Article Text

Abstract
BACKGROUND There is an increase in vascularity in the asthmatic airway. Although inhaled corticosteroids (ICS) are an effective anti-inflammatory treatment in asthma, there are few data on any effects on structural changes.
METHODS Endobronchial biopsy specimens from seven asthmatic subjects not receiving ICS and 15 receiving 200–1500 μg/day beclomethasone dipropionate (BDP) were immunohistochemically stained with an anti-collagen type IV antibody to outline the endothelial basement membrane of the vessels. These were compared with biopsy tissue from 11 non-asthmatic controls (four atopic and seven non-atopic).
RESULTS There was a significant increase in the density of vessels (number of vessels/mm2 of lamina propria) in the asthmatic subjects not on ICS compared with non-asthmatic controls (mean 485 (interquartile range (IQR) 390–597) versus 329 (IQR 248–376) vessels/mm2, p<0.05; 95% CI for the difference 48 to 286). There was no significant difference between asthmatic subjects on ICS and those not on ICS or control subjects in the number of vessels/mm2 (mean 421 (IQR 281–534)). However, patients who received ⩾800 μg/day BDP tended to have a reduced number of vessels/mm2 compared with patients not on ICS and those receiving ⩽500 μg/day BDP (mean 366 (IQR 153–608) versus 494 (IQR 391–583), p = 0.08; 95% CI for the difference –31 to 288). Similarly, there was an increase in the percentage of lamina propria occupied by vessels in asthmatic patients not on ICS compared with controls (mean 15.6% (IQR 13.1–18.0) versus 10.1% (IQR 8.4–13.3), p<0.01; 95% CI for the difference 2.4 to 9.3) but a significant decrease in the percentage of lamina propria occupied by vessels was detected in asthmatic patients on ICS (mean 11.4% (IQR 9.1–14.9), p<0.01; 95% CI for the difference 0.7 to 7.7) compared with those not on ICS. The density of vessels correlated significantly with both airway hyperresponsiveness and percentage change in forced expiratory volume in one second (FEV1) after bronchodilator (r = –0.38 for PD20 methacholine and r = 0.49 for change in percentage FEV1 after bronchodilator versus number of vessels/mm2, p<0.05).
CONCLUSION These findings suggest that ICS, especially at higher doses, may reduce airway wall vascularity in asthmatic subjects but further longitudinal intervention studies are required to confirm this suggestion.
- airway vascularity
- asthma
- inhaled corticosteroids
Statistics from Altmetric.com
Asthma is a chronic inflammatory disease of the airways characterised by inflammatory cell infiltration and epithelial shedding. In common with other chronic inflammatory diseases such as rheumatoid arthritis and atherosclerosis, a tissue structural remodelling process seems to occur. This is evidenced by increased thickness of basement membrane,1 ,2 increased deposition of collagen in the lamina propria,2 smooth muscle hyperplasia/hypertrophy,3 and increased vascularity.4 The functional significance of airway remodelling in chronic asthma is not yet fully understood, but is invoked as a potential contributor to reduced airway distensibility5 as well as increased airway responsiveness and fixed airflow obstruction.6
Increased vascularity in airway lamina propria may have several consequences in asthma. The bronchial circulation plays an important role in the regulation of heat and water loss in the airway, and increased vascularity may predispose to exercise induced asthma in which such factors are important.7 The inflammatory process includes microvascular leakage,8 which may again be enhanced by such structural changes. However, perhaps the most important consequences of increased vascularity are the potential effects on non-specific airway responsiveness. Morphometric studies have shown that a small increase in airway wall thickness, such as that caused by oedema or circulation engorgement, may lead to a large increase in the narrowing of the airway lumen when airway smooth muscle contracts.6
Many mediators released during the inflammatory process from cells or nerves are potentially capable of causing bronchial vascular dilatation. Such factors include histamine,9bradykinin,10 and platelet activating factor.11 Adding to the complexity of events, some of these mediators have biphasic or triphasic responses causing both vasodilation and vasoconstriction, depending on the presence of other factors present locally in the airway. In addition, some inflammatory cytokines and growth factors which are present in the airway—for example, tumour necrosis factor-alpha (TNF-α), vascular endothelial growth factor (VEGF), basic fibroblast growth factor (bFGF), platelet-derived growth factor (PDGF), and endothelial growth factor (EGF)—can potentially induce angiogenesis.12 ,13 However, knowledge of factors that may influence human airway vascularity is limited.
Inhaled corticosteroids (ICS) are an effective treatment for asthma because of their anti-inflammatory action.14 ,15Furthermore, previous studies have shown that ICS could potentially reduce the increased thickness of the basement membrane in asthmatic subjects.16 ,17 Such studies suggest that ICS may have a potential therapeutic role in reversing the airway remodelling process. An effect of ICS on the increased vascularity observed in asthma has not previously been described. The aims of this cross sectional study were to determine whether the increase in vascularity observed in endobronchial biopsy specimens from asthmatic subjects was related to the use of ICS and to examine the relationship between vascularity and clinical physiological indices in asthmatic subjects, in particular bronchoconstrictor hyperresponsiveness (PD20 methacholine) and bronchodilator responsiveness.
