Article Text

Abstract
BACKGROUND Idiopathic pulmonary fibrosis is an inflammatory disease which leads to chronic ventilatory insufficiency and is characterised by a reduction in pulmonary static and dynamic volumes. It has been suggested that lung elastance may also be abnormally increased, particularly in end stage disease, but this has not been systematically tested. The aim of this study was to assess the respiratory mechanics during mechanical ventilation in patients affected by end stage disease.
METHODS Respiratory mechanics were monitored in seven patients with idiopathic pulmonary fibrosis being ventilated for acute respiratory failure (Pao 2/Fio 2 5.8 (0.3); pH 7.28 (0.02); Paco 2 8.44 (0.82) kPa; tidal volume 3.4 (0.2) ml/kg; respiratory rate 35.1 (8.8) breaths/min) using an oesophageal balloon and airway occlusion during constant flow inflation. The total respiratory system mechanics (rs) was partitioned into lung (L) and chest wall (w) mechanics to measure static intrinsic positive end expiratory pressure (PEEPi), static (Est) and dynamic (Edyn) elastances, total respiratory resistance (Rrs), interrupter respiratory resistance (Rint,rs), and additional respiratory resistance (ΔRrs).
RESULTS PEEPi was negligible in all patients. Edyn,rs and Est,rs were markedly increased (60.9 (7.3) and 51.9 (8.0) cm H2O/l, respectively), and this was due to abnormal lung elastance (dynamic 53.9 (8.0) cm H2O/l, static 46.1 (8.1) cm H2O/l) while chest wall elastance was only slightly increased. Rrs and Rint,rs were also increased above the normal range (16.7 (4.5) and 13.7 (3.5) cm H2O/l/s, respectively). RL and Rint,L contributed 88% and 89%, on average, to the total. Edyn,rs, Est,rs, Rrs and Rint,rs were significantly correlated with the degree of hypercapnia (r = 0.64 (p<0.01),r = 0.54 (p<0.05),r = 0.84 (p<0.001), andr = 0.72 (p<0.001), respectively).
CONCLUSIONS The elastances and resistances of the respiratory system are significantly altered in ventilated patients with end stage idiopathic pulmonary fibrosis. These features are almost totally due to abnormalities in lung mechanics. These profound alterations in elastic and resistive mechanical properties at this stage of the disease may be responsible for the onset of hypercapnia.
- idiopathic pulmonary fibrosis
- mechanical ventilation
- pulmonary mechanics
Statistics from Altmetric.com
Idiopathic pulmonary fibrosis is a progressive and generally fatal disease. The essential histological feature is chronic inflammation of the alveolar wall which tends to destroy the lung architecture by consequent healing with progressively severe fibrosis. Alterations of static and dynamic lung volumes due to this disease are well known but little information exists about the mechanical characteristics.1 Studies on static and dynamic lung compliance performed in stable patients revealed that the lung is less distensible than normal,2-5 and it has been suggested that measurements of distensibility may correlate with degree of fibrosis2 ,5 even though studies performed in the late stage of the disease are lacking. As the disease progresses to the end stage, hypoxic respiratory failure ensues and mechanical ventilation is sometimes administered, especially in patients awaiting lung transplantation.6 The institution of mechanical ventilation allows us to record respiratory mechanics non-invasively. These have been shown to be useful both clinically to predict weaning from mechanical ventilation7 ,8 and physiologically to understand the mechanisms leading to life threatening episodes of acute respiratory failure.9-13 This study reports the first systematic measurement of resistances and elastances of the total respiratory system, lung, and chest wall during mechanical ventilation in patients with end stage idiopathic pulmonary fibrosis.
Methods
Seven mechanically ventilated patients with idiopathic pulmonary fibrosis, admitted to our Respiratory Intensive Care Unit for acute respiratory failure while on the waiting list for single lung transplantation, were studied. The study protocol was approved by the Salvatore Maugeri Institutional ethical committee and informed consent was obtained from the patients or from their next of kin.
