and treatment should then follow the BTS asthma guidelines.10
Spirometers are increasingly used in primary care with measurements being made by both GPs and practice nurses. It is essential that correct technique and interpretation of results is taught and understood. Spirometry courses are available and many practice nurses, especially those familiar with asthma management, can take on this role with good effect. Alternatively, where geographically appropriate, hospital pulmonary function departments should consider open access services as cardiologists have done with ECGs for many years. Reports should be pertinent and helpful and should use terms with which the local GPs are familiar, suggesting further investigations, treatment options, and referral where appropriate. Respiratory physicians should not complain about poor recognition of COPD in primary care if GPs are denied access to the tools needed for diagnosis.
Treatment
The potential and limitations of current treatment are summarised in the BTS guidelines on the management of COPD.3 Our purpose here is to address some of the specific implications of treatment in primary care and to highlight some changes likely to occur in the management of COPD as a result of recent research.
SMOKING CESSATION
Smoking cessation is central to modifying the natural history of COPD but remains a difficult goal. Nicotine is the principal addictive element in tobacco. Dependency varies but can be at least as great as in illicit drug use. Several key points are now well established11:
- (1)
- quitting smoking is much more likely when the patients have mentally reached the stage where they wish to do so—the “state of change” model;
- (2)
- withdrawal symptoms can be significantly reduced by nicotine replacement treatment (NRT) such as patches, gum or spray. Higher doses of NRT tend to be more effective than low doses in most patients;
- (3)
- new drugs under investigation may enhance quit rates. Bupropion, licensed in the USA, increases the sustained quit rate and its effect appears to be additive to NRT12;
- (4)
- quitters who smoke cigarettes within a week of trying to give up will fail. Patients needing a cigarette within 30 minutes of waking and before they get out of bed have high nicotine dependence.
Smoking cessation clinics have been conducted in primary care, usually by practice nurses, for many years. Sustained quit rates of 10–15% are understandably disappointing for doctors, but represent a cheap, cost effective intervention13 that halves the rate of FEV1 decline and compares favourably with available drug treatments.
BRONCHODILATORS
Regular inhaled bronchodilators remain central to the treatment of symptomatic COPD. Short acting bronchodilators can and should be used regularly and in high doses for more severe COPD. In asthma the recommendation to use short acting β agonists only as required arose from concerns over safety. Their use in COPD, however, is wholly appropriate and beneficial and there are no reported safety issues. Satisfactory combination inhalers containing both β agonist and anticholinergic agents are available but unfortunately only as metered dose inhalers. Long acting inhaled β agonists appear to be more beneficial than initially thought with evidence that quality of life measured in a number of ways can be improved.14 Long acting inhaled anticholinergic drugs are awaited with interest. The use of oral theophylline is limited by side effects but newer phosphodiesterase 4 (PDE4) inhibitors show some promise as a possible replacement with some anti-inflammatory activity.
There are now clear scientific data showing that improvements in symptoms and exercise performance in COPD correlate poorly with short term post-bronchodilator changes in FEV1 but result from a reduction in the amount of dynamic hyperinflation. This relatively recent concept is important in understanding a number of clinical features of COPD. Expiration is prolonged and patients need to take their next breath before the previous one has finished. Thus, they breathe at a higher lung volume than is comfortable, particularly during exercise. Bronchodilator drugs can reduce this problem without necessarily modifying tests of forced expiration such as FEV1. Changes in forced vital capacity (FVC) or a relaxed VC may act as a measurable indicator. In practice, patients should be given a few weeks trial of regular inhaled bronchodilators and asked to note any improvements in breathlessness, chest tightness, and exercise tolerance. The patient's report of such treatment may be more valuable than quantitative changes in FEV1.
Nebulisers have a useful role in very severe COPD but their appropriateness should be assessed by a respiratory specialist, as explained in the BTS nebuliser guidelines.15 Patients should have tried high dose bronchodilators via a large volume spacer before commencing long term nebuliser therapy.
INHALED CORTICOSTEROIDS
There is continuing controversy about these drugs but data from several unpublished studies may clarify their role in COPD.16 The results of both the Copenhagen and EUROSCOP studies suggest that treatment with inhaled corticosteroids does not modify the rate of decline of lung function when given early in the disease. The same appears to be true even in those patients with more severe disease included in the ISOLDE study. However, the ISOLDE study found a significant reduction in the number of exacerbations and an amelioration of the deterioration in quality of life when patients with COPD were treated with high dose inhaled corticosteroids. A recent meta-analysis17 of inhaled corticosteroids on lung function has suggested that there may be a dose effect in that only higher doses (beclomethasone 1500 μg per day or equivalent) have any measurable effect. More information is required to help interpret these findings. These data call into question the previous recommendations about the need for a trial of oral corticosteroids before commencing patients on inhaled treatment but further discussion is needed before this approach can be completely abandoned.
PULMONARY REHABILITATION
There is now very strong evidence that pulmonary rehabilitation improves exercise performance and reduces breathlessness in patients with moderate to severe COPD.18 ,19 More is now known about exercise limitation due to peripheral muscle weakness. Affected individuals are more likely to use health care resources than similar patients without muscle weakness.20 Specific cellular and metabolic abnormalities have been identified in the limb muscles of patients with COPD and these do not seem to be simply a consequence of lack of activity. Rehabilitation improves overall exercise performance and reverses some of these peripheral muscle problems. Patients most likely to benefit appear to be those with an FEV1 between 30% and 50% predicted. In the UK most of these patients are known to their GPs but not necessarily to hospital physicians.
Unfortunately there are few rehabilitation units available and most GPs will have no local access. Developing an appropriate referral pattern for rehabilitation, sharing the resources of primary and secondary care, is a major task for the next few years.
