Article Text

Abstract
An 11 year old boy with cystic fibrosis suffered a stroke, producing right sided weakness. Four years previously a totally implantable venous access device (Port-a-Cath) had been inserted. Magnetic resonance angiography revealed a filling defect in the left middle cerebral artery. Transoesophageal echocardiography demonstrated a thrombus attached to the tip of the Port-a-Cath and also the presence of a patent foramen ovale. After an initial period of anticoagulation the defect was closed using a septal occlusion device introduced via a cardiac catheter. The boy's neurological signs completely resolved and he remains free from further thromboembolic episodes. Whilst pulmonary embolism has been described before in relation to a totally implantable venous access device, this is believed to be the first description of a paradoxical embolism in relation to such a device.
- cystic fibrosis
- paradoxical embolism
- catheterisation
Statistics from Altmetric.com
An 11 year old boy with cystic fibrosis was admitted to hospital with sudden onset of confusion and slurred speech. On examination he was found to have a right-sided hemiparesis, expressive and receptive dysphasia. He had originally presented at the age of two days with a meconium ileus and was subsequently found to be homozygous for the ΔF508 deletion. A sweat test performed at the age of four months confirmed the diagnosis of cystic fibrosis. Since the age of four he had required many hospital admissions for intravenous antibiotic therapy. In February 1992 a Port-a-Cath was inserted via the right internal jugular vein and secured to the anterior chest wall. His lung function was considerably compromised with a forced expiratory volume in one second (FEV1) of 0.63 l (35% predicted) and a forced vital capacity (FVC) of 0.98 l (49% predicted).
A computed tomographic (CT) brain scan performed on the day after admission revealed a poorly defined area of low attenuation in the left temporoparietal region which was suggestive of ischaemia in the territory of the left middle cerebral artery. Magnetic resonance angiography confirmed recent ischaemia in this region with evidence of an embolus in the left middle cerebral artery. A transthoracic echocardiogram was performed which showed an unusual Ebstein's-like deformity of the tricuspid valve; the proximal part of the septal leaflet of the tricuspid valve was displaced apically with a point of attachment in the mid body of the right ventricle. Mild tricuspid regurgitation was also seen but no other abnormalities were apparent.