PATIENTS
The clinical characteristics of the study population are shown in table 1. Pulmonary function tests presented in the table were the last performed in our department (1–5 months before the study). The clinical diagnosis of idiopathic pulmonary fibrosis was confirmed by transbronchial biopsy or after explorative thoracotomy, the diagnostic strategy used in most published studies.1All the patients had undergone one of these two procedures to be included on the North Italian transplant waiting list. Computed tomographic (CT) scans showed interstitial reticular or linear opacities, patchy areas of ground glass appearance, and varying degrees of honeycomb changes. The patients were on long term oxygen therapy and were being treated with systemic corticosteroids or immunosuppressant drugs. Patients who had chest radiographic evidence of pneumonia, clinical or echocardiographic signs of heart failure, or pulmonary embolisms were excluded from the study. The decision to intubate was made by the attending physician on the basis of marked deterioration in blood gas tensions with hypercapnia (pH⩽7.30 with Paco 2 ⩾6.6 kPa) and the presence of severe dyspnoea and tachypnoea. All the patients were intubated with an endotracheal tube (7.0 or 7.5 mm internal diameter) and were mechanically ventilated with a Cesar ventilator (Taema, France) using constant inspiratory flow. The study of respiratory mechanics was started within 24 hours of the intubation.
Pulmonary function tests, arterial blood gas tensions and breathing pattern
MATERIALS
The breathing pattern during spontaneous breathing, just before intubation, was measured using a portable Wright spirometer. Flow was measured with a heated pneumotachograph (Screenmate Jaeger, Wurzburg, Germany) inserted between the proximal end of the endotracheal tube and the “Y” of the ventilator. Volume was determined by numerical integration of the flow signal. Differential pressure transducers (Honeywell, Freeport, Illinois, USA, ±250 cm H2O) were employed to record the pressures. Pressure at the airways (Paw) was sampled by means of tubing proximal to the pneumotachograph. Tracheal pressure (Ptr) was recorded with a polyethylene catheter with a few side holes at the distal tip, positioned in the trachea 3–4 cm below the distal end of the endotracheal tube. Oesophageal pressure (Poes) was monitored using a balloon catheter system inserted in the middle third of the oesophagus and filled with 0.8 ml of air. The position of the balloon was checked using the so called “occlusion test” performed at the beginning of the study.14 The transpulmonary pressure (Pl) was obtained by subtracting Poes from Ptr. The equipment dead space, not including the endotracheal tube, was 140 ml. Arterial blood gas tensions were measured with a blood gas analyser (Radiometer, Copenhagen, Denmark).
STUDY PROTOCOL
The patients were sedated with a benzodiazepine and curarised with pancuronium bromide 0.1 mg/kg during the study. They were examined in a semi-recumbent position. Airway suctioning was carefully done three minutes before each measurement. This time interval has been shown to be sufficient to avoid the effects of the transient bronchoconstriction response to suction.15During the study a physician not involved in the procedure was always present to provide care for the patients. The ventilator settings consisted of a fixed tidal volume (8.3 (0.9) ml/kg), a fixed inspiratory flow (0.60 (0.2) l/s), and a respiratory frequency of 12 breaths/min. The tidal volume was set to be between 30% and 40% of the total lung capacity (TLC) recorded in each patient during the previous pulmonary function test. This was likely to allow us to record the respiratory mechanics far away from the “flat” part of the pressure/volume curve3 and very close to that part of the curve in which these patients usually breathe spontaneously (table 1, FRC/TLC 41.7%). The inspired fraction of oxygen (Fio 2) was set to achieve an oxygen saturation (Sao 2) of >90%. All the patients were studied at zero end expiratory pressure (ZEEP).
MEASUREMENTS
The end inspiratory16 and end expiratory occlusion10 method was employed to record respiratory mechanics. Three to five measurements for each method were taken at fixed intervals of five minutes to assess the reproducibility of the measurements. Several regular mechanical breaths were recorded to achieve a steady state after which the respiratory mechanics were measured. Intrinsic end expiratory pressure (PEEPi) was measured by occluding the airway opening for five seconds at the end of tidal expiration and pressing the end expiratory hold button incorporated in the ventilator. During this occlusion the increases in Paw and Ptr, if any, were due to end expiratory elastic recoil of the respiratory system (PEEPi,rs) and the increase in Pl reflected end expiratory elastic recoil of the lung (PEEPi,L). End expiratory elastic recoil of the chest wall (PEEPI,w) was computed by subtracting PEEPi,L from PEEPi,rs. After several breaths the airway opening was occluded at the end of inflation for three seconds. As shown in fig 1, three seconds were usually sufficient to reach an apparent plateau in tracheal pressure. Briefly, after the occlusion there is a sudden decrease in Paw, Ptr, and Pl from a maximal value (Pmax) to a lower value (P1), followed by a gradual decrease until an apparent plateau is reached (P2). P1 was measured by back extrapolation of a computer fitted curve. P2 represents the static end inspiratory elastic recoil of the total respiratory system (Pst,rs), lung (Pst,L), and chest wall (Pst,w) on Paw, Ptr, Pl, and Poes, respectively. The static elastance of the total respiratory system (Est,rs) was calculated as the ratio between the difference between P2 and end expiratory (PEEPi) plateau pressure on the Ptr trace and the expiratory tidal volume (Vt). The static elastance of the lungs (Est,L) was recorded as the ratio described above, but using the Pltrace. The static elastance of the chest wall (Est,w) was computed by subtracting Est,L from Est,rs. The dynamic elastances of the respiratory system (Edyn,rs), and lungs (Edyn,L) were measured by dividing P1–PEEPi on the Paw or Ptr and Pl tracings, respectively, by Vt. The dynamic elastance of the chest wall (Edyn,w) was computed by subtracting Edyn,L from Edyn,rs.
