Article Text

Abstract
BACKGROUND Pulmonary hypoplasia accompanied by pulmonary hypertension resistant to treatment is an important feature of congenital diaphragmatic hernia (CDH). The pathogenesis of the pulmonary vascular abnormalities in CDH remains to be elucidated at the molecular level. Vascular endothelial growth factor (VEGF), an endothelial cell specific mitogen, is known to play a role in pulmonary angiogenesis and vascular remodelling but there are no data on VEGF expression in patients with CDH.
METHODS Necroscopic lung specimens from 21 patients with CDH with lung hypoplasia and from seven age matched control newborn infants without lung hypoplasia were processed for immunohistochemical analysis using affinity purified anti-human VEGF antibodies. All the cases of CDH had pulmonary hypoplasia, indicated by a lung/body weight index of ⩽0.012, and pulmonary hypertension indicated by repeated cardiac ultrasonography. Cellular localisation of VEGF was semiquantitatively analysed using a staining score ranging from 0 (no staining) to 4 (very strong staining).
RESULTS Significantly raised levels of VEGF immunoreactivity were observed in lung specimens from cases of CDH compared with controls. VEGF was detected mainly in the bronchial epithelium and the medial smooth muscle cells of large (>200 μm) and small (<200 μm) pulmonary arteries, the most intense staining being in the medial smooth muscle cells of the small pulmonary arteries. Endothelial cells were positive for VEGF staining in patients with CDH but not in controls.
CONCLUSIONS This is the first study of VEGF expression in newborn infants with CDH. Increased levels of VEGF, especially in the small, pressure regulating pulmonary arteries, point to a potential role in vascular remodelling. This may reflect an unsuccessful attempt by the developing fetus to increase the pulmonary vascular bed in the hypoplastic lungs to alleviate the associated pulmonary hypertension.
- congenital diaphragmatic hernia
- pulmonary hypertension
- vascular endothelial growth factor
- angiogenesis
- immunohistochemistry
Statistics from Altmetric.com
- congenital diaphragmatic hernia
- pulmonary hypertension
- vascular endothelial growth factor
- angiogenesis
- immunohistochemistry
Congenital diaphragmatic hernia (CDH) remains one of the major challenges in paediatric surgery and neonatology. Despite recent developments in therapeutic modalities such as delayed surgery, exogenous surfactant therapy, nitric oxide (NO) inhalation, extracorporeal membrane oxygenation (ECMO), and partial liquid ventilation, the mortality rate remains around 40% in high risk cases.1-3 The main pathological findings reported in the lungs of infants with CDH are lung hypoplasia and pulmonary vascular abnormalities including (a) reduced total pulmonary vascular bed and decreased number of vessels per volume unit of lung and (b) medial hyperplasia of pulmonary arteries together with peripheral extension of the muscle layer into small arterioles.4-6 The most common cause of the unfavourable outcome in human CDH is persistent pulmonary hypertension.2-5 Indeed, follow up of surviving patients with CDH has revealed that the pulmonary perfusion scan does not improve although the ventilation scan improves towards nearly normal levels.7
A recent developmental study of the lung vasculature showed that in early gestation the pulmonary vasculature develops by a combination of central angiogenic sprouting and the formation of peripheral vasculogenic lakes which progressively communicate with each other as gestation advances.8 A number of growth factors with a proven or potential role in vascular development and remodelling in health and disease conditions have been identified.9 ,10Vascular endothelial growth factor (VEGF), a potent angiogenic growth factor, has been reported to have a narrow target cell specificity to endothelial cells. Moreover, VEGF regulates vasculogenesis and postnatal vascular remodelling.11-13 VEGF binds to high affinity cell surface receptors, KDR/flk and flt, which are predominantly expressed in endothelial cells.13 Expression of VEGF is upregulated under a variety of pathophysiological conditions including pulmonary hypoxia.12-14
In order to investigate the pathogenesis of the underlying vascular abnormalities in CDH lungs we have investigated the cellular localisation of VEGF in pulmonary necropsy specimens obtained from neonates with CDH and age matched controls.
Methods
TISSUE SPECIMENS
Lung tissue specimens used in this study were obtained from our archival collection at the Department of Pathology. These specimens represent material from 21 patients with CDH treated at Sophia Children’s Hospital during the period 1981–97 who had died and from whom necroscopic material was obtained with the parents’ consent. All cases were associated with lung hypoplasia, as indicated by a lung/body weight ratio index of ⩽0.012.15 The control group consisted of seven age matched neonates who had died in the first 24 hours of extrauterine life because of neonatal asphyxia or placental insufficiency. These control cases did not have lung hypoplasia on histological screening. The CDH group had a gestational age varying from 35 weeks to term, with a mean of 38.4 weeks, while that of the control group was 35.1 weeks. Neither the CDH nor the control group was subjected to ECMO treatment. The left or right lung was chosen randomly for examination since no significant differences were found between the two lungs on histological screening in subjects with CDH.
