Article Text

Abstract
BACKGROUND Guidelines for asthma management focus on treatment with inhaled corticosteroids and on home recording of peak expiratory flow (PEF). The effect of maintenance treatment with inhaled corticosteroids on PEF variation and its relation to other parameters of disease activity were examined in 102 asthmatic children aged 7–14 years.
METHODS During 20 months of treatment with inhaled salbutamol, with or without inhaled budesonide (600 μg daily), forced expiratory volume in one second (FEV1), the dose of histamine required to provoke a fall in FEV1 of more than 20% (PD20), the percentage of symptom free days, and PEF variation were assessed bimonthly. PEF variation was computed as the lowest PEF as a percentage of the highest PEF occurring over 14 days, the usual way of expressing PEF variation in asthma self-management plans. For each patient using inhaled corticosteroids within subject correlation coefficients (ρ) were computed of PEF variation to the percentage of symptom free days, FEV1, and PD20.
RESULTS PEF variation decreased significantly during the first two months of treatment with inhaled corticosteroids and then remained stable. The same pattern was observed for symptoms and FEV1. In contrast, PD20 histamine continued to improve throughout the whole follow up period. In individual patients predominantly positive associations of PEF variation with symptoms, FEV1, and PD20 were found, but the ranges of these associations were wide.
CONCLUSIONS During treatment with inhaled corticosteroids the changes in PEF variation over time show poor concordance with changes in other parameters of asthma severity. When only PEF is monitored, clinically relevant deteriorations in symptoms, FEV1, or PD20 may be missed. This suggests that home recording of PEF alone may not be sufficient to monitor asthma severity reliably in children.
- asthma
- children
- inhaled corticosteroids
- peak expiratory flow
- home monitoring
Statistics from Altmetric.com
Current guidelines for management of childhood asthma focus on two principles: maintenance treatment with anti-inflammatory drugs (most commonly inhaled corticosteroids) and home recording of symptoms and peak expiratory flow (PEF).1 ,2 The effectiveness of inhaled corticosteroids for childhood asthma has been well established.3 Self-management programmes for childhood asthma, comprising both patient education and PEF based adaptation of the dosage of corticosteroids, are effective in reducing asthma morbidity in children.4 ,5 It is unknown, however, whether it is the education or the PEF monitoring that is responsible for this success. In fact, a study in adult asthmatic patients has shown that a PEF based self-management programme is no more effective than a programme based on education alone.6 Another study in adults showed that a symptom based self-management programme was just as effective as a PEF based programme.7 Similarly, it has been shown that education alone can reduce the exacerbation rate in childhood asthma.8 Despite the lack of knowledge on the usefulness of home monitoring of PEF, it has become very popular in contemporary asthma management. The Global Initiative for Asthma (GINA) guidelines recommend that every patient with asthma should have his own portable PEF meter and state that long term home recordings of PEF are desirable.2 In clinical practice this often means that asthmatic children of school age monitor their asthma and its response to treatment primarily based on home PEF recordings.9Indeed, the degree of variation of PEF is considered to be the golden standard for assessing the severity of childhood asthma and monitoring in some studies.10 ,11
Surprisingly few studies have examined changes in PEF over longer periods of time in asthmatic children. Most of these studies have been population based12-15 and the subjects in these studies received little, if any, treatment for asthma. To date no studies have been published on changes in PEF over time in asthmatic children receiving treatment with inhaled corticosteroids. We therefore analysed changes in home recorded PEF in asthmatic children during long term maintenance therapy with inhaled corticosteroids. The aim of the study was to assess the pattern of PEF variation over time and its relationship to changes in other parameters of disease activity.