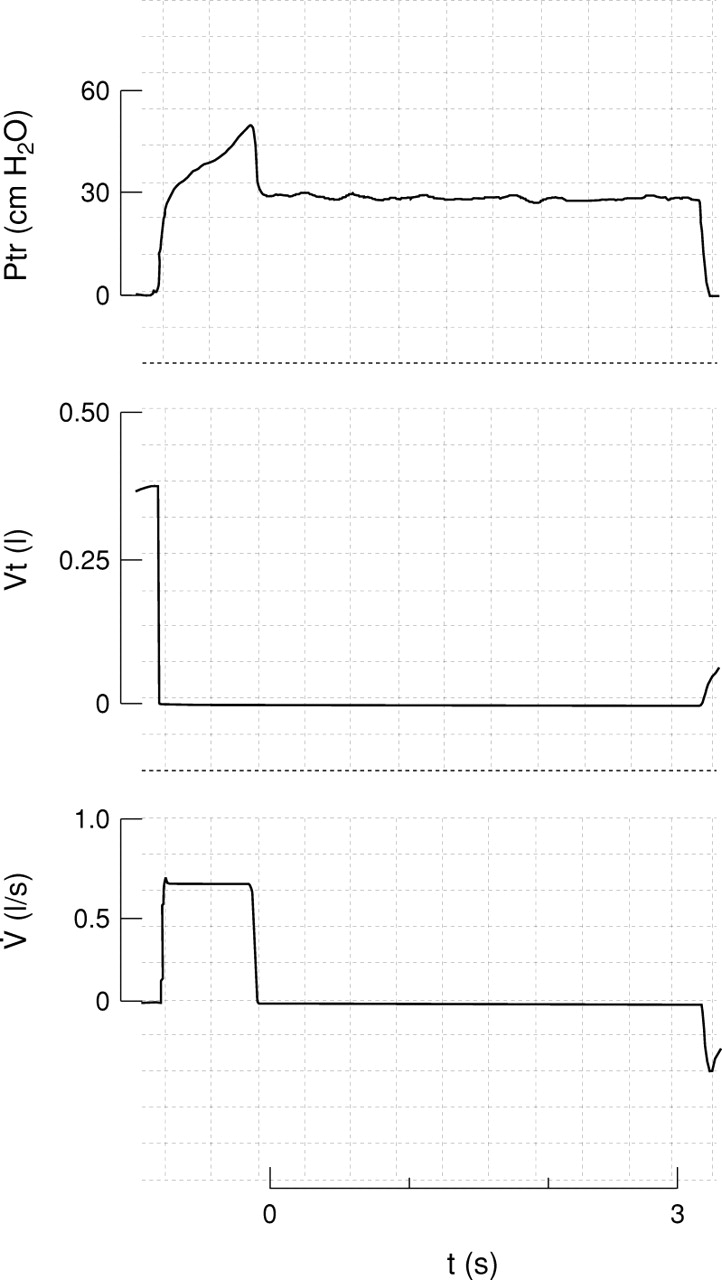
Typical record of a patient during the end inspiratory occlusion manoeuvre. Ptr = tracheal pressure, Vt = tidal volume,V˙ = airflow. Note that an apparent plateau in Ptr was reached before three seconds.
