Article Text

Abstract
BACKGROUND The long acting β2 agonist salmeterol is very effective in preventing asthmatic responses to specific stimuli, and this effect could theoretically be due to some anti-inflammatory property in addition to bronchodilator property.
METHODS The protective effect of a single dose of salmeterol (50 μg) on allergen induced early and late responses and on the associated airway inflammation was investigated in a double blind, placebo controlled, crossover study in 11 atopic asthmatic subjects. Eosinophil percentages and concentrations of eosinophil cationic protein (ECP) in peripheral blood and in hypertonic saline induced sputum were measured 24 hours after allergen inhalation.
RESULTS Salmeterol effectively inhibited both early and late asthmatic responses in comparison with placebo. Salmeterol also inhibited the increase in the percentage of eosinophils in the sputum 24 hours after allergen inhalation (median (range) baseline 6% (1–36), after placebo 31% (5–75), after salmeterol 12% (1–63)). However, the increase in both sputum and serum ECP concentrations 24 hours after allergen challenge was not affected by pretreatment with salmeterol.
CONCLUSIONS A single dose of salmeterol inhibits the allergen induced airway responses and the increase in sputum eosinophils after allergen challenge.
- β agonist
- salmeterol
- asthma
- allergen bronchial challenge
- eosinophils
Statistics from Altmetric.com
It is known that long acting β2 agonists are effective in controlling asthma symptoms and improving lung function.1 Additionally, long acting β2agonists have shown some in vitro anti-inflammatory properties but it is controversial whether they have similar effects in vivo. There is indirect evidence that long acting β2 agonists inhibit the late asthmatic reaction (LAR) following inhaled allergen challenge and the associated increase in bronchial hyperresponsiveness.2 Moreover, pretreatment with salmeterol before allergen challenge induced a significant decrease in the concentration of eosinophil cationic protein (ECP) but not of the differential cell count in bronchoalveolar lavage (BAL) fluid obtained 24 hours after allergen inhalation.3 By analysis of sputum induced by inhalation of hypertonic saline, some investigators reported no effect of a single dose of salmeterol on the increase in eosinophil percentages induced by allergen inhalation in sensitised asthmatics.4 In this study we examined whether a single dose of salmeterol is able to reduce the increase in the number of sputum eosinophils induced by allergen challenge in sensitised asthmatic subjects.
Methods
Eleven mild asthmatic subjects (eight men) of mean age 20 years (range 16–27) with positive skin prick tests toDermatophagoides pteronyssinus were selected. All subjects showed normal baseline forced expiratory volume in one second (FEV1) (mean 93% predicted (range 83–121)), non-specific bronchial hyperresponsiveness to methacholine (geometric mean 0.134 mg (range 0.037–0.59)), and an early asthmatic response (EAR) followed by an LAR to specific bronchial challenge withD pteronyssinus in a screening test. All patients were treated with occasional inhaled salbutamol on demand only during the preceding month and had no respiratory infections. Each subject performed two allergen inhalation tests at four week intervals 15 minutes after two puffs of salmeterol (50 μg) or placebo, administered in double blind, randomised, crossover design. At seven hours a methacholine challenge test was performed (results not presented). At 24 hours after allergen inhalation, hypertonic saline induced sputum and blood samples were collected for measurement of total and differential cells and ECP concentration. In each allergen challenge the same total dose of allergen administered in the screening test was inhaled step by step.
Specific bronchial provocative tests were performed with allergens standardised in biological units (BU) (NeoAbellò, Milano, Italy). Allergen extract solution was delivered by a DeVilbiss 646 jet nebuliser (DeVilbiss Health Care, Somerset, Pennsylvania, USA) using a procedure previously described.5 EAR and LAR were measured as percentage falls in FEV1 with respect to baseline 10–60 minutes and 3–7 hours, respectively, after allergen inhalation. EAR and LAR were considered significant when the percentage falls in FEV1 were greater than 20%.
