Article Text

Abstract
BACKGROUND A study was undertaken to establish the chronic effect of initial and recurrent treated pulmonary tuberculosis on impairment of lung function.
METHODS A total of 27 660 black South African gold miners who had reliable pulmonary function tests from January 1995 to August 1996 were retrospectively followed for the incidence of pulmonary tuberculosis to 1970. The lung function measurements in 1995–6 were related to the number of previous episodes of tuberculosis and to the time that had lapsed from the diagnosis of the last episode of tuberculosis to the lung function test. Miners without tuberculosis or pneumoconiosis served as a comparison group.
RESULTS There were 2137 miners who had one episode of tuberculosis, 366 who had two, and 96 who had three or more episodes. The average time between the diagnosis of the last episode of tuberculosis and the lung function test was 4.6 years (range one month to 31 years). The loss of lung function was highest within six months of the diagnosis of tuberculosis and stabilised after 12 months when the loss was considered to be chronic. The estimated average chronic deficit in forced expiratory volume in one second (FEV1) after one, two, and three or more episodes of tuberculosis was 153 ml, 326 ml, and 410 ml, respectively. The corresponding deficits for forced vital capacity (FVC) were 96 ml, 286 ml, and 345 ml. The loss of function due to tuberculosis was not biased by the presence of HIV as HIV positive and HIV negative subjects had similar losses. The percentage of subjects with chronic airflow impairment (FEV1 <80% predicted) was 18.4% in those with one episode, 27.1% in those with two, and 35.2% in those with three or more episodes of tuberculosis.
CONCLUSIONS Tuberculosis can cause chronic impairment of lung function which increases incrementally with the number of episodes of tuberculosis. Clearly, prevention of tuberculosis and its effect on lung function is important and can be achieved by early detection and by reduction of the risk of tuberculosis through intervention on risk factors such as HIV, silica dust exposure, silicosis, and socioeconomic factors.
- chronic lung function impairment
- tuberculosis
- silica dust
Statistics from Altmetric.com
Several studies have shown that early and partially treated pulmonary tuberculosis can result in airflow obstruction.1-5 Studies with longer follow up have shown that a large percentage of cases with treated pulmonary tuberculosis have evidence of permanent airflow obstruction or restrictive impairment.6-8 There are no published studies in which the effect of recurrent episodes of treated pulmonary tuberculosis on lung function impairment have been evaluated.
The South African gold mining industry employs over 300 000 miners. The risk factors for tuberculosis in gold miners include exposure to silica dust,9 ,10 silicosis,10-12 HIV infection,13 socioeconomic factors, and the high risk of tuberculosis in the general South African population. Prior to 1992 the incidence of tuberculosis among working gold miners was stable but high (of the order of 500 smear and/or culture positive cases per 100 000 person years). With the advent of HIV the incidence of tuberculosis has been rising consistently and currently is in excess of 2000 cases per 100 000 population.14 The mines have active and passive case finding programmes and the treatment of tuberculosis follows the World Health Organisation standards. Before 1980 miners who developed pulmonary tuberculosis were not allowed to return to underground mining but, with the introduction of more effective tuberculosis treatment in the early 1980s, most miners return to underground mining when physically fit to do so.
The main objective of this study was to estimate the effect of treated initial and recurrent tuberculosis on the loss of lung function, especially the chronic effect—that is, the residual deficit in lung function. Specifically, we evaluated (1) the effect of the number of treated tuberculosis episodes on loss of lung function; (2) the effect on loss of lung function of time between the last episode of tuberculosis and the lung function test; (3) the confounding effect of HIV on the loss of lung function due to tuberculosis; and (4) the proportion of subjects with chronic airflow impairment (FEV1 <80% predicted), according to the number of tuberculosis episodes, in subjects with over 18 months between the last episode of tuberculosis and the lung function test.