Methods
ASTHMATIC AND CONTROL SUBJECTS
Twenty two asthmatic subjects (15 men) of mean age 44 years (interquartile range (IQR) 32–52) were recruited. All patients met the ATS criteria for asthma.18 They were divided into two groups: those not receiving treatment with ICS (n = 7; one non-atopic subject) and those being treated with ICS (200–1500 μg/day beclomethasone dipropionate (BDP)); (n= 15; five non-atopic). All the asthmatic patients had measurable airway hyperresponsiveness to methacholine (PD20 methacholine <2 mg) and had been on current medication unchanged for at least six months. Eleven non-asthmatic volunteers (eight men) of mean age 26 years (IQR 21–32 years) were also recruited. Seven were non-atopic and four were atopic. None had a history of asthma and all had a PD20methacholine of >6.4 mg. Individual patient details are shown in table 1.
Characteristics of study participants
All patients and control volunteers were current non-smokers. The study was approved by the Alfred Hospital ethics review committee and written consent was obtained from all subjects prior to bronchoscopy.
CLINICAL AND AIRWAY RESPONSIVENESS MEASUREMENTS
Atopy was determined as a response to one or more common aeroallergens (house dust mix, Southern grass, rye grass, cat fur, feather, Cladosporium, andAspergillus) on skin prick testing with a weal diameter of ⩾3 mm in the presence of a positive histamine and negative control reaction.
At screening, forced expiratory volume in one second (FEV1) was measured using a rolling seal spirometer (SensorMedics 2130; SensorMedics Corporation, California, USA). Patients withheld bronchodilators for eight hours. The best of three technically satisfactory readings was recorded. Salbutamol 200 μg was then given via a metered dose inhaler and spacer and FEV1 measurement was repeated 15 minutes later.
Within two weeks airway responsiveness to inhaled methacholine (PD20 methacholine) was measured under similar baseline conditions using a previously described dosimeter technique.19 Briefly, cumulative doubling doses of methacholine from 3 to 6400 μg were administered at five minute intervals until there was a decrement in FEV1 exceeding 20%. Results were expressed as the dose of inhaled methacholine estimated to provoke a 20% decrement in FEV1(PD20) by linear interpolation between the last two points on the dose-response curve.
FIBREOPTIC BRONCHOSCOPY AND ENDOBRONCHIAL BIOPSY PROCEDURES
For subjects on BDP the last dose was taken the night before bronchoscopy. If required for symptoms or if FEV1 predicted was less than 70% predicted, 200 μg salbutamol was given via metered dose inhaler and spacer shortly before bronchoscopy (indicated in table 1). Otherwise no bronchodilator was given to the asthmatic patients for four hours before bronchoscopy. Three of the control subjects were also given salbutamol prior to bronchoscopy in line with another study protocol that was being followed. Bronchoscopy was carried out under intravenous sedation with 2–10 mg midazolam (Roche, France). Pulse oximetry was performed throughout the procedure and supplemental oxygen was provided via nasal cannulae. The upper and lower airways were anaesthetised with topical 2% lignocaine. Six endobronchial biopsy specimens were taken from the subsegmental carinae of the right lower lobe using alligator forceps (Olympus, FB 15C, Japan); they were snap frozen in ornithine carbamyl transferase (OCT) in an isopentane/liquid nitrogen slurry immediately after bronchoscopy and stored at –80°C until indirect immunoperoxidase staining was performed.
IMMUNOHISTOCHEMICAL ANALYSIS
All reagents were from Dako, Denmark unless otherwise stated. Seven micron sections were cut on a Cryocut 1800 cryostat (Reichert-Jung, Heidelberg, Germany) onto poly-l-lysine coated slides in duplicate, approximately 35 μm apart. Sections were fixed in paraformaldehyde-lysine-periodate (PLP) and 10% normal rabbit serum/phosphate buffered saline (PBS) was used as blocking reagent of non-specific antigenic sites. Immunostaining was performed using a mouse anti-human collagen type IV monoclonal antibody diluted in 1% normal rabbit serum/PBS (1:3200). Subsequent addition of a biotinylated rabbit anti-mouse antibody (1:400 in PBS) was followed by horseradish-peroxidase conjugated streptavidin (1:600 in PBS). Metal enhanced diaminobenzidine (DAB; Pierce, Illinois, USA) was used as chromogen substrate and sections were then counterstained with haematoxylin. Each staining run included a negative isotype IgG1 control slide and nasal polyp positive control slide.
Slides were coded and assessed by one blinded observer (BEO). Sections were analysed by a method described previously.4 In brief, airway biopsy sections were analysed to a depth of 150 μm below the epithelial basement membrane using a computerised image analyser (Video Pro 32, Leading Edge Pty Ltd, Adelaide, Australia). Smooth muscle and glands were excluded. All structures internal to vessel endothelial basement membrane were included in the evaluated vascular area. For each patient at least five non-overlapping consecutive high power (×40) fields of one slide were assessed and the results were added together. The total number of vessels/mm2 of lamina propria was determined by dividing the number of vessels counted by the total area measured. In addition, the area occupied by vessels was expressed as a percentage of the total area of lamina propria assessed.