Sputum was induced and processed according to the method of Pinet al,6 slightly modified.7 ECP concentrations were measured in blood and sputum supernatant using a specific radioimmunological method (ECP RIA, Pharmacia, Uppsala, Sweden).8
ANOVA and paired t tests were used to compare FEV1, PD20FEV1, and serum or sputum ECP concentrations, while the Mann-Whitney test was used to compare sputum and blood differential cell percentages. A level of probability lower than 5% was considered significant.9
Results
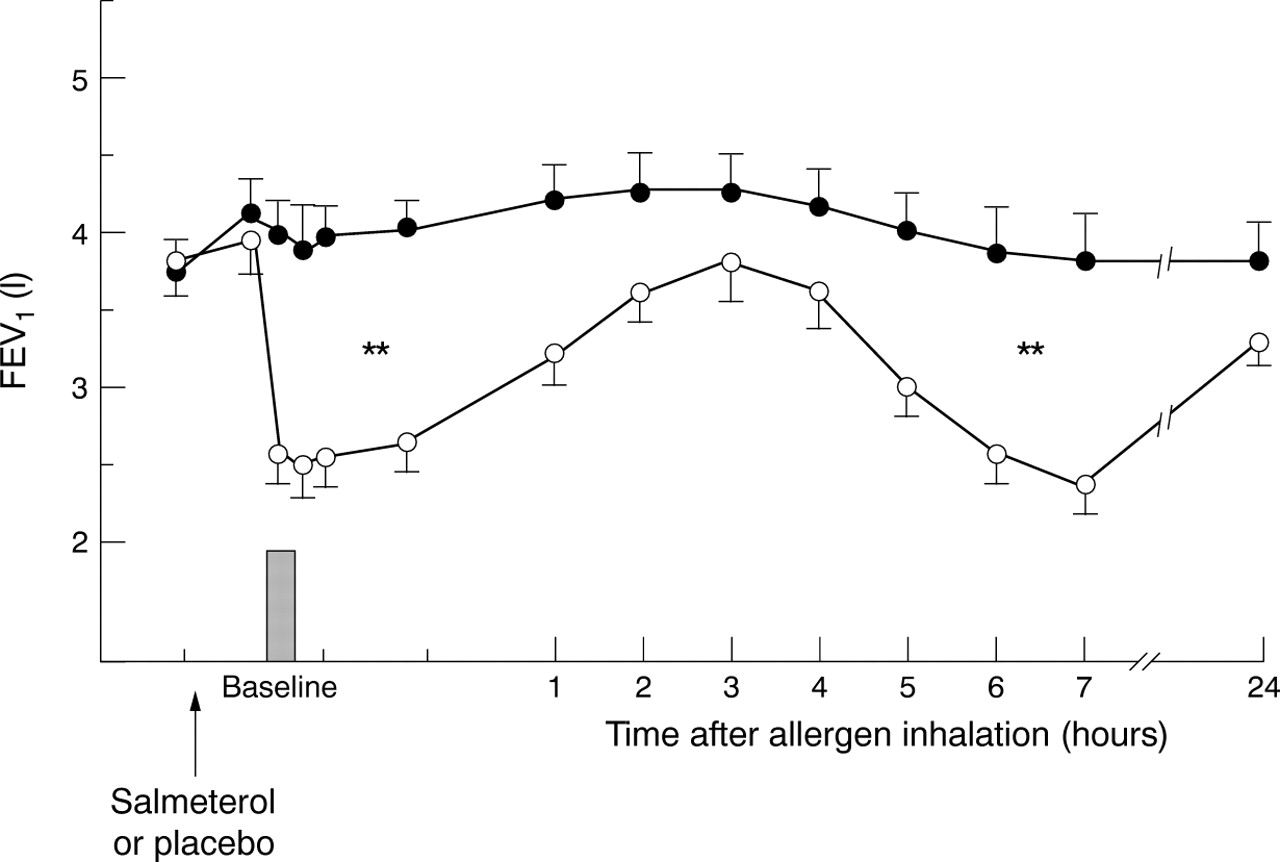
Pretreatment with salmeterol produced a significant increase in FEV1 compared with placebo (mean (SD) ΔFEV110 (5)% after salmeterol, 4 (5)% after placebo, p<0.05) and an inhibition of both EAR (median (range) ΔFEV1 –2% (–28 to +2) after salmeterol, –41% (–57 to –27) after placebo, p<0.01) and LAR (median (range) ΔFEV1 –5% (–37 to +6) after salmeterol, –45% (–65 to –20) after placebo, p<0.01; fig 1). After pretreatment with salmeterol EAR persisted in one subject and LAR in three.