We computed the flow resistive properties of the endotracheal tubes by dividing the difference between peak Paw and peak Ptr by the preceding constant inspiratory flow.9 The so called interrupter resistances of the total respiratory system (Rint,rs), lung (Rint,L), and chest wall (Rint,w) were computed by dividing (Pmax–P1) from the Ptr, Pl, and Poes tracings, respectively, by the preceding constant flow and subtracting the resistance of the endotracheal tube. The slow decay in pressure (P1–P2) divided by the flow preceding the occlusion yields the effective additional resistance of the total respiratory system (ΔR,rs), lung (ΔR,L), and chest wall (ΔR,w). The sum of interrupter resistances and additional resistances represents the total resistance of the respiratory system (Rrs), lung (Rl), and chest wall (Rw). In the calculation of resistances the error due to the closing time of the valve of the ventilator was corrected.17
DATA ANALYSIS
The breathing pattern was analysed over a two minute period of spontaneous breathing in oxygen. All signals were recorded on an eight channel recorder (Gould TA 4000, Valley View, Ohio, USA). They were sampled at 100 Hz by an analogue-to-digital converter and stored on a personal computer (Vectra 386/20N, Hewlett Packard, USA) for subsequent analysis. The mean value from three measurements was used for each physiological variable. The results are expressed as mean (SD). Statistical analysis was performed using the Student’st test for paired observations. Correlation analysis was used to assess the associations between variables. A p value of <0.05 was considered significant.
Results
Only one out of seven patients was extubated and passed to non-invasive ventilation five days after intubation, while the others died after 3.2 (4) days of ventilation. The causes of death were mainly related to hypoxia refractory to oxygen therapy. No signs of new pulmonary infections or increased lung water, compared to those on the initial radiograph, were observed before the patients died. One patient developed bilateral basal atelectasis 24 hours after the measurements of respiratory mechanics. Two of the patients also had multiple organ failure.