STATISTICAL ANALYSIS
Comparison between the groups was by a Kruskal-Wallis non-parametric ANOVA. The Mann-Whitney U test (two tail) was used to obtain p values. Data are presented as mean and interquartile ranges, and 95% confidence intervals (CI) are included for the differences found between groups. PD20 methacholine values were log10 transformed before analysis and are presented as geometric means and ranges. Comparison of lung function indices between groups was performed using a one way ANOVA. A Spearman correlation test was used to determine the relationship between physiological indices (PD20 methacholine and FEV1) and vascularity. p values of <0.05 were considered statistically significant after correcting for multiple comparison. Intra-observer variation was determined by counting two patients randomly chosen from each group twice at different times and determining the coefficient of variation (CV). Inter-observer variation was assessed by two observers (BEO and LZ) independently counting 10 control biopsy specimens. Variation between intra-observe and inter-observer analysis showed reproducibility in the counting technique. The intra-observer CV for the number of vessels/mm2 was 8% and for the percentage of area occupied by vessels was 4%. Inter-observer CV was 14% for the number of vessels/mm2 and 4% for the percentage of area occupied by vessels.
Results
There were no statistical differences observed between the two asthmatic groups in terms of airway hyperresponsiveness (PD20 methacholine), percentage FEV1 predicted (before and after bronchodilator), or in the percentage change in FEV1 after bronchodilator (table 1). The asthmatic patients had a mean FEV1 pre-bronchodilator of 88.3% predicted (IQR 73–99%) with a geometric mean (GSD) PD20 methacholine of 0.035 (IQR 0.01–0.09) mg. Asthmatic patients had a significantly reduced percentage predicted FEV1 pre-bronchodilator compared with the non-asthmatic controls (mean 105.4% (IQR 96–117%), p<0.01).
The total area of lamina propria measured for vessel evaluation below the basement membrane was similar for the three groups with an overall mean of 6.11 (IQR 5.82–6.70) mm2 × 10–2(table 2).
Summary of collagen type IV vessel staining in airway biopsy specimens
There was an increase in the number of vessels/mm2 (density of vessels) in asthmatic patients not receiving treatment with ICS compared with the non-asthmatic controls (mean 485 (IQR 390–597) versus 329 (IQR 248–376) vessels/mm2, p<0.05; 95% CI for the difference 48 to 286). Mean vessel density in the asthmatic patients treated with ICS was not statistically different from that in the asthmatic patients not on ICS or in the non-asthmatic controls, having a very wide range (421 (IQR 281–534) vessels/mm2). There was no correlation between dosage of ICS used by the asthmatic patients and the number of vessels/mm2(r = –0.26, p = 0.121; table 2, figs 1 and2). However, patients who received ⩾800 μg/day BDP tended to have a reduced number of vessels/mm2 when compared with patients not receiving ICS and those receiving BDP in a dose of ⩽500 μg/day (mean 366 (IQR 153–608) versus 494 (IQR 391–583) vessels/mm2, p = 0.08; 95% CI for the difference –31 to 288).