Methods
The study was performed on 27 660 black South African gold miners employed by a large gold mining company in whom pulmonary function tests were carried out during the period from January 1995 to August 1996. For these miners the incidence of pulmonary tuberculosis was ascertained retrospectively to 1970.
TUBERCULOSIS CASE DETECTION
The company has an active case finding programme through yearly mass miniature radiographic (MMR) screening. In patients with abnormal radiographs standard size chest radiographs are taken. Three sputum specimens are collected for microscopic examination and culture from those with suspected tuberculosis. All sputum specimens are decontaminated, concentrated, and stained with auramine and Ziehl-Neelsen for microscopic examination and culture on Lowenstein Jensen slants in the hospital laboratory.13 Initial identification is done by the local laboratory. From 1994 the AccuprobeMycobacterium tuberculosis complex culture identification test (Gen-Probe Inc, San Diego, USA), a rapid DNA probe test which uses the technique of nucleic acid hybridisation for the identification of M tuberculosis complex species, has been used to distinguish M tuberculosis from other mycobacteria. The diagnosis of tuberculosis is based on radiological, clinical, and bacteriological results using a validated scoring system,14 in accordance with the standard case definition used by the South African national tuberculosis programme. On entry into the employment the miners are interviewed for a previous history of tuberculosis. Of the tuberculosis cases, 0.3% reported one and 0.001% reported more than one history of tuberculosis diagnosed before employment in the mines. The company has computerised records of all tuberculosis episodes on all miners from 1970.
HIV TESTING
Patients with suspected tuberculosis are offered voluntary HIV testing with counselling before and after the test. HIV is diagnosed if both the screening (Enzymun-test Anti-HIV 1+2+subtype O, Boehringer Mannheim Immunodiagnostics) and confirmatory (Elisa IM system HIV-1/HIV-2 III Plus, Abbott) diagnostic tests are positive.
DETECTION OF PNEUMOCONIOSIS
Miners whose radiographs are identified as abnormal during yearly MMR screening undergo standard chest radiography. The identity of subjects diagnosed as having silicosis category 1/1 and above according to the ILO category on standard radiographs has been recorded cross sectionally on a computerised database since 1994. These data were used for the present study.
LUNG FUNCTION SCREENING
Lung function screening was introduced in 1994. Spirometric tests are performed routinely on all miners at an initial examination, periodically at three yearly intervals, and on leaving the industry. Maximal forced expiratory manoeuvres are recorded in a computerised database using a Hans Rudolph pneumotachograph (Flowscan, Electromedical Systems Inc). The system software requires and validates calibration with a three litre syringe. Barometric pressure and temperature are entered via the keyboard for correction of volumes to BTPS. During testing, flow versus volume tracings are displayed. A minimum of three acceptable and reproducible forced expiratory manoeuvres are obtained according to the standards recommended by the American Thoracic Society (ATS). All testing is done by nursing personnel trained in the techniques of performing spirometric tests to ATS standards. Height is measured to the nearest centimetre in stockinged feet. Data computerised for each test include date of test, date of birth, height, weight, the highest forced vital capacity (FVC), highest forced expiratory volume in one second (FEV1), and forced expiratory flow at 25–75% of forced vital capacity (FEV25–75%). In a reliability study we excluded outliers outside the 99.98% confidence interval (CI) of the mean (p<0.0001) and established that lung function tests were most reliable from January 1995 to August 1996 (reliability coefficient G = 0.94).15 Using the data from this period we also estimated predictive lung function curves for miners without a previous history of tuberculosis or pneumoconiosis and found these to be almost identical to those estimated on non-smoking and non-symptomatic black South African men not exposed to dust.16
SUBJECT SELECTION
The 27 660 miners comprised all those who had a periodical or exit lung function examination during the reliable testing period (January 1995 to August 1996)15 and whose lung function measurements were within the 99.98% CI of the mean value. Only one lung function test per miner was used, and the tuberculosis history and pneumoconiosis status prior to the lung function test were established. There were 18 754 periodic examinations and 8906 exit examinations. In a preliminary analysis we analysed the two types of examinations separately and established that the results were very similar, and thus the two were combined.