Methods
Data from a long term multicentre study on inhaled corticosteroids in childhood asthma were used, details of which have been published previously.16 ,17 Inclusion criteria were a clinical diagnosis of asthma, demonstrable airways obstruction (defined as forced expiratory volume in one second (FEV1) 55–90% predicted or an FEV1/forced vital capacity (FVC) ratio of 0.5–0.75), airways hyperresponsiveness (defined as a provocative dose of histamine causing a 20% fall in FEV1 (PD20) of ⩽150 μg) after withdrawal of anti-inflammatory maintenance therapy, and age 7–14 years. Informed consent was received from all subjects and the study was approved by the hospital ethics review boards of all participating centres.
Before entering the trial all maintenance therapy for asthma was withdrawn and patients used inhaled β2 agonists on demand only for two weeks. Subsequently they were randomised to treatment, consisting of inhaled β2 agonists (salbutamol 200 μg) plus inhaled corticosteroid (budesonide 200 μg) (BA+ICS), or inhaled β2 agonists plus placebo (BA+PL), by metered dose inhaler three times daily administered in a double blind fashion. Rescue medication consisted of inhaled fenoterol dry powder.16
Patients returned to the clinic every two months. At each follow up visit the FEV1 was measured; PD20 histamine was assessed at alternate visits. FEV1 was expressed as a percentage of the reference (or predicted) value (FEV1%pred).18 PD20 values were log transformed before analysis.
Before each visit patients recorded symptom scores and PEF values (twice daily before inhaling trial medication) in a diary for 14 days. At the start of the study each patient received a new mini-Wright PEF meter (Clement Clarke, Harlow, UK) and standardised instructions on how to use it. At each follow up visit the PEF meter was brought along for inspection and each patient was asked to demonstrate a satisfactory PEF manoeuvre.
Diary cards with missing values for more than two of the 14 days were excluded from the analysis. For each diary card the percentage of symptom free days was calculated. Based on our earlier study,17 PEF variation was expressed as low%high (the lowest PEF value occurring over each 14 day period expressed as a percentage of the highest PEF occurring during that time period). This index was chosen rather than the commonly used amplitude%mean (highest PEF on each day minus the lowest PEF on that day, expressed as a % of their mean, averaged over 14 days), firstly because low%high is the expression commonly used in asthma self-management plans5and, secondly, because it has been shown to be more effective than amplitude%mean in identifying short episodes of reduced PEF.17 ,19
The relation of PEF variation to other indices of disease activity was examined in two ways. Changes in PEF variation (low%high) over time were compared with changes in symptoms and PD20 in the group treated with inhaled corticosteroids. In addition, for each patient in the BA+ICS group a within subject Spearman correlation coefficient was calculated between PEF variation and the % of symptom free days, FEV1%pred, and PD20. These analyses were confined to the BA+ICS group because this group received treatment that is now considered to be the standard care for asthmatic children. The treatment applied to the other group (maintenance treatment with inhaled bronchodilators) is no longer advocated, and the relationship between different indices of disease activity in this study group was considered to be less relevant.
WITHDRAWALS AND THEIR INFLUENCE ON RESULTS
The length of follow up from randomisation to termination of the study ranged from 10 to 28 (median 22) months. The study was terminated because about 40% of the patients in the BA+PL arm had to be withdrawn from the study due to worsening of their asthma.16 Because of this selective withdrawal and variable follow up, the number of diary cards available for analysis decreased rapidly after 20 months of follow up. The results are therefore confined to the first 20 months of blinded follow up. Children who were withdrawn from the study had lower levels of PEF, FEV1, and PD20 than children who remained in the study. As a result, mean levels of these indices in the BA+PL group are inflated due to selective withdrawal of those with lower levels.16
PEF CORRECTIONS
PEF can be corrected for height although, even after such a correction, considerable variation in PEF between subjects remains.20 This is one of the reasons why PEF is usually not expressed as a percentage of a height corrected reference value in asthma self-management plans. Instead, each PEF level is expressed as a percentage of the patient’s best value. For the purpose of this paper analyses with PEF were performed, both with and without height correction. Similarly, analyses of PEF were performed with and without correction for the inaccuracy of the PEF meter.21 ,22
Statistical analyses were performed using SPSS for Windows, version 8.0.