Lung tissue specimens were fixed in formalin by immersion fixation and embedded in paraffin for histopathological examination and immunohistochemical analysis.
IMMUNOHISTOCHEMICAL ANALYSIS
Paraffin sections (6 μm thickness) of the lung tissues were cut and mounted on glass slides coated with 3-amino-propyl-trioxysilane (Sigma, St Louis, MO, USA). Immunohistochemical analysis was performed using a standard avidin-biotin complex (ABC) method as described previously.16 ,17 In brief, after deparaffinisation in xylene and rehydration through graded alcohol, the slides were rinsed with water and phosphate buffered saline (PBS) and placed in a Sequeza Immunostaining Workstation (Shandon Scientific Ltd, Astmoor, Runcorn, UK). The slides were preincubated for 15 minutes with normal goat serum to block non-specific binding, then incubated for 30 minutes at room temperature with affinity purified rabbit polyclonal antibodies in a dilution of 1:200. The anti-VEGF antiserum used was raised against a 20 amino acid synthetic peptide corresponding to residues 1–20 of the amino terminus of human VEGF18 (Santa Cruz Biotechnology Inc, Santa Cruz, USA).
The optimal dilution was identified by examining the intensity of staining obtained with a series of dilutions of the antiserum from 1:50 to 1:500. The dilution (1:200) resulted in specific and easily visible signals in paraffin sections of a capillary haemangioma. The haemangioma sections served as a positive control in the study. After washing with PBS, the test and control slides were incubated for 30 minutes with biotinylated secondary antibody (Multilink, 1:75 dilution, Biogenex, San Ramon, MO, USA). After two washes in PBS the slides were incubated for 30 minutes with alkaline phosphatase conjugated streptavidin (Biogenex) in a dilution of 1:50, then rinsed with 0.2 M Tris HCl, pH 8.0. Levamisole (Sigma) was used to block the endogenous alkaline phosphatase activity and the slides were stained for 30 minutes with 0.3% new fuchsin/Tris HCl (Sigma) for colour enhancement. Negative controls were prepared by omission of the primary antiserum. The slides were lightly counterstained with Mayer’s haematoxylin for 10 seconds.
Immunolocalisation of VEGF in endothelial cells and smooth muscle cells was verified by staining with specific markers. Endothelial cells were identified by CD31 immunostaining.19 Staining was performed by the ABC method using 0.025% 3,3-diaminobenzidine (DAB) as chromogen. The slides were incubated for 20 minutes in methanol with 0.3% H2O2 to block the endogenous peroxidase activity. They were then incubated with the primary anti-human CD31 monoclonal antibody in a dilution of 1:80 (Dako Corporation, Glostrup, Denmark) at room temperature for 30 minutes and subsequently visualised after developing the colour with 0.025% DAB. Using the DAB based colour development method, consecutive tissue sections were stained with anti-human mouse monoclonal α-smooth muscle actin (αSMA) antibody (clone 1A4, Biogenex) in a dilution of 1:200.
SEMIQUANTITATIVE ANALYSIS
Prior to screening, sections were coded so that the observers were unaware of the clinical details of the case under study. VEGF expression was analysed semiquantitatively using a visual scale ranging from 0 to 4 (grade 0 = no staining, grade 1 = focal staining, grade 2 = diffuse faint staining, grade 3 = diffuse moderate staining, and grade 4 = diffuse strong staining).20 The entire slide of a tissue block taken from the mid lung area was investigated and scored at the same magnification by three independent observers and the average used for subsequent analysis. Sections were graded 0–4 for the localisation of VEGF in the bronchial epithelium, endothelium, and medial smooth muscle cells in small (50–200 μm external diameter) and large (>200 μm external diameter) pulmonary arteries.21 This scoring method has previously been shown to allow the detection of differences in expression levels as small as 1.5 times.20 ,22
STATISTICAL ANALYSIS
The median VEGF staining score was calculated for the two groups. Before ranking, the scores were rounded to the nearest complete number. Statistical analysis was performed after ranking using either the Mann–Whitney test or Fisher’s exact test as appropriate. A p value of ⩽0.05 was considered significant.