STATISTICAL ANALYSIS
For the descriptive analysis we standardised lung function tests for height of 1.70 m and tabulated the observed and predicted lung function tests using prediction equations calculated on miners without tuberculosis or pneumoconiosis. The linear regression model was used to estimate the effect of the number of episodes of tuberculosis and the time lapsed from the last episode of tuberculosis on lung function (LF) as follows:

where the dichotomous (0,1) variables episode,i = 3, 4, 5 represent one, two, three or more episodes of tuberculosis, respectively, and the dichotomous variables time, i = 6, 7, . . ., 13 represent lapsed time of 6 months, 7–12 months, 13–18 months, 19–24 months, 1–2.9 years, 3–3.9 years, 4–4.9 years, and 6 or more years, respectively. For example, for a person with two episodes of tuberculosis and a time lapse of 7–12 months, the variables episode4 = 1 and time7 = 1 while all the other dichotomous variables are equal to zero.
To establish whether HIV is a confounding factor we estimated the effect of tuberculosis episodes in HIV positive and HIV negative subjects. A comparison group used throughout the analysis comprised subjects who did not have a history of tuberculosis or pneumoconiosis. The percentage of subjects with chronic airflow impairment, defined as FEV1 <80% predicted,17 was established in subjects with a time lapse of more than 18 months—that is, the time when the loss of lung function due to tuberculosis was found to stabilise.
Results
Of the 27 660 miners, 23 712 had neither pneumoconiosis nor tuberculosis, 2599 had a history of tuberculosis, and 1349 miners had pneumoconiosis of whom 185 had tuberculosis also. Of the 2599 miners with tuberculosis only, 2137 had one episode, 366 had two episodes, 79 had three episodes, and 17 had four or more episodes. Tables 1 and 2show the observed and percentage predicted mean values for height adjusted FVC and FEV1 according to the number of episodes of tuberculosis for five year age categories for subjects who did not have radiological changes for pneumoconiosis. A consistent decrease with episodes of tuberculosis is apparent for all age categories.
Mean observed (in litres) and percentage predicted values of forced vital capacity (FVC) according to the number of episodes of tuberculosis
Mean observed (in litres) and percentage predicted values of forced expiratory volume in one second (FEV1) according to the number of episodes of tuberculosis
Table 3 shows the age and height adjusted regression coefficients β and standard errors (SE) for each of the lung function tests (FVC, FEV1, FEV1% and FEF25–75%). The regression coefficients represent the decrease in lung function in litres in subjects with increasing number of tuberculosis episodes, in subjects with pneumoconiosis and any number of tuberculosis episodes, and in subjects with pneumoconiosis only compared with subjects who did not have tuberculosis or pneumoconiosis (the baseline group). For example, the FEV1 decreased by an average of 180 ml in those with one episode of tuberculosis, by 362 ml in those with two episodes, by 462 ml in those with three episodes, and by 964 ml in those with four or more episodes. Subjects with pneumoconiosis and a recorded history of tuberculosis had a decrease of 384 ml while those with pneumoconiosis only had a decrease of 215 ml. The prediction equations for the baseline group were: FVC = –2.901 − 0.025 × age + 4.655 × height; FEV1 = –1.654 − 0.030 × age + 3.665 × height (age in years and height in metres).
Age and height adjusted regression coefficients β and standard errors (SE) for lung function tests for 27 660 miners
Table 4 shows the age and height adjusted regression coefficients and standard errors for the number of tuberculosis episodes (three and more episodes were combined) and the time between the diagnosis of the last episode of tuberculosis and the lung function test. The coefficients allow us to calculate the loss due to specific numbers of episodes and time elapsed. For example, the loss of FEV1 in subjects with one episode of tuberculosis and a time lapse of six months is [0.729 + (–1.055)] × 1000 = –326 ml, with a time lapse of 12 months it is [0.729 + (–0.975)] × 1000 = –247 ml, with 18 months it is [0.729 + (–0.868)] × 1000 = –139 ml, and with 24 months it is [0.729 + (–0.865)] × 1000 = –136 ml. For subjects with three and more episodes the corresponding losses are –583 ml, –503 ml, –396 ml, and –393 ml. The data show that the loss of lung function is highest in the first six months and stabilises at 13–18 months.