Results
Of 116 children who were randomised to receive blinded medication,16 102 (75 boys) filled out their baseline diary card completely.17 Their mean (SD) age was 11 (2) years and mean FEV1 was 79 (12)% predicted. The geometric mean PD20 was 18.4 μg. Mean morning PEF was 281 (68) l/min, and mean afternoon PEF was 305 (76) l/min. The mean lowest PEF over the 14 day baseline period was 63 (16)% of the highest PEF during this period. Mean diurnal PEF variation (amplitude%mean) was 13.7 (8.1)%. The two treatment groups were comparable with respect to all baseline characteristics.16
PEF improved during the first two months in children on BA+ICS while remaining unchanged in the BA+PL group (95% CI for difference after two months 17 to 77 l/min for morning PEF and 10 to 71 l/min for afternoon PEF). This difference did not change during further follow up. In both groups PEF slowly improved throughout further follow up, which is attributable to increase in height.16 Correcting PEF values for these changes in height during the study did not alter the results of the analyses.
The changes in PEF variation over time in both treatment groups are depicted in fig 1. Low%high increased during the first two months of treatment with inhaled corticosteroids (95% CI for difference 6.6 to 20.5%) and then remained stable (95% CI for difference after 20 months of follow up 6.2 to 19.0%). Amplitude%mean followed a similar pattern of improvement. The small increases in PEF variation seen after the second month could be due in part to withdrawal of unstable patients with high PEF variation.
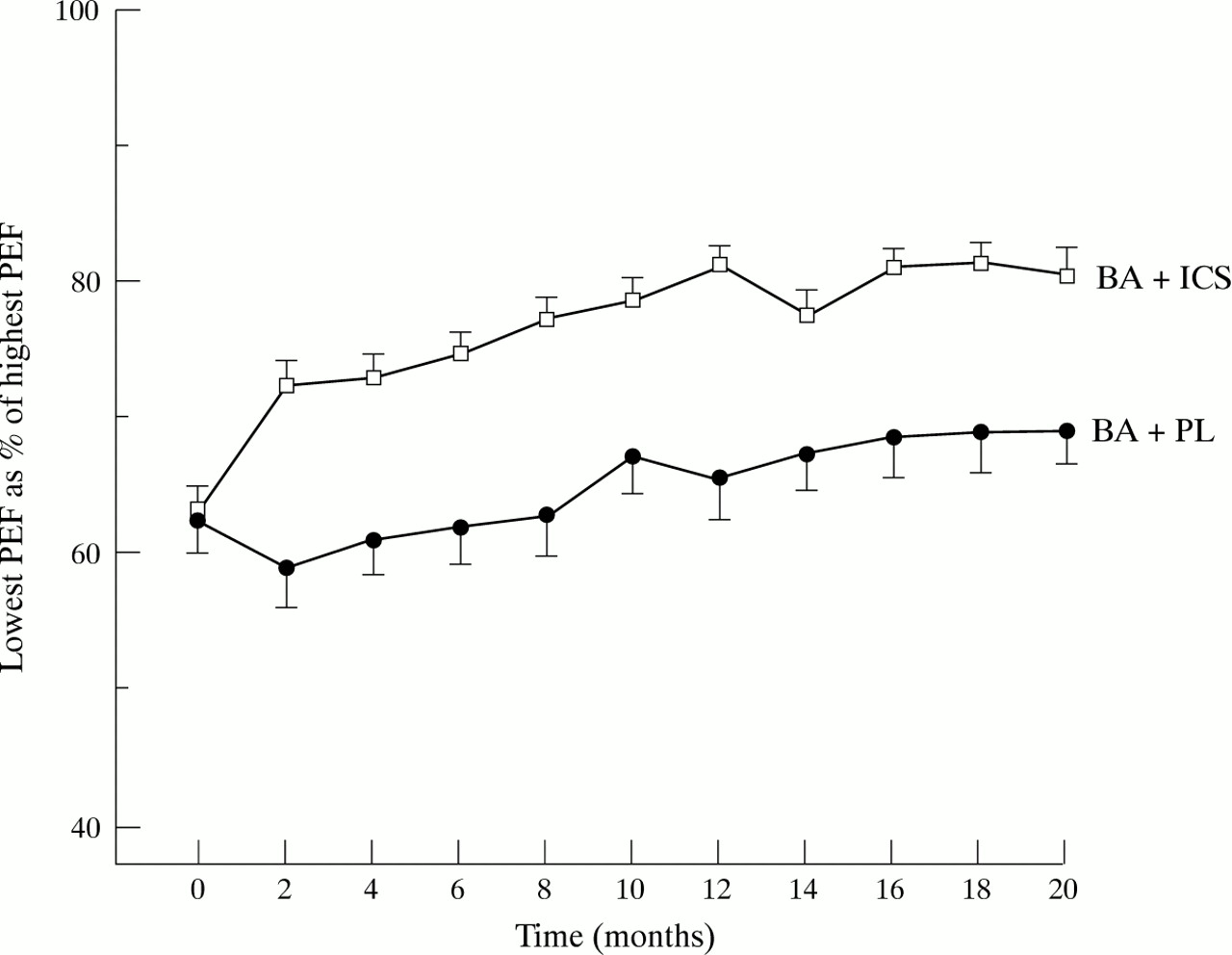
Changes in PEF variation (expressed as the lowest PEF level obtained in each follow up period as a percentage of the highest PEF level occurring in that period, low%high) during treatment with inhaled β2 agonists alone (closed circles) or in combination with inhaled corticosteroids (open squares). Data points represent mean values; bars represent standard errors.