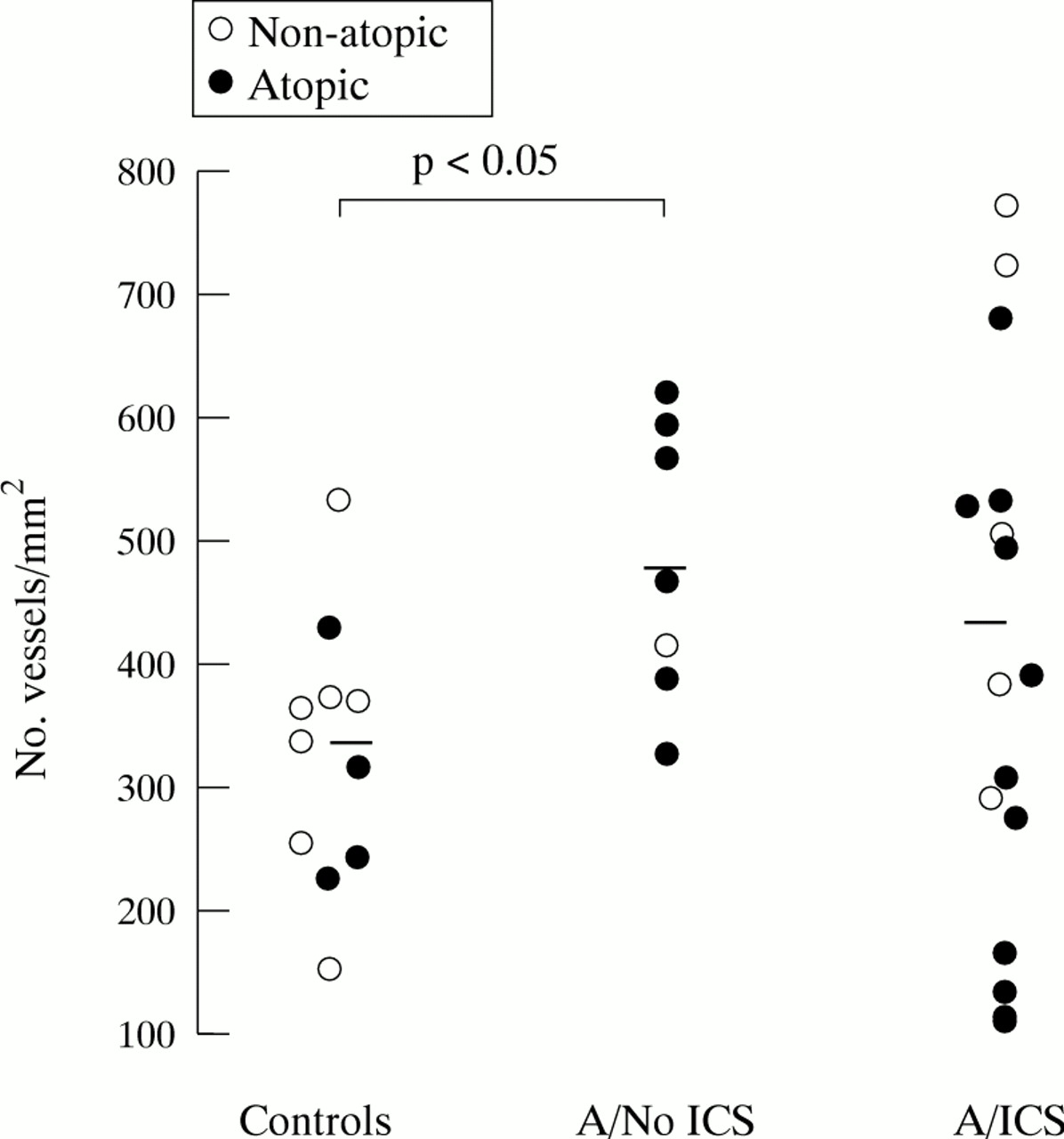
Number of vessels/mm2 in endobronchial biopsy specimens from asthmatic subjects (A) compared with those from non-asthmatic controls. The asthmatic subjects are divided into two groups, those receiving treatment with inhaled corticosteroids (A/ICS) and those not (A/No ICS).

Relationship between number of vessels/mm2in endobronchial biopsy specimens from asthmatic patients and dose of beclomethasone dipropionate (BDP).
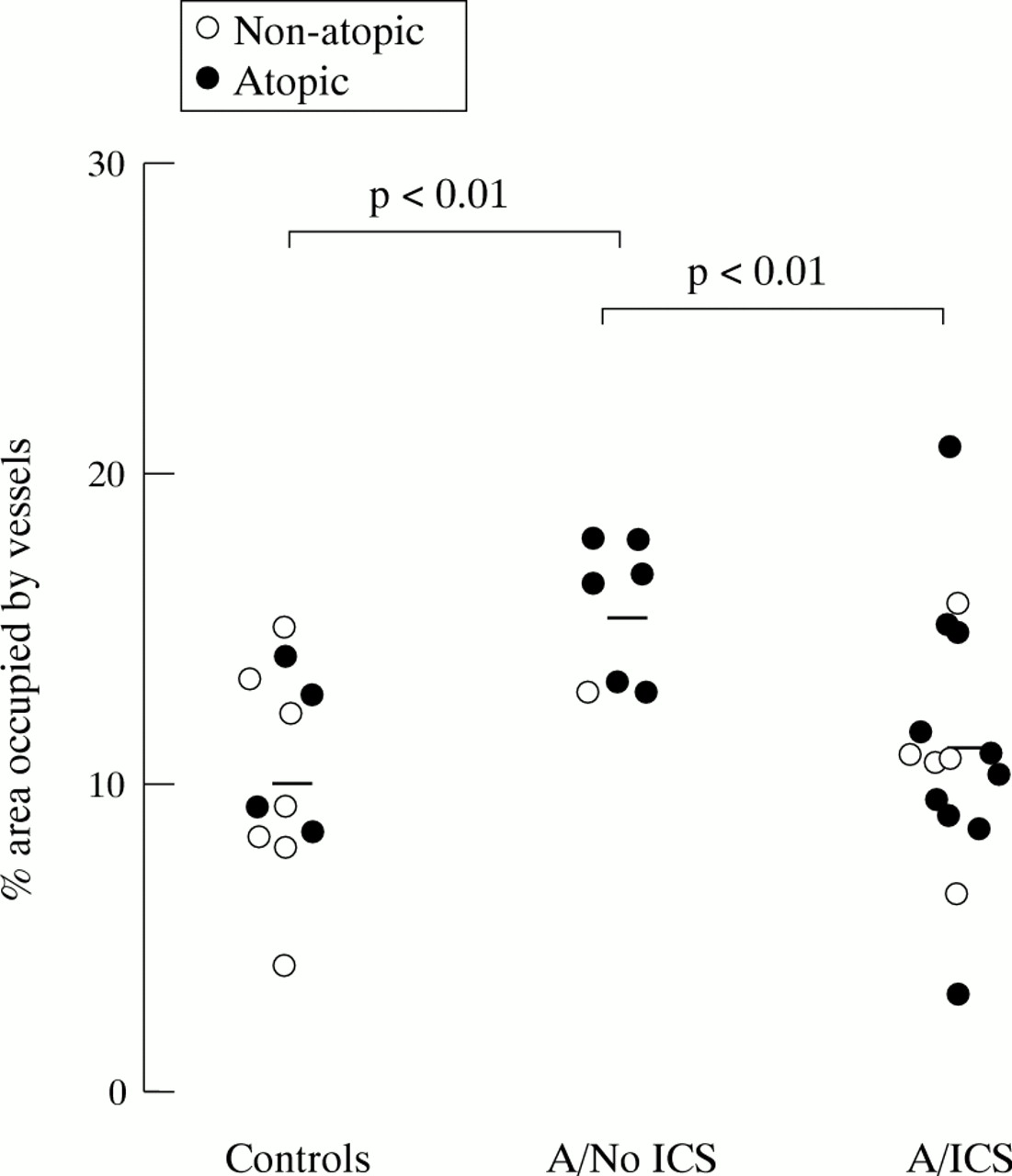
The percentage area of vascularity was significantly increased in the asthmatic patients not being treated with ICS compared with the non-asthmatic controls (15.6% (IQR 13.1–18.0%) versus 10.1% (IQR 8.4–13.3%), p<0.01; 95% CI for the difference 2.4 to 9.3). There was significantly less vascularity in asthmatic subjects receiving treatment with ICS than in those not treated with ICS (11.4% (IQR 9.1–14.9%) versus 15.6% (IQR 13.1–18.0%), p<0.01; 95% CI for the difference 0.7 to 7.7). There was a significant inverse correlation between dosage of ICS used by asthmatic patients and percentage area of vascularity (r = –0.58, p<0.01; table 2, figs 3 and 4). There was no difference observed in mean vessel size (μm2) between any of the groups (p = 0.69; table2).

Percentage area occupied by vessels in endobronchial biopsy specimens from asthmatic subjects (A) compared with those from non-asthmatic controls. The asthmatic subjects are divided into two groups, those receiving treatment with inhaled corticosteroids (A/ICS) and those not (A/No ICS).