Age and height adjusted regression coefficients β and standard errors (SE) for the number of TB episodes and the time elapsed from last TB episode to lung function test for 26 311 miners who did not have pneumoconiosis, and loss of lung function after one episode and specific lapsed time
Table 5 shows the age and height adjusted regression coefficients and standard errors for the number of episodes of tuberculosis for subjects known to be HIV negative (n = 1038) and for those known to be HIV positive (n = 305). There were no apparent major differences between the two groups.
Age and height adjusted regression coefficients β and standard errors (SE) for the number of TB episodes and 25 055 subjects known to be HIV positive or HIV negative
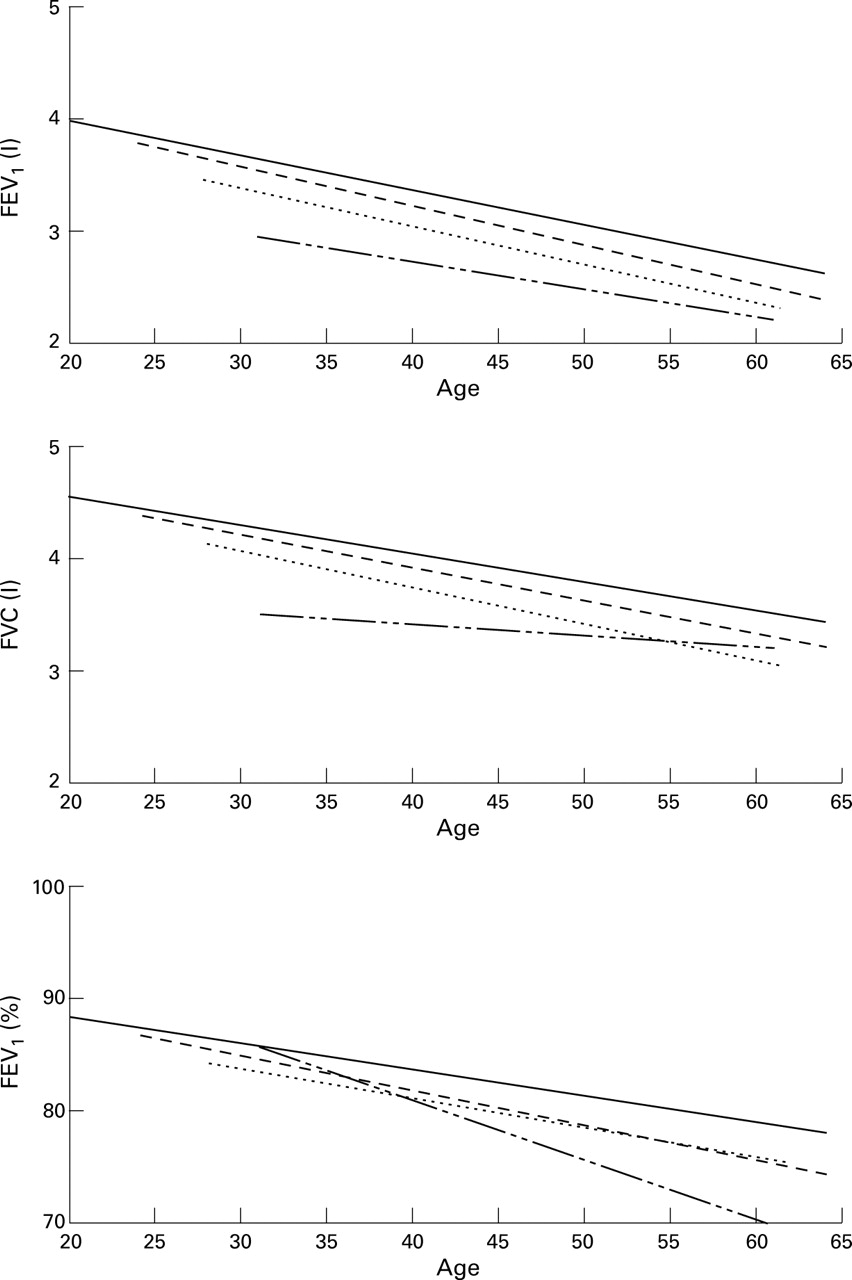
Figure 1 shows the decline in lung function (FVC, FEV1, and FEV1%) with age for subjects without tuberculosis and pneumoconiosis, according to number of tuberculosis episodes, estimated cross sectionally. The plotted curves were estimated individually for each group and indicate that, in addition to the average loss due to the tuberculosis episodes, subjects with tuberculosis also have a steeper decline with age.