The breathing pattern immediately before intubation was characterised by an increased breathing frequency and reduced tidal volume (table 1). PEEPi was present in only one patient and was 1.3 cm H2O for PEEPi,rs, 1.0 cm H2O for PEEPi,L, and 0.3 cm H2O for PEEPi,w.
Figure 2 shows the elastance of the respiratory system, lung, and chest wall during passive ventilation for each patient. Mean Edyn,rs was 60.91 (7.28) cm H2O/l while Edyn,L and Edyn,w were 53.90 (7.98) cm H2O/l and 7.01 (1.98) cm H2O/l, respectively. Mean Est,rs was 51.91 (7.22) cm H2O while the values for Est,L and Est,w were 46.08 (8.06) cm H2O/l and 6.02 (0.80) cm H2O/l, respectively. The contribution of lung elastances to the respiratory system elastances amounted to 88% and 89% for Edyn,rs and Est,rs, respectively. Edyn,rs and Edyn,L were significantly higher than Est,rs and Est,L, respectively (p<0.05).
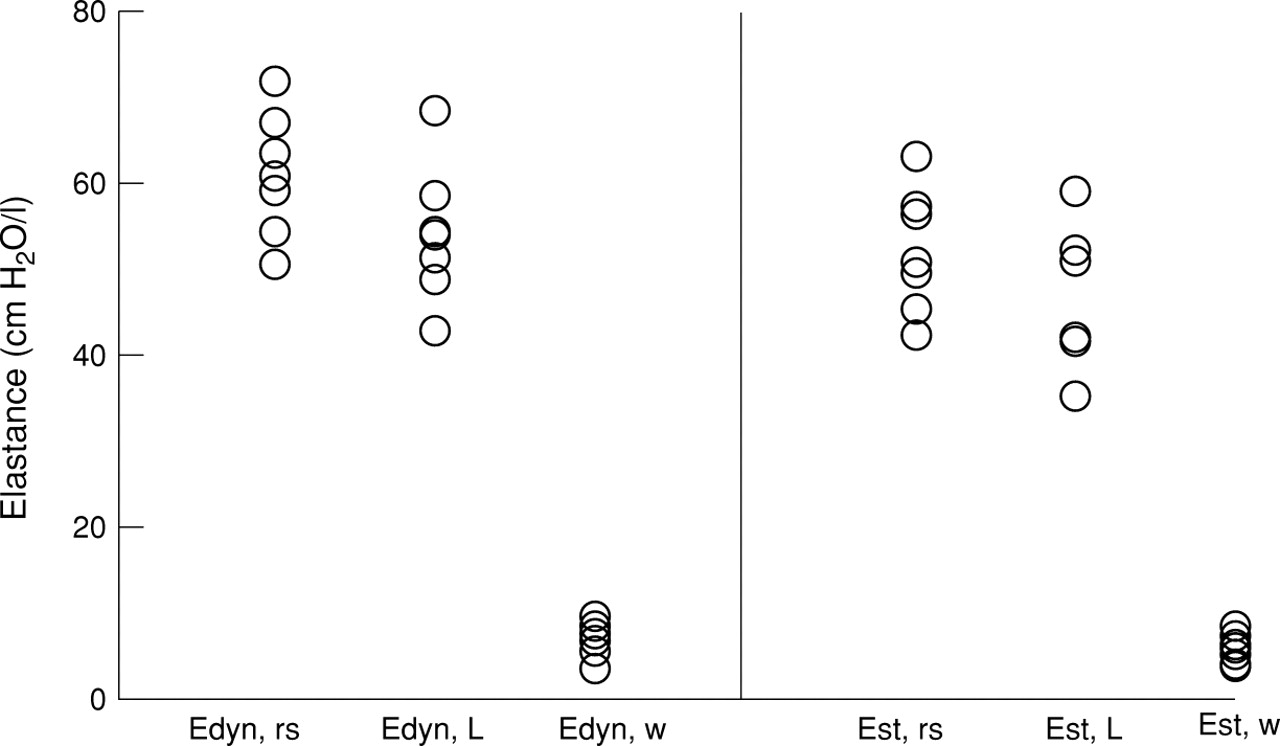
Individual values for dynamic and static elastances of the total respiratory system (Edyn,rs and Est,rs), lung (Edyn,L and Est,L) and chest wall (Edyn,w and Est,w).
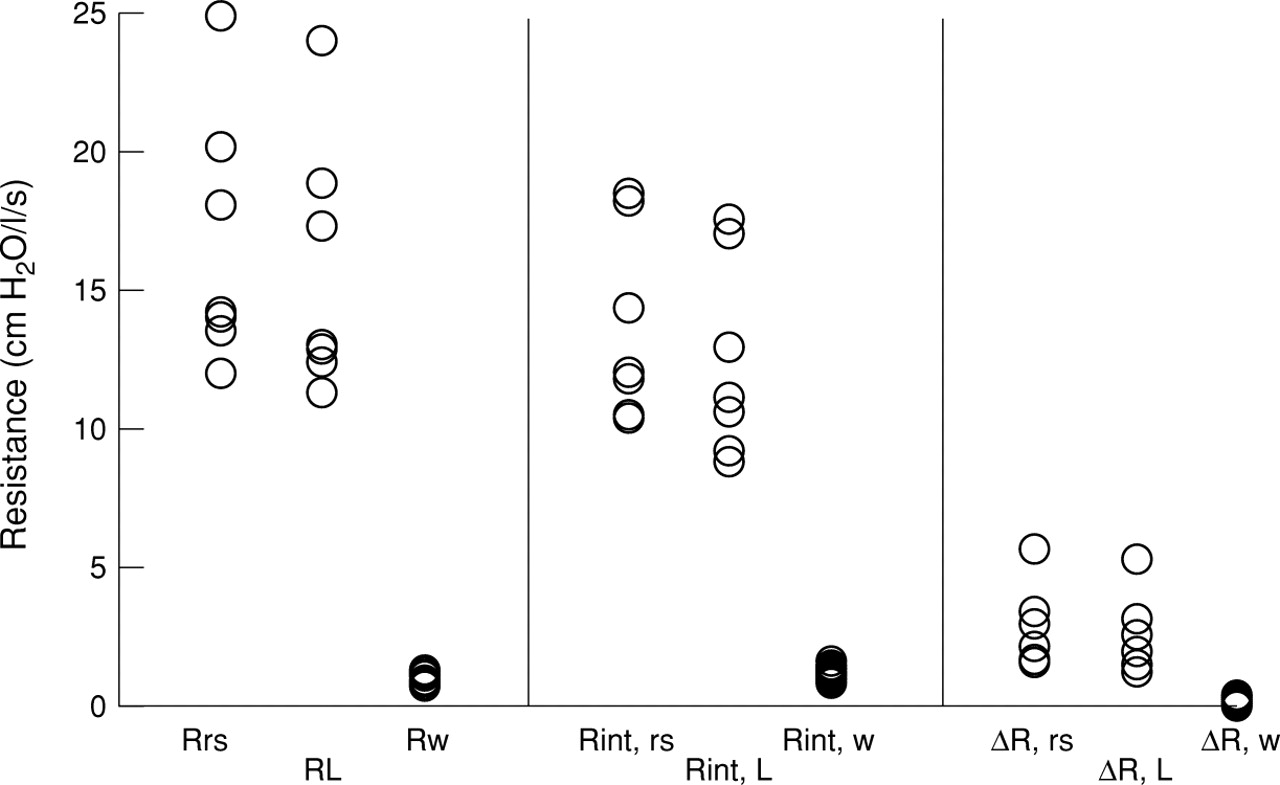
The resistances of the respiratory system, lung, and chest wall for each patient are shown in fig 3. Mean Rrs was 16.70 (4.61) cm H2O/l/s, while Rl and Rw were 15.27 (4.61) and 1.14 (0.29) cm H2O/l/s, respectively. Rint,rs was 13.68 (3.45) cm H2O/l/s while the values for Rint,L and Rint,w were 12.47 (3.57) and 1.21 (0.24) cm H2O/l/s, respectively. ΔR,rs, ΔR,L and ΔR,w were 3.02 (1.42), 2.80 (1.39), and 0.25 (0.11) cm H2O/l/s, respectively.

Individual values for the total resistances of the total respiratory system (Rrs), lung (Rl) and chest wall (Rw), for the interrupter resistances of the total respiratory system (Rint,rs), lung (Rint,L) and chest wall (Rint,w), and for the effective additional resistance of the total respiratory system (ΔR,rs), lung (ΔR,L) and chest wall (ΔR,w).
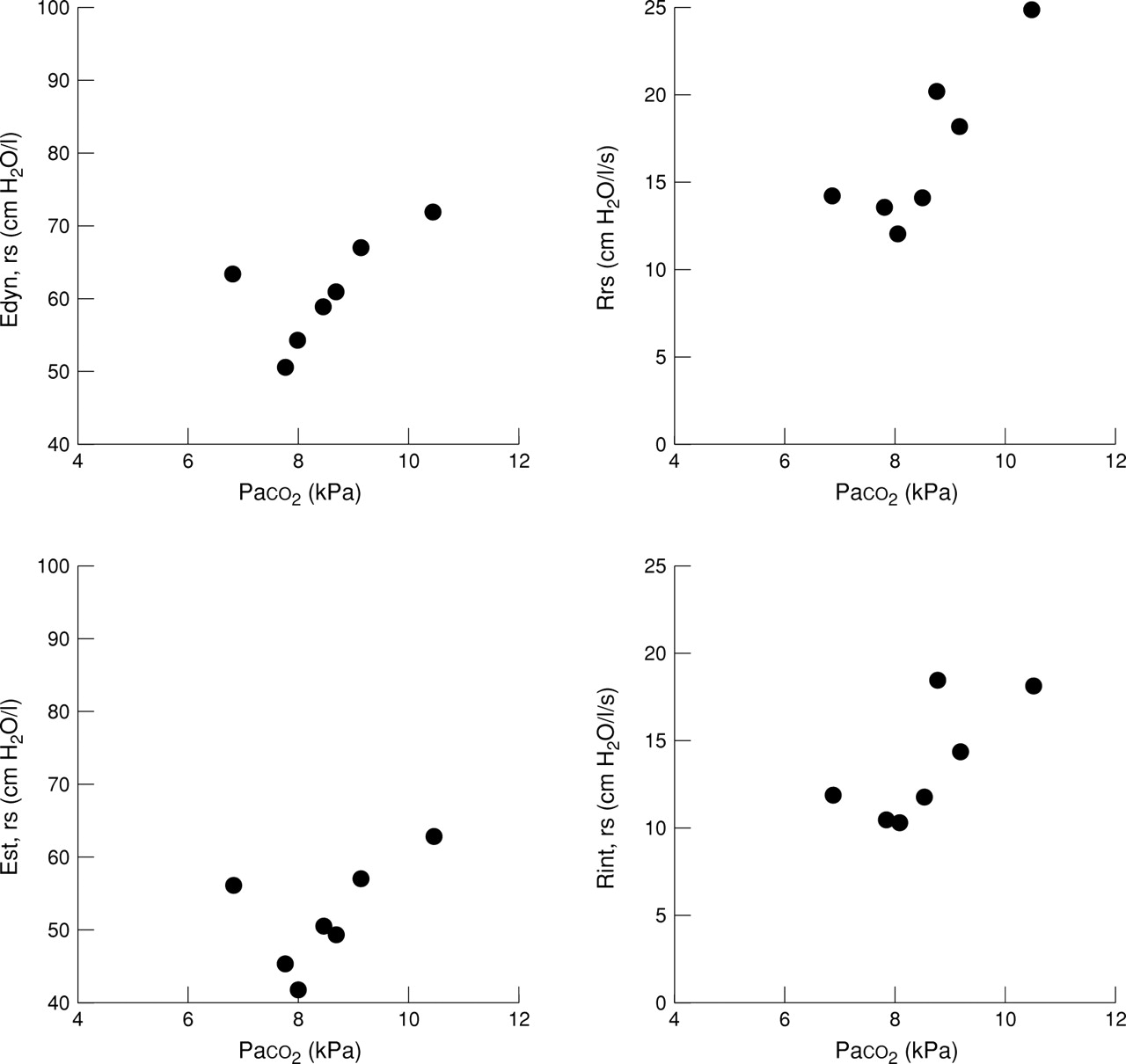