Relationship between percentage area occupied by vessels in endobronchial biopsy specimens from asthmatic patients and dose of beclomethasone dipropionate (BDP).
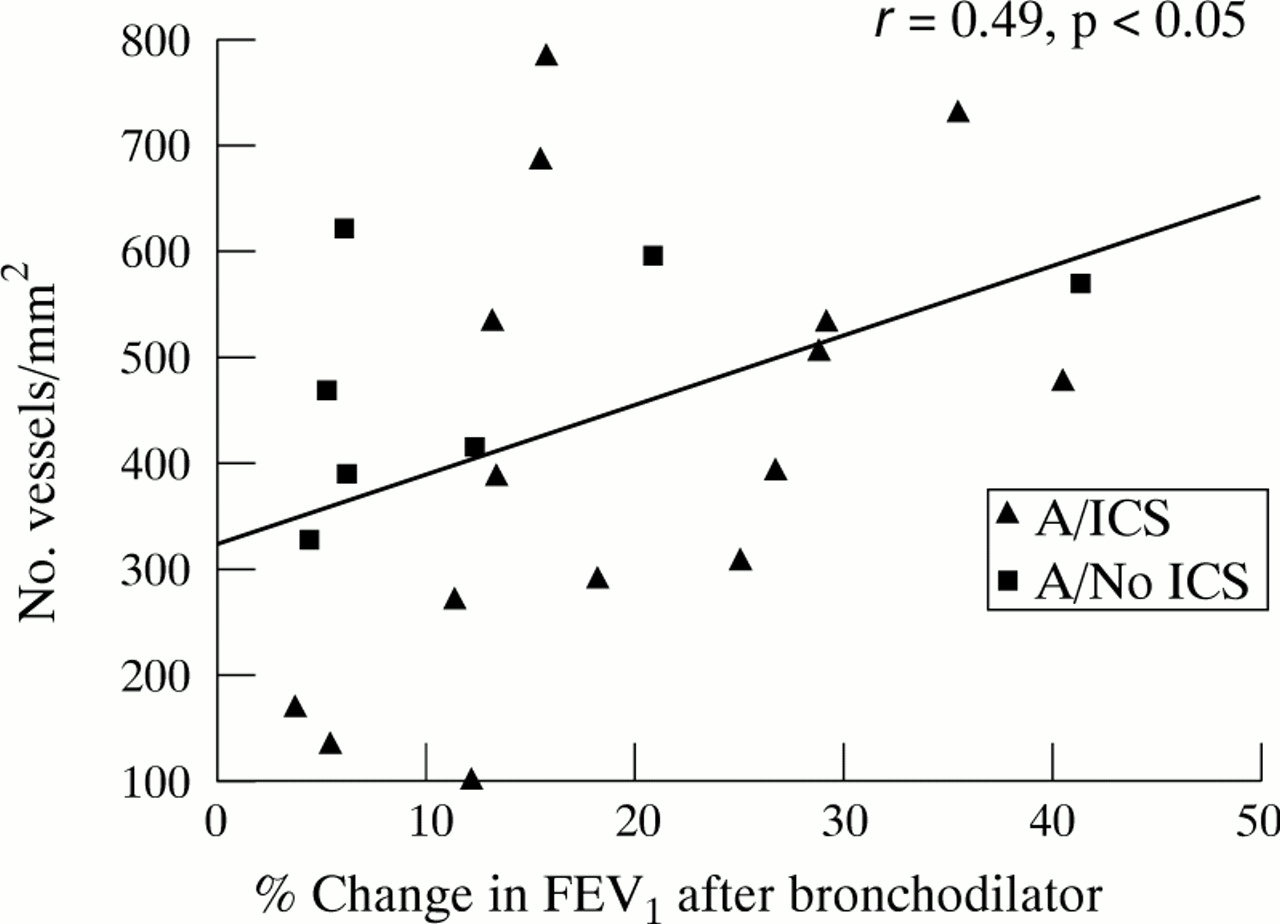
There was a significant inverse correlation between log PD20 methacholine and the number of vessels/mm2in the asthmatic subjects (r = –0.38, p<0.05; fig 5), showing that vessel density was greater in those patients with most marked hyperresponsiveness. There was no overall relationship between PD20 methacholine and the percentage area of vessels (r = 0.02, p = 0.457). There was also a significant positive correlation between percentage change in FEV1 with bronchodilator and number of vessels/mm2 (r = 0.49, p<0.05; fig 6) for the asthma patients overall. However, there was no significant relationship between percentage change in FEV1with bronchodilator and the percentage area of vessels (r = –0.07, p = 0.379).
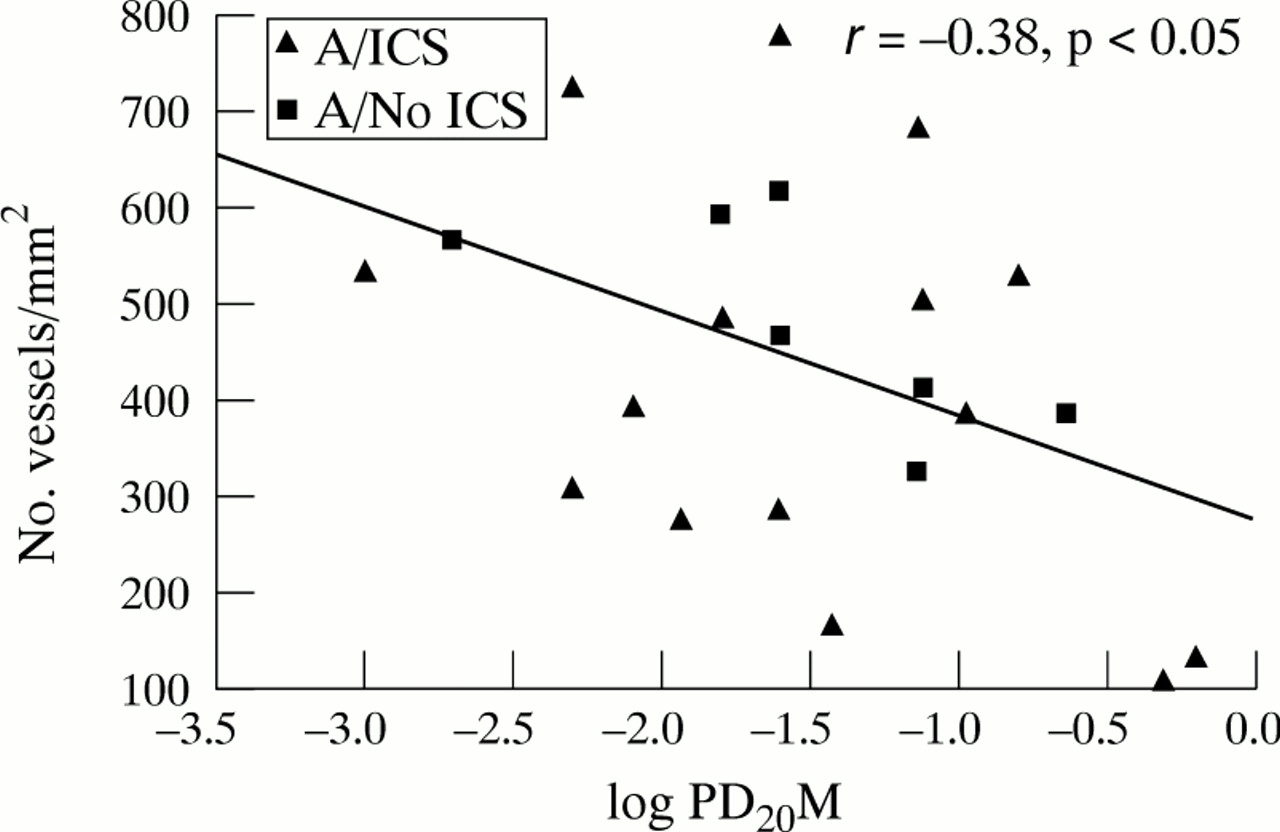
Relationship between number of vessels/mm2of lamina propria and hyperresponsiveness (log PD20methacholine (PD20M)) in endobronchial biopsy specimens from asthmatic patients. The asthmatic subjects are divided into two groups, those receiving treatment with inhaled corticosteroids (A/ICS) and those not (A/No ICS).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between number of vessels/mm2of lamina propria and percentage change in FEV1 after bronchodilator use in endobronchial biopsy specimens from asthmatic patients. The asthmatic subjects are divided into two groups, those receiving treatment with inhaled corticosteroids (A/ICS) and those not (A/No ICS).