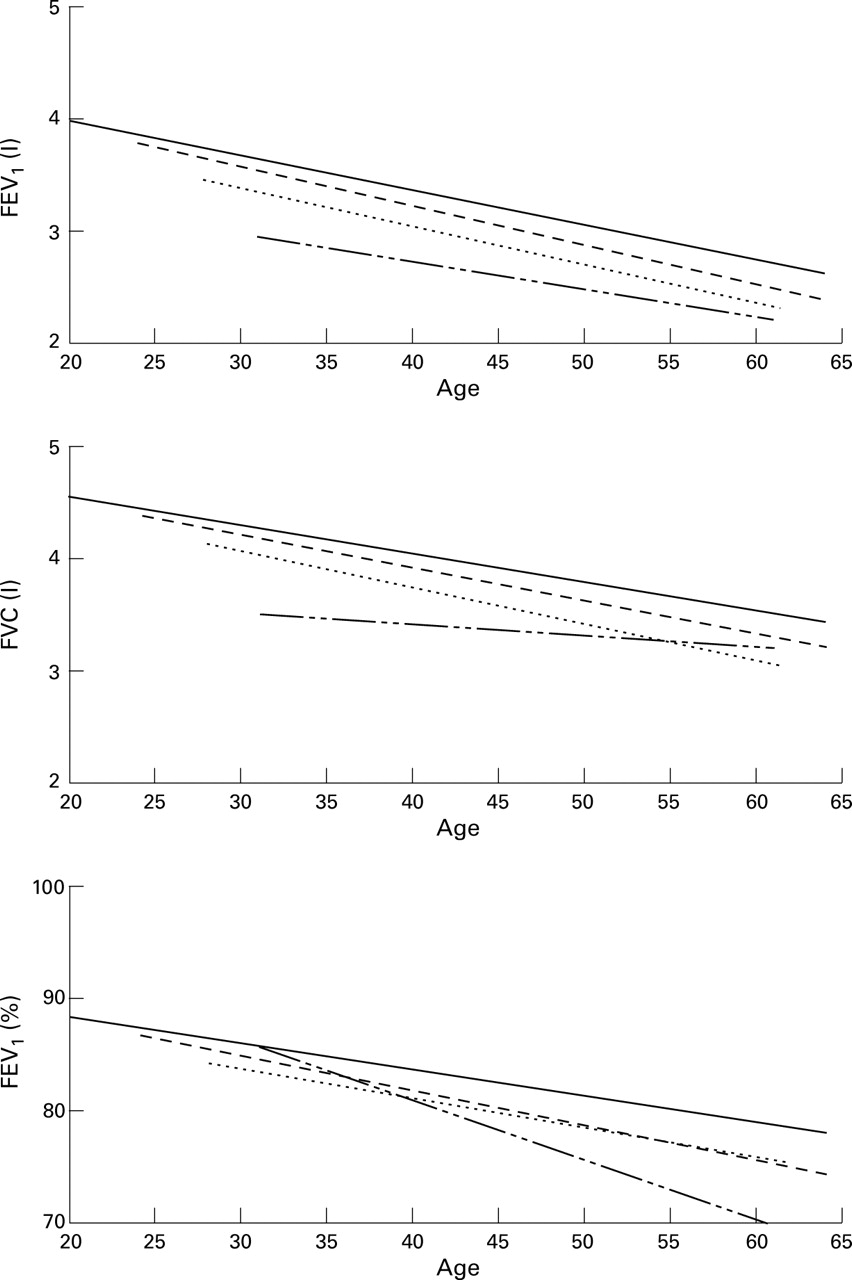
Decline in lung function with age for miners with one (– – – –), two (.....), and three and more (—— - - ——) episodes of tuberculosis.