Figure 4 shows the correlation analysis between the degree of alteration in mechanical variables and the level of Paco 2 recorded just before intubation. Edyn,rs Est,rs, Rrs, and Rint,rs were significantly correlated with the degree of hypercapnia (r = 0.64 (p<0.01), 0.54 (p<0.05), 0.84 (p<0.001) and 0.72 (p<0.001), respectively). Tidal volume (Vt) and breathing frequency (f) were also significantly correlated with some mechanical variables, but these correlations were rather weak (Vt and Rint,rs, r = 0.38 (p<0.05); Vt and Est,L,rs, r = 0.41 (p<0.05); f and Rrs, r = 0.39 (p<0.05); f and Edyn,rs, r = 0.46 (p<0.05)).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation analysis between dynamic (Edyn,rs) and static (Est,rs) elastances of the respiratory system, total resistances (Rrs) and interrupter resistances (Rint,rs) of the total respiratory system, and arterial carbon dioxide tension (Paco 2 ).
Discussion
In this study we have provided information for the first time about partitioning of elastic and resistive properties of the total respiratory system between lung and chest wall mechanics in mechanically ventilated patients with end stage idiopathic pulmonary fibrosis.
Idiopathic pulmonary fibrosis is a progressive disease. The median survival from the time symptoms are first reported is less than five years, irrespective of the response to treatment.18 ,19Late stages of the disease are characterised by breathlessness, hypoxia, and hyperventilation. When acute respiratory failure ensues, most of the patients develop hypercapnia so that death occurs unless mechanical ventilation is instituted. Mechanical ventilation offers us the unique possibility of measuring passive respiratory mechanics non-invasively while the patients are ventilated. Information is available in the literature concerning most disease of the respiratory system such as chronic obstructive pulmonary disease (COPD),8-13 adult respiratory distress syndrome (ARDS),7 ,11 postoperative complications,11and cardiogenic pulmonary oedema,10 ,13 but there are no data recorded from patients with interstitial lung disease. We have found that this last group of patients has gross abnormalities of pulmonary mechanics.