Discussion
This study confirms our previous finding4 of an increase in bronchial vascularity in mild asthmatics, both in terms of number of vessels and area of the lamina propria occupied by vessels. We further show that there is an inverse correlation between dosage of ICS used by asthmatic patients and percentage area of vascularity in the lamina propria, which suggests that ICS may reduce vascularity in asthma. A significant relationship exists between vessel density and bronchial hyperresponsiveness in asthmatic subjects, suggesting that the degree of vascularity, and perhaps the potential capacity for engorgement of the airway wall, may play a part in the pathogenesis of hyperresponsiveness in asthma.
It has been recognised for some time that asthmatic subjects who die in acute attacks have an enlarged capillary bed in the airway wall.20 However, only recently have such changes attracted attention. Kuwano et al 21 found that there was increased vascularity of small airways in asthma compared with those in controls using anti-Factor VIII and trichrome stains on necroscopic and surgically resected specimens. There was no difference found in vessel numbers. Carroll et al 22 compared the bronchial vasculature in necroscopic specimens from eight cases of fatal asthma, 11 cases of non-fatal asthma and nine controls by using an anti-Factor VIII antibody to identify vessels. They found that both the number and area of large blood vessels were increased in the large cartilaginous airways in cases of fatal asthma, but without differences in total number or area of vessels between the groups. The difference between our results and those of other studies may reflect differences in study population, tissue source, sample size, tissue preservation and preparation, staining technique, and scoring method. We have found these changes to be reproducible in more than one patient group and when using different preparation techniques, with frozen sections being used in this study and ethanol fixed paraffin embedded biopsy specimens previously.4
The apparent increase in number of vessels/mm2 seen in asthmatic airway sections could potentially be due to an elongation of vessels which then fold in and out of the plane of section. However, it still suggests that vascular proliferative responses may be occurring, and the data support the hypothesis that angiogenesis is a component of airway wall remodelling even in mild to moderate asthma.
Many inflammatory mediators which have been shown to be increased in asthmatic airways share bronchomotor and vascular effects. Histamine,9 bradykinin,10 platelet activating factor,11 and mediators released by autonomic sensory nerves23 are airway mediators with potent vasodilator actions. In addition, some of the cytokines and growth factors associated with airway inflammation may have a part to play in airway wall remodelling and may be responsible for the increased number of vessels in asthmatic airways seen in this study. There is evidence to suggest that TNF-α is one such candidate which has been shown to be upregulated in asthmatic airways and to have pro-inflammatory and angiogenic effects.24 bFGF13 and VEGF12 are potentially potent angiogenic growth factors which may be released in the airway wall as part of the airway inflammatory response in asthma or as part of the remodelling response itself due to intramural mechanical forces.25
Inhaled corticosteroids have been shown to be the most effective anti-inflammatory treatment in asthma. They downregulate many inflammatory cytokines in the airway wall, such as IL-1, IL-4, IL-5 and GM-CSF,26 ,27 and in vitro studies have shown that they are also strong inhibitors of VEGF.15 Systemic glucocorticosteroids have also been reported to attenuate ozone induced increases in bronchial blood flow in sheep.28 In addition, recent studies have provided some evidence that treatment with ICS in mild asthma may be able to reverse basement membrane thickening, thought to be part of the remodelling process that occurs secondary to airway inflammation.16 ,17 Furthermore, the relative potencies of corticosteroids are assessed using the McKenzie skin assay, which relies on an acute vasoconstrictor response.29 The modulating action of corticosteroids on endothelial leakage may also involve a direct influence on vascular endothelium or neural reflex mechanisms, in addition to antagonism of inflammatory mediators.8
The finding that an inverse correlation exists between the dosage of ICS used by asthmatic subjects and the percentage area of vascularity supports our hypothesis. This dose-response relationship between the number of vessels/mm2 of lamina propria was not significant. However, it was shown that patients who received a dose of ⩾800 μg/day BDP tended to have a reduced number of vessels/mm2 compared with patients receiving no ICS and those receiving BDP in a dose of ⩽500 μg/day. The six subjects with the lowest number of vessels/ mm2 which fell within the normal range were all receiving a higher dose of ICS (⩾800 μg/day BDP), which suggests that a high dose of ICS may be needed to reverse the increased vascularity of the bronchial wall in asthmatic patients. Our study provides the first evidence that ICS may downregulate the increased vascularity in human asthmatic airways. A long term, longitudinal intervention study is needed to confirm this finding.