In fig 2 changes in three different indices of disease activity during maintenance treatment with inhaled corticosteroids are plotted. Whereas improvements in the percentage of symptom free days and PEF variation (low%high) levelled off after the first year of treatment, PD20 histamine continued to improve throughout the whole follow up period.

Changes in PEF variation (expressed as the lowest PEF level obtained in each follow up period as a percentage of the highest PEF level occurring in that period; open squares), percentage of symptom free days (triangles), and PD20 histamine (solid circles) in 44 children during long term treatment with inhaled β2 agonists and corticosteroids. Data points represent mean values; bars represent standard errors.
Forty four children in the BA+ICS group completed 20 months of follow up (table 1). For each of these children within subject Spearman correlation coefficients between low%high PEF, the percentage of symptom free days, PD20 histamine, and FEV1 % predicted were computed (fig 3, table 2). Predominantly positive associations were found and mean Spearman’s ρ values were significantly different from 0 (95% CI for mean ρ of low%high PEF to percentage symptom free days was 0.28 to 0.49, to PD20it was 0.27 to 0.49, and to FEV1 % predicted it was 0.19 to 0.37). However, the ranges were wide and, in a considerable number of patients, the correlation coefficients were negative (fig 3). The results of these analyses remained the same when another index of PEF variation (amplitude%mean) was used, and when PEF values were corrected for the inaccuracy of the mini-Wright PEF meter.
Mean (SD) or number (%)* baseline characteristics of 44 children who completed 20 months of follow up on maintenance therapy with inhaled β2 agonists and inhaled corticosteroids

{kind=link}
{kind=link}
{kind=link}
Within subject Spearman correlation coefficients of PEF variation (expressed as the lowest PEF level obtained in each follow up period as a percentage of the highest PEF level occurring in that period, low%high) to the percentage of symptom free days, PD20 histamine, and FEV1 % predicted in 44 children during long term treatment with inhaled β2agonists and corticosteroids. Points represent individual values for Spearman’s ρ; bars represent median values.