A significant increase in the elastance of the respiratory system was observed. The mean value reported in the present study is approximately four times that recorded in normal anaesthetised subjects20 and even higher than in a group of patients with ARDS who did not survive an episode of acute respiratory failure.7 The increase in elastance of the respiratory system was mainly due to the abnormally increased lung elastance. Some studies performed in spontaneously breathing subjects have already reported that dynamic or static compliance of the lung (the reciprocal of elastance) is reduced.2 ,5 These studies were performed in spontaneously breathing, apparently stable, patients. For example, the largest study reported was in 23 subjects2 with mild resting hypoxaemia, more than one third of whom had normal values of Pao 2. Nevertheless, the authors of the study reported that a reduction in lung distensibility was significantly correlated with the severity of the morphological stage of the disease. There are many reasons why lung elastance is so markedly increased. Interstitial pulmonary fibrosis is characterised by severe alveolar fibrosis which reduces lung volumes. With the simple loss of lung volume the pressure/volume curve of the lung is contracted on its volume axis, therefore reducing the static or dynamic compliances. However, part of the explanation of the increased elastance may also be related to a “true” stiffness of the ventilated lung. Problems of volume correction may be avoided by fitting an exponential expression to the curve to obtain a shape factor (k), but this does not clarify the issue.5 It has also been suggested that loss of compliance may be due to the decreased amount of surfactant phospholipid present in patients with interstitial pulmonary fibrosis.21 Chest wall elastance only accounted for about 15% of the increase in the elastance of the respiratory system but it was, nevertheless, slightly above the normal value, probably due to the increased lung recoil which may displace the chest wall into the lower flat portion of the pressure/volume curve.