Figure 2 shows the percentage of subjects whose percentage predicted FEV1 was below 80% for miners without tuberculosis or pneumoconiosis, and for those with one, two, and three or more episodes of tuberculosis. To estimate the chronic loss—that is, the residual deficit in lung function—subjects with a time lapse of less than 18 months were excluded from this calculation.

{kind=link}
{kind=link}
Distribution of percentage predicted forced expiratory volume in one second (FEV1) and percentage of subjects below the 80% predicted value.
Discussion
Several studies have observed that early and partially treated tuberculosis results in airways obstruction.1-5 Only a few studies with a follow up of more than 18 months have been performed. In one study 68% of 71 subjects had evidence of airways obstruction after 9–192 months (average 5.6 years) of follow up from diagnosis of tuberculosis.6 Impairment of airflow was related to the extent of tuberculosis determined radiologically and to the amount of sputum produced at the end of follow up, which also correlated with the extent of the disease.6 In another study obstructive changes were found to be most common after 10 years of follow up and were correlated with the extent of residual shadowing on the chest radiographs.7A third study observed that, after 15 years of follow up, 40 patients with pulmonary tuberculosis who had obstructive impairment on discharge had a higher estimated yearly decline in vital capacity than those without obstruction (–54.3 ml/year versus –27.7 ml/year) but the decline in FEV1 was only slightly higher.8
The residual damage to the lung tissue after completion of tuberculous treatment includes varying degrees of fibrosis, bronchovascular distortion, emphysema, and bronchiectasis.18 Increased sputum production was also observed several years after tuberculosis treatment that correlated with the initial extent of tuberculosis on the radiographs.6 The present study quantifies the loss of lung function caused by initial and recurrent treated tuberculosis and by specific time lapsed after tuberculosis diagnosis, especially the chronic damage due to tuberculosis episodes in a gold mining population screened and treated for tuberculosis according to WHO guidelines.
Because of exposure to silica dust, the South African gold miners are at an increased risk of developing pulmonary tuberculosis and many miners develop several episodes of tuberculosis which are thought to be mainly due to reinfection. As most miners continue to be exposed to silica dust after treatment, it is important to evaluate the impact of recurrent episodes of tuberculosis on loss of lung function in these subjects. The present study evaluated the impact of recurrent episodes of treated tuberculosis on impairment of lung function in 27 660 black South African gold miners of whom 2137 had had one episode of tuberculosis, 366 two episodes, 79 three episodes, and 17 four or more episodes of tuberculosis.
The increased number of episodes of tuberculosis corresponded with increasing loss of lung function. This loss was the highest in the first six months after diagnosis of tuberculosis, and became stable in 13–18 months. The estimated decrease in FEV1 in subjects with one episode of tuberculosis was 326 ml after six months, 247 ml after one year, and stabilised at an average residual loss of 153 ml over the total follow up period (table 4); for subjects with two episodes of tuberculosis the temporal loss of FEV1 was 499 ml after six months, 419 ml after 12 months, and stabilised at an average residual loss of 326 ml from 12 months onwards; while for subjects with three episodes of tuberculosis the temporal loss of FEV1 was 583 ml after six months, 503 ml after 12 months, and stabilised at an average residual loss of 410 ml.