Median within individual Spearman correlation coefficients between various parameters of disease activity in 44 asthmatic children during long term (20 months) treatment with inhaled corticosteroids
Discussion
This study shows that maintenance therapy with inhaled corticosteroids in asthmatic children reduces PEF variation considerably. At first sight this result does not seem to be very surprising because the efficacy of inhaled steroids in childhood asthma is well established.3 ,16 Most studies on inhaled corticosteroids, however, have only assessed the effects on PEF levels, not PEF variation. This is curious because PEF variation is considered by many to be the golden standard of asthma severity.2 ,10 ,11 In only four studies have the effects of inhaled corticosteroids on PEF variation been reported. In mild or episodic asthma inhaled corticosteroids do not reduce PEF variation, probably because it was not very high at the start of the study.23 ,24 In moderately severe childhood asthma long term treatment with inhaled corticosteroids has been shown to reduce PEF variation.16 ,25 In each of these studies PEF variation was expressed as amplitude%mean. There is now accumulating evidence that this way of expressing PEF variation, apart from being very cumbersome to calculate, will fail to identify short lasting episodes of reduced PEF26 ,27 or clinically relevant symptomatic exacerbations.17 ,19 Such episodes are probably better appreciated by expressing PEF variation as the lowest level occurring over a given time period as a percentage of the highest level obtained over that time period. This expression has the additional advantages that it is very easy to calculate and corresponds with PEF indices used in self-management plans.17
We therefore chose to express PEF variation as the lowest value as a percentage of the highest value over a given period of time (low%high). In the analyses presented in this paper the use of amplitude%mean instead of low%high as an expression of PEF variation did not alter the results.
The most important finding of this study is that, during maintenance treatment with inhaled corticosteroids, changes in PEF variation correspond quite variably with other indices of disease activity. At group level improvements in symptom scores and PEF variation levelled off after 12 months of treatment whereas airways hyperresponsiveness to histamine continued to improve throughout the entire 20 month follow up period (fig 2). More importantly, a considerable number of individual patients showed improvements in symptom free days, FEV1, or PD20 histamine whilst their PEF variation worsened (fig 3, table 2). This observation is in accordance with earlier studies showing poor concordance of changes in PEF levels over time to changes in symptoms,28 FEV1,29 or methacholine responsiveness.28 These results show that, when only PEF values and their changes over time are recorded in asthmatic children, clinically relevant deteriorations in symptoms, airway calibre, and airways hyperresponsiveness may be missed. Clearly this is undesirable in the management of asthma in children.
Thus, the current emphasis on home recording of PEF may not be justified. At present there is no simple way of assessing the degree of airways inflammation in childhood asthma. As long as it is unknown which parameter provides the best or most important information on the severity and the course of childhood asthma, it appears prudent to have asthmatic children return to the clinic regularly to review their symptoms and to perform spirometric and/or other lung function tests, such as those aimed at assessing airways hyperresponsiveness. If PEF is recorded at home the values must be interpreted in the light of the clinical situation as well as using other parameters of disease activity.
The variable relation of changes in PEF to other indicators of disease activity may also explain why researchers have so far been unable to demonstrate the additional benefit of recording home PEF over and above recording symptom scores alone as a basis for adjusting therapy in asthma self-management plans.6 ,7 ,30 Currently available evidence suggests that the most important part of asthma self-management in children is to educate them to respond promptly to symptoms which suggest an impending exacerbation.4 ,8
In summary, this study shows that changes in PEF variation during long term treatment with inhaled corticosteroids in childhood asthma correlate quite variably to changes in symptoms, degree of airways obstruction, and histamine hyperresponsiveness. This indicates that recording changes in PEF level alone is insufficient to monitor asthma severity reliably in children. Home PEF records can be useful for assessing and monitoring asthma in children but should not be regarded as the golden standard.
Acknowledgments
This study was funded by a grant from the Netherlands’ Government Health Research Promotion Programme (SGO). Study drugs were supplied by Glaxo Wellcome, Astra, and Boehringer Ingelheim.