The fact that there was no difference between the asthmatic groups in baseline lung function, PD20 methacholine, and symptom score (data not shown) suggests that current disease activity per se was unlikely to be a major factor in determining the degree of airway vascularity. Some subjects were given salbutamol as premedication prior to bronchoscopy which could potentially have caused bronchial vasodilation and confounded the results when comparing the groups, although there was no evidence from the data that this was the case. In this study we attempted to avoid, as far as possible, any potential confounding due to age and atopy. Indeed, the difference between asthmatics and controls and the apparent effect of ICS on vascularity were confirmed after adjustments for the potential confounders (age, atopy, and bronchodilator premedication) by using analysis of covariance and multiple regression analysis.
The pathophysiological significance of increased vascularity in asthma is unclear. A model of airway wall thickening proposed by Morenoet al 6 suggests that a small increase in wall volume, such as that caused by oedema or vascular engorgement, might account for the increased airway responsiveness seen with bronchial provocation. Patients with impaired left ventricular function or left sided valvular disorders have been found to have heightened responsiveness to methacholine within the asthmatic range, presumably due to such an effect.30 In normal subjects a rapid intravenous infusion of fluid can induce similar changes in airway responsiveness. Intravenous administration of two litres of warm normal saline produced significant decrements in FEV1 (mean (SD) 0.65 (0.16) l) in eight asthmatic subjects and moderate reductions in eight normal subjects (0.33 (0.04) l).31The magnitude and duration of the change in the asthmatic patients was of the same quantitative and qualitative pattern as the change caused by moderately severe hyperventilation.31
There are several lines of evidence to suggest that airflow obstruction induced by exercise or isocapnic hyperventilation results from vascular hyperaemia without a significant airway smooth muscle component.32 In this situation it is thought that the temperature within the airway falls,7 associated with an increase in bronchial blood flow to supply sufficient heat to prevent thermal damage.33 When hyperpnoea suddenly ceases, a rebound hyperaemia follows with rapid rewarming of the airway wall resulting in engorgement of the capillary bed and perhaps oedema formation.7 Prevention or amplification of this rewarming has been shown to be able to increase or diminish airflow obstruction.33 Moreover, asthmatics are known to rewarm their airways twice as rapidly as normal subjects.7
Inhalation of specific antigen has been shown to lead to an immediate increase in total bronchial blood flow coincident with the immediate increase in airflow resistance in an ovine model.34 The late phase airway response was also preceded by a significant increase in bronchial arterial blood flow.34 These data, when taken together, offer strong indirect evidence that a dysfunction of bronchial circulation may play a part in the development of airway hyperresponsiveness in asthma. The significant inverse correlation between the number of vessels/mm2 in the bronchial lamina propria and methacholine hyperresponsiveness in asthmatic subjects found in the current study provides further evidence to support this hypothesis.
Interestingly, we found that the percentage area occupied by vessels, which may reflect the degree of engorgement of the vessels, did not significantly correlate with airway responsiveness. One explanation is that the number of vessels/mm2 represents the capacity for engorgement of the bronchial capillary beds, while the percentage area of vessels may represent the state of the vasculature at the one arbitrary time point when the bronchoscopy was performed and may be subject to premedication and fixation conditions.
We did not find a relationship between vascularity of the lamina propria and baseline pulmonary function. However, there was a significant relationship between vessel density and percentage change in FEV1 after bronchodilator. This may be another manifestation of the importance of tissue volume within the area circumscribed by the muscle layer in determining the physiological consequences of muscle contraction.6
In this study we have taken biopsy samples only from the central airways and are unable to directly extrapolate these findings to the small airways. However, Wiggs et al 35 and others have shown that there is continuous airway wall thickening from the small membranous (peripheral) airways to the large central airways which is more pronounced in the peripheral airways. Kuwano et al 21reported a twofold increase in the vascularity of the small airways of asthmatic subjects compared with controls. Thus, it is likely that increased vascularity is continuous from the central to peripheral airways and is a generalised airway change in asthma.
In summary, this study has shown that the increased vascularity in the airway wall in patients with mild asthma may be reduced by inhaled corticosteroids. The increased number of vessels/mm2 of lamina propria correlated with airway responsiveness and percentage change in FEV1 after bronchodilator, suggesting that angiogenesis in the asthmatic airway wall may have a significant role in the pathophysiology of asthma. Further longitudinal intervention studies are required, as well as investigation of the link between asthmatic airway inflammation and wall remodelling.
Acknowledgments
This study was supported by NH and MRC Australia, Glaxo-Wellcome Australia,the Alfred WTMSS, and the Alfred Hospital Foundation. We are indebted to Ros Bish and Sally Gollant (research nurses) for recruitment and assessment of patients. We also thank Dr Ling Zheng (LZ) for her assistance in quality control and Michael Bailey for statistical advice.