Results
CLINICAL AND NECROPSY DATA
Thirteen of the 21 diaphragmatic hernias were left sided. All patients presented in the first six hours of life and were treated according to a standard protocol including conventional mechanical ventilation, cardiac ultrasound, and delayed surgery.1Clinical evidence of right to left shunting was obtained by preductal and postductal transcutaneous oxygen saturation differences of >10% in cases of CDH.23 Echocardiography documented the right to left shunt and pulmonary hypertension. In three cases associated major congenital anomalies were found (Fallot’s tetralogy, tracheo-oesophageal cleft, and trisomy 21, respectively). Nineteen of the neonates with CDH died within 48 hours of birth, five in the first hour. In three instances hyaline membrane disease was observed and one patient developed pulmonary bleeding. All seven age matched controls had died in the first 24 hours after birth. Control cases were subjected to ventilatory therapy in settings similar to those of the CDH cases, including inspiratory oxygen fraction of 1.0 for variable periods up to 16 hours postnatally.
LOCALISATION OF VEGF
VEGF was found in the bronchial epithelium and medial arterial smooth muscle cells of the control cases. Distinct VEGF immunostaining was identified in the bronchial epithelium and the medial smooth muscle cells of the pulmonary arteries in tissue specimens from the CDH group, as verified by immunolocalisaton of αSMA. VEGF immunoreactivity in the bronchial epithelium and arterial medial smooth muscle cells was more intense in the CDH cases than in the controls (fig 1A and B).
{kind=link}
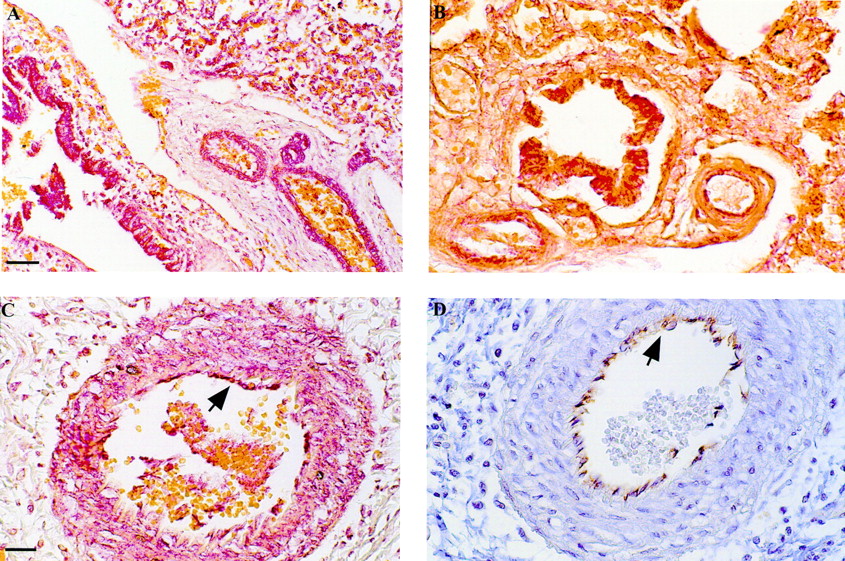
Immunohistochemical localisation of VEGF in lung tissue. (A) Intense expression of VEGF in the medial smooth muscle cells of small diameter pulmonary arteries and in the bronchial epithelium of CDH lung tissue. (B) Expression of VEGF in the bronchial epithelium and faintly in the smooth muscle cells of the pulmonary arteries of control non-hypoplastic lung tissue. (C) Expression of VEGF in the arterial endothelium (arrowed) and medial smooth muscle cells of pulmonary arteries in CDH hypoplastic lung tissue. (D) Arterial endothelium identified (arrow) by CD31 staining using peroxidase technique. (Calibration bars = 50 μm in A and B and 25 μm in C and D).
In the CDH group VEGF staining in the pulmonary vasculature was most intense in the medial smooth muscle cells of the small pulmonary arteries with an external diameter of <200 μm. High levels of VEGF expression were also found in the supernumerary arteries from the CDH cases. VEGF expression was detected in the endothelium of the pulmonary arteries only in the CDH cases (fig 1C). This endothelial staining was colocalised using consecutive sections stained with the endothelial cell marker CD31 (fig 1D). No VEGF immunopositivity was detected in the endothelium of controls (fig 1B). Weak VEGF expression was observed in the medial smooth muscle cells of large pulmonary veins in the CDH cases.
No differences in the pattern of VEGF expression were seen between the CDH cases artificially ventilated for up to 48 hours and the five cases who died in the first hour after birth despite maximal attempted resuscitation, even without receiving vigorous ventilatory support. No VEGF expression was observed in the arterial medial smooth muscle cells of pulmonary veins in the control group.