The resistance of the respiratory system was also markedly increased compared with the values reported for normal subjects,20 ,22 although to a lesser extent than that reported for patients with COPD.8-13 Lung resistances accounted for most of the total amount. It is rather surprising that Rint, estimation of airway resistance, was so high in patients with increased lung recoil, which should theoretically increase airway calibre. Interestingly, West and Alexander23 found that patients with higher respiratory work per breath also had increased resistive work compared with normal subjects. Indeed, Gibson and Pride3 suggested that the decreased lung volume observed in their patients with fibrosing alveolitis could result in a decrease in upstream conductance, even without structural changes in the airway which are, however, likely to be present in our patients affected by end stage disease. An interesting finding of our study is the increase in ΔR that reflects the viscoelastic properties and the time-constant heterogeneity within the respiratory tissue. Idiopathic pulmonary fibrosis in its late stages is characterised by patchy pathological findings so that advanced fibrotic changes occur in some areas, especially subpleurally, whereas other areas have more activity.24 These different histological features within the same interstitial tissue may explain this increase in ΔR since it is likely that, together with functionally deranged alveoli, some others may at least be partially preserved which may lead to time-constant heterogeneities.
Some methodological problems should be discussed. Firstly, the values of the mechanics of the respiratory system obtained during mechanical ventilation may not truly represent the values that occur during spontaneous breathing. This is particularly true for the measurements of chest wall mechanics which are likely to be affected by curarisation and sedation. Westbrook et al 25found that the static volume/pressure curve of the chest wall either shifts to the right or becomes less curved at low lung volumes with induction of anaesthesia paralysis. The measurements of respiratory mechanics must, however, be performed with the patients sedated to avoid any active contribution which would profoundly alter the recordings. Curarisation has been shown not to affect elastance or resistance of the respiratory system further after anaesthesia.26 Secondly, the end expiratory occlusion was held in this study for three seconds. This time interval has been used in most of the studies in the literature9 ,10 ,27 although recent recommendations are for a five second interval to allow true static recoil conditions to be reached.28 As shown in fig1, three seconds were usually enough to reach an apparent plateau in tracheal pressure, even though occlusion had to be prolonged in one patient who reached this plateau later. While three seconds may not be enough in most patients with COPD due to important time-constant heterogeneity, it should be sufficient for patients with idiopathic pulmonary fibrosis in whom we have shown the change in resistance which reflects this heterogeneity to be about 30% lower than in patients with COPD.9 Thirdly, we examined only one setting of the ventilator. It has been shown in normal anaesthetised paralysed subjects that Rint,rs increases linearly with increasing flow and so the fixed inspiratory flow used in the present study (0.60 (0.2) l/s) may be higher than that produced during spontaneous breathing. While this is true for normal subjects, it is not necessarily the case in patients with increased respiratory resistance in whom Eissa and coworkers27 found that resistance and static elastance did not change with increasing inspiratory flow.
The results of this study confirm the abnormal respiratory mechanics in patients with idiopathic pulmonary fibrosis. Most of the abnormalities are likely to be a reflection of the progressive inflammatory process that leads to interstitial fibrosis and reorganisation of the lung architecture. Since alveolar hypoventilation is uncommon in these patients before death, it is possible to speculate that, during the course of the disease, inspiratory muscles have the time required to adjust mechanically and metabolically to the increased workload. In the very end stages of the disease the lungs are likely to become so stiff and the resistances increase to such a point that the respiratory muscles can no longer sustain the loads. The breathing pattern would therefore be characterised by the typical rapid shallow breathing pattern present in all our patients before intubation, leading to progressive hypercapnic respiratory failure. Some of the correlations found between the degree of hypercapnia and respiratory mechanics, even though rather weak, may indirectly suggest that the more severe is the alveolar hypoventilation, the greater the degree of mechanical changes.