{kind=link}
Mean (SE) values of FEV1 before and up to seven hours after allergen challenge in subjects pretreated with placebo (open circles) or salmeterol (closed circles). **p<0.01 between placebo and salmeterol.
Sputum was successfully obtained in all subjects at baseline evaluation and 24 hours after both allergen challenges. When placebo was inhaled before allergen challenge the sputum eosinophil percentage increased significantly (median 34%, p<0.05 versus baseline). Compared with placebo, pretreatment with 50 μg salmeterol resulted in a significant inhibition of the increase in sputum eosinophil percentage at 24 hours after allergen (15%, p<0.05 with respect to placebo; table 1).
Inflammatory indices of eosinophil activation in sputum and blood
Sputum ECP concentrations also increased at 24 hours after allergen inhalation in subjects pretreated with placebo (geometric mean 581 μg/ml, p<0.01 versus baseline) as well as after pretreatment with salmeterol (410 μg/ml, p<0.01 versus baseline) with no significant difference between placebo and salmeterol treatment (table1).
Blood eosinophil percentages did not change with respect to the baseline value at 24 hours after allergen inhalation with either placebo or salmeterol. Compared with baseline values, serum ECP concentrations increased at 24 hours after allergen with placebo pretreatment (9.2 versus 6.0 μg/l, respectively, p = 0.03) and salmeterol pretreatment (9.4 versus 6.0 μg/l, respectively, p = 0.02; table 1).
Discussion
This study shows that salmeterol inhibits the increase in sputum eosinophils induced by allergen challenge in sensitised asthmatic subjects. Moreover, our data confirm that pretreatment with salmeterol prevents both EAR and LAR to allergen inhalation.
Eosinophil recruitment into the airway can be prevented by anti-inflammatory drugs such as inhaled corticosteroids.10It is debatable whether long acting β2 agonists also have some anti-inflammatory properties in vivo. In a group of subjects with mild asthma salmeterol significantly reduced serum ECP levels by approximately 50%.11 Moreover, salmeterol significantly reduced the increase in plasma proteins in nasal lavage fluid of subjects with allergic rhinitis eight hours after nasal allergen challenge12 and inhibited the recruitment of eosinophils in bronchial lavage fluid 24–48 hours after segmental allergen challenge.13 Pizzichini et al found that the late increase in sputum eosinophils after allergen inhalation was not prevented by pretreatment with salmeterol or with beclomethasone.4 The disagreement between our results and the results of Pizzichini et almay be explained by the different study design. In the study by Pizzichini et al each subject repeated five allergen challenges and four hypertonic saline sputum inductions for each allergen challenge. This could have resulted in a progressive increase in airway inflammation in each subject during the progression of the study, leading to a more persistent eosinophilic inflammation and consequently to the low repeatability reported by these authors in sputum eosinophil percentages measured before each allergen challenge. In fact, a small change in markers of airway inflammation can be induced by repeated hypertonic saline challenges14 and allergen inhalation increases non-specific bronchial reactivity for many days.15
Although airway eosinophilic recruitment induced by allergen challenge was inhibited by salmeterol, ECP levels in induced sputum obtained after pretreatment with salmeterol were no different from those obtained after placebo pretreatment. While it has been shown that salmeterol can inhibit diapedesis of inflammatory cells into the tissue at bronchodilator doses,16 higher concentrations of drug are required to affect ECP release from eosinophils.17 On the other hand, ECP levels were more variable than eosinophil percentages and there is therefore considerable potential for a type II error in failing to detect a modest effect of salmeterol on ECP levels.
Tolerance to some anti-inflammatory effects of salmeterol has been reported as a possible explanation for the loss of the protective effect of salmeterol on allergen challenge after repeated administrations of the drug.18 This fact could produce a discrepancy between the acute and chronic effects of salmeterol on airway inflammation in asthma.
In conclusion, we have shown that a single dose of salmeterol reduces the recruitment of eosinophils in the airways after allergen challenge, in addition to the prevention of the early and late airway responses.
Acknowledgments
Source of study drugs: GlaxoWellcome, Verona, Italy.