The mean VEGF expression score in the CDH cases had a maximal value of 3.38 in the bronchial epithelial cells. Endothelial and medial smooth muscle cells of large pulmonary arteries (external diameter >200 μm) had low staining values of 0.5 and 1.43, respectively. Statistical analysis of the VEGF expression scores in the two groups showed significantly higher levels (p⩽0.05) in the bronchial epithelium and medial smooth muscle cells of the large and small pulmonary arteries of the CDH group compared with controls (p = 0.001, 0.027, and 0.002, respectively, using the non-parametric Mann-Whitney U test, table 1).
Table of ranking data for Mann-Whitney U test
Since there was no expression of VEGF in the endothelium of the pulmonary arteries in the controls and the score was always zero, Fisher’s exact test was considered more appropriate for the comparison of endothelial staining scores.24 ,25 Significantly higher expression was observed in the endothelial cells of CDH cases using Fisher’s exact test with p values of 0.01 and <0.001 for large and small pulmonary arteries, respectively, compared with controls.
Discussion
We have found increased VEGF immunoreactivity in the endothelium and medial smooth muscle cells of pulmonary arteries in cases of CDH with pulmonary hypoplasia. The highest levels of expression in the pulmonary vasculature were observed in the medial smooth muscle cells of arteries with a diameter of less than 200 μm, particularly in the supernumerary arteries which are known to play an important role in pulmonary blood pressure regulation and vascular resistance.26
Our results are in agreement with a previous experimental report which confirmed that the arterial medial smooth muscle cells are a source of VEGF.27 The increased VEGF expression detected in CDH cannot be due to artificial ventilation since we did not find any difference in VEGF expression between the patients ventilated for short (up to one hour) or longer (up to 48 hours) periods. In addition, no differences in the degree of VEGF expression were found in bronchial epithelium in the CDH group, regardless of whether or not these lungs were exposed to high levels of inspiratory oxygen or volume trauma and shear forces related to variable periods of artificial ventilation.
Since no significant differences in lung hypoplasia have been reported between the right and left lungs from infants with high risk CDH,28 ,29 we randomly chose either lung from the CDH group for study. In agreement with previous studies, we found no differences between the lungs in a preliminary examination.
VEGF is recognised as an endothelial cell mitogen and angiogenic inducer with activity restricted to the vascular endothelial cells.30 ,31 It is expressed in a variety of cells and a paracrine mechanism of action has been suggested whereby non-endothelial cells secrete VEGF which modulates the vasculogenesis and angiogenesis in the adjacent vascular endothelium.27This important angiogenic role of VEGF is indicated by the fact that abnormal vessel development leading to death occurred in embryos lacking a single VEGF allele32 or following the experimental inactivation of the VEGF gene by replacing the coding sequence of exon 3 of the VEGF gene in embryonic stem cells.33
We found endothelial reactivity for VEGF in the pulmonary vasculature of human CDH hypoplastic lungs but not in the control cases; this is in agreement with a previous study which reported that VEGF is not expressed in the normal endothelium of the developing fetus.27 However, it has previously been reported that, in endothelial cells derived from microvessels, VEGF expression can be upregulated in vitro by hypoxia and adenosine.34 ,35
There is a similarity between the structural changes in the pulmonary vasculature of CDH hypoplastic lungs and that of another paediatric form of pulmonary hypertension—namely, persistent pulmonary hypertension of neonates.9 ,36 It is unclear whether similar growth factors and cytokines contribute to these vascular abnormalities.37 Furthermore, it is of note that increased VEGF expression has been reported in the lungs of patients with primary pulmonary hypertension.37
Our knowledge of vascular development in congenital diaphragmatic hernia and/or vascular remodelling following postnatal interventions is far from complete, and it is too early to speculate in detail about the pulmonary vascular abnormalities at the molecular level. There is no doubt that growth factors play an essential role in the development and maturation of the pulmonary and vascular systems.38 ,39The increased VEGF expression in small diameter and supernumerary pulmonary arteries in CDH cases complicated by pulmonary hypertension may reflect an apparently unsuccessful attempt by the developing fetus and neonate to compensate for the stunted lung vessel growth and/or to stimulate arterial angiogenesis of the pulmonary pressure regulating arteries caused by a mechanism which remains to be identified.
Acknowledgments
The expert technical assistance of Mr Johan van Lier is much appreciated. The Sophia Foundation and Medical Faculty, EUR supported this study. Dr Shehata is in receipt of an international grant from the Tanta University Medical Faculty Foundation, Tanta, Egypt.