Nevertheless, it is important to inform and discuss the merits of regular exercise with COPD patients in primary care. Simple and quick advice might include suggesting that patients walk regularly to the point of being breathless and over a period of weeks to steadily increase the distance walked, perhaps using the number of lamp posts as a guide. Many patients and their relatives are very anxious about being breathless, assuming this may be harming their heart and lungs. Strong reassurance and permission to be breathless is required and regularly repeated at follow up visits. Leaflets giving information on exercises and lifestyle will reinforce advice.
OXYGEN
Long term oxygen therapy (LTOT) has been shown to improve survival and quality of life in selected patients.21 Many who might benefit from LTOT are not being referred to chest physicians for assessment. GP prescribing of oxygen is predominantly by cylinders which, if used for many hours a day, cost over six times the amount of oxygen concentrator maintenance. GPs require more education on indications for referral for LTOT. One possible role of primary care groups might be the introduction of pulse oximeters which could be used for the measurement of oxygen saturation in patients with more severe COPD. A study by Roberts et al 22 on the use of pulse oximetry in primary care found that an oxygen saturation below 92%, when patients are in a stable phase, was helpful in deciding when to refer for consideration of LTOT. When arterial saturation is unavailable patients should be considered for referral when they have severe COPD (FEV1<1.5 litres), are cyanosed, and/or have signs of cor pulmonale.
ACUTE EXACERBATIONS
Many patients with more severe COPD experience regular exacerbations of their symptoms, particularly during the winter months. Common symptoms of exacerbations are sputum purulence, increases in sputum volume, breathlessness, wheeze, and chest tightness. Exacerbations can broadly be of two kinds: (1) infective (characterised by change in sputum colour and possibly pyrexia); and (2) changed lung mechanics and increased airflow obstruction (characterised by dyspnoea without evidence of infection). Both patterns may occur together and the cause of worsening lung function is often not clear.
Management in the community usually involves increasing bronchodilator use and, with signs of infection, a course of appropriate antibiotics. In those patients where there is increased breathlessness and wheezing a course of prednisolone, 30 mg per day for 1–2 weeks, is likely to be beneficial. The decision as to the need to admit the patient to hospital will be influenced by the severity of symptoms, the ability to cope at home, and the knowledge of the patient's past medical history. Patients with more severe COPD may have repeated hospital admissions and a discharge plan involving a multidisciplinary approach is required to optimise both clinical and social circumstances.
EDUCATION AND PATIENT INVOLVEMENT
Although COPD is a common condition its diagnosis, differentiation from asthma, and appropriate management have been largely neglected. The BTS guidelines address gaps in knowledge. Dissemination to doctors and nurses in primary care using a four page easily digested summary should have secured a higher level of awareness but the proven impact of guidelines is generally disappointing. Further and repeated education is needed to raise the levels of understanding and management to those of asthma. The BTS COPD consortium, sponsored by a large number of pharmaceutical and equipment manufacturers, continues to provide educational initiatives, particularly to primary care.
Many courses on COPD and spirometry for practice nurses are now available. Local lung function units should also be encouraged to provide teaching on spirometry. Primary care groups and clinical governance initiatives should also encourage more dissemination of good practice and wider use of spirometers. Expertise amongst GPs and practice nurses could be shared within the group.
Self-management plans have been shown to improve significantly many clinical outcomes in asthma. Only limited data are available about self-management plans in COPD which require testing in controlled trials. A possible plan might include patient participation and education in (1) increasing bronchodilators with increasing symptoms, (2) taking courses of antibiotics for infective symptoms, and (3) initiating a course of prednisolone. A written plan drawn up jointly with the patient would be necessary, with safeguards to call a GP if symptoms became worse. It remains to be tested if this approach would reduce hospital admissions, time off work, and duration of attacks. The only published controlled study of self-management23 in primary care showed no differences in symptoms but the overall quality of life score improved with time in the intervention group.
Implementation of change in primary care
As with asthma, COPD should be managed predominantly in primary care. However, a huge educational input at all levels of the Health Service is needed to provide the necessary resources, time, staff, and direction to diagnose and manage this important disease effectively.
In primary care some of the most pressing requirements are to be aware of COPD and its diagnosis, to search for COPD patients amongst older asthmatics, particularly if they smoke, to screen smokers over the age of 40 years, to perform spirometric tests, to adopt a positive approach to management, adopting an overall package of care, to change the mood and social circumstances of COPD patients, to involve patients and carers, and to encourage regular review as part of routine care.
The future
COPD is a major clinical problem for both general practitioners and hospital physicians. More information is needed if we are to develop rational care plans that maximise the use of scarce resources. Key areas to be considered are:
- (1)
- better data about the true prevalence of the disease in primary care;
- (2)
- better data about the cost effectiveness of different treatment options in COPD;
- (3)
- further information about how best to implement treatment guidelines and evaluate their efficacy;
- (4)
- new ways of identifying patients in need of rehabilitation and providing cost effective treatment;
- (5)
- assessing the impact of early discharge from hospital or care in the community on exacerbations of COPD.
The following three questions merit further study:
What is the role of spirometry as a screening tool? Is it cost beneficial to screen smokers over the age of 40? Will the finding of abnormal lung function increase smoking quit rates? Will patients with slightly low lung function be treated unnecessarily?
What are the best ways of identifying patients for rehabilitation in the community? Can effective rehabilitation be delivered to a wider group of patients without the need for specialist centres?
Can self-management plans for COPD be devised that are as beneficial as those for asthma? Controlled studies need to look at symptoms, exacerbations, hospital admissions, and quality of life.