For FVC the estimated decrease in subjects with one episode of tuberculosis was 305 ml after six months, 213 ml after one year, and stabilised at an average residual loss of 96 ml over the total follow up period (table 4); for subjects with two episodes the temporal loss of FVC was 495 ml after six months, 403 ml after 12 months, and stabilised at an average residual loss of 286 ml from 12 months onwards; and for subjects with three episodes of tuberculosis the temporal loss of FVC was 554 ml after six months, 462 ml after 12 months, and stabilised at an average residual loss of 345 ml. However, the loss in FEV1% showed a different pattern, suggesting an increase in the obstructive pattern with increasing duration of the follow up period (table 4), especially in subjects with three or more episodes of tuberculosis. This result is in agreement with the previous studies with longer follow up periods which observed an obstructive pattern in patients with tuberculosis.6 ,7
The presence of HIV infection in many tuberculosis subjects did not bias the estimated effect of tuberculosis on lung function as those who tested HIV positive and HIV negative at the time of the diagnosis of tuberculosis had a similar loss of lung function (table 5). In recent years almost all subjects presenting with tuberculosis are tested for HIV infection. The effect of pneumoconiosis on loss of lung function was similar to that of one episode of tuberculosis.
To determine the percentage of subjects with chronic lung function impairment we calculated the percentage of subjects whose predicted FEV1 was below 80%—namely, 18.4% in those with one episode of tuberculosis, 27.1% in those with two episodes of tuberculosis, and 35.2% in those with three or more episodes of tuberculosis (fig 2). This result shows that miners with a history of pulmonary tuberculosis need to be carefully monitored for chronic impairment of lung function and that prevention of further episodes of tuberculosis in these miners is of great importance.
Limitations of the study include the lack of adjustment for smoking and exposure to silica dust and the retrospective assessment of tuberculosis history. Tobacco smoking could potentially have biased the estimated effect of tuberculosis on loss of lung function as tobacco smoking was found to be associated with an increased risk of tuberculosis in a cohort of white gold miners,10 and smoking is known to increase lung function loss. However, the bias is unlikely to be of substantial importance as black gold miners generally have substantially lower tobacco consumption (5–10 cigarettes per day) than that of the cohort of white miners (20–50 cigarettes per day).19 In the absence of data on exposure to silica dust, silicosis has been shown to act as a surrogate variable for the effect of exposure to silica dust on loss of lung function in miners with a relatively low rate of pulmonary tuberculosis,20 but it is possible that the extent of lung damage due to tuberculosis is potentiated by the silica dust load in the lung. Because of retrospective assessment of tuberculosis, healthy survival effect could have resulted in the underestimation of the effect of tuberculosis on lung function. There is some indication of the presence of this effect in fig 1. Younger subjects with three episodes of tuberculosis have FVC almost as low as that of older subjects, suggesting that the older subjects could be those with three less damaging episodes of tuberculosis and that older miners with extensive loss of lung function due to three or more episodes of tuberculosis had left the mines.
In conclusion, tuberculosis can cause chronic lung function impairment which increases incrementally with the number of episodes of tuberculosis, affecting approximately 18% of subjects with one episode, 27% of subjects with two episodes, and 35% of subjects with three episodes of tuberculosis. Clearly, prevention of chronic lung function impairment caused by tuberculosis in gold miners would be accomplished by preventing tuberculosis through intervention on risk factors such as HIV, silica dust exposure, silicosis, and socioeconomic factors, and by detection of the tuberculosis episodes at an early stage.
Acknowledgments
The authors thank the Anglogold Health Services, which covers the workforce of Freegold mines in Welkom in South Africa, for allowing them to use their lung function, pulmonary tuberculosis and radiological data and acknowledge valuable comments from Dr Jill Murray and Professor A Solomon. The study received funding from the Safety in Mines Research Advisory Committee.