Ebstein's anomaly is associated with abnormal intra-atrial connections and therefore a transoesophageal echocardiogram was arranged. This was performed under general anaesthesia and demonstrated a small patent foramen ovale, the anterior border abutting the posterior aspect of the ascending aorta. The Port-a-Cath was seen in the right atrium and was noted to impinge against the tricuspid valve during the cardiac cycle. In addition, a large thrombus was seen attached to the tip of the Port-a-Cath in the right atrium.
Despite using intravenous contrast, no right to left shunt was demonstrable during the procedure. Techniques to enhance any right to left shunt such as coughing and the Valsalva manoeuvre were not possible because of the general anaesthetic.
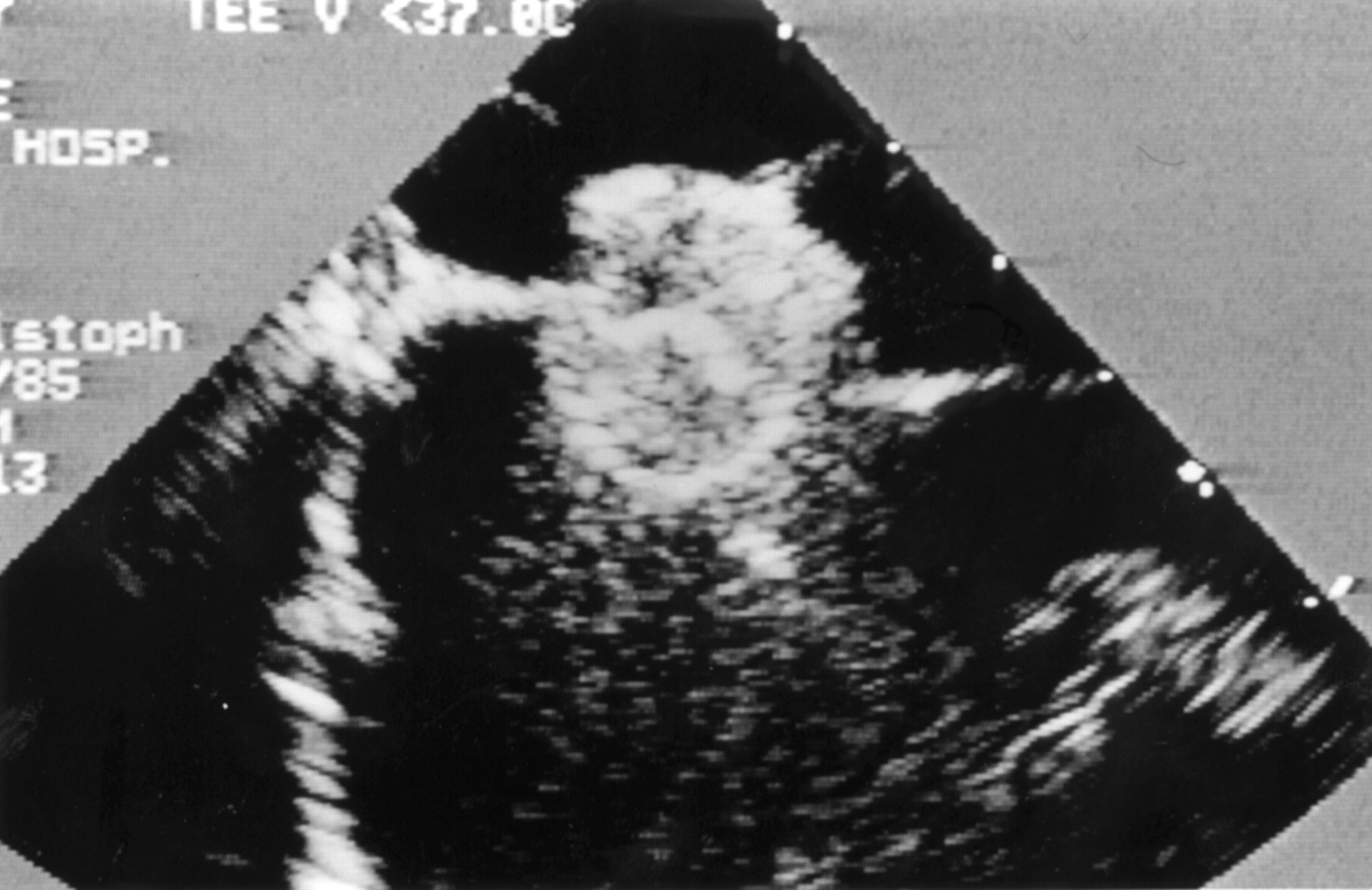
The patient was anticoagulated with warfarin and started on an anti-platelet dose of aspirin. One month later the defect was closed using a 9 mm atrial septal occlusion device introduced via a cardiac catheter (fig 1). By this time the neurological signs had completely resolved and aspirin was discontinued after three months. There have been no further episodes of thromboembolism.

{kind=link}
Septal occlusion device clamped across the atrial septum.
Discussion
Paradoxical embolism was first described by Cohnheim in 18771 but until 1930 only post-mortem cases were reported in the literature. In recent years more advanced techniques for detection of a patent foramen ovale have allowed the accurate diagnosis of presumptive paradoxical embolism during life.
Thromboembolism has been described as a complication relating to the use of totally implantable venous access devices2 but we believe this is the first time that a paradoxical embolism has been described in relation to the use of such a device.
Paradoxical embolism can only be considered proven if a venous thrombus is detected lodged in an intracardiac septal defect. This degree of certainty is extremely rare, but has been demonstrated during life using both transthoracic and transoesophageal echocardiography.3 ,4 More often we can assume paradoxical embolism if “Johnson's triad” exists—that is, (1) venous thrombosis with or without pulmonary embolism, (2) an intracardiac defect with right to left shunting, and (3) arterial embolism without a corresponding source in the left heart or proximal arterial tree.5
The reported incidence of a patent foramen ovale varies from 5% to 30%. In younger adults with ischaemic stroke, where the cause may be undefined in up to 35% of cases, the incidence of a patent foramen ovale is significantly higher at around 40%.6 This suggests that paradoxical embolism occurs more frequently than was previously thought.
Paradoxical embolism is more likely in the setting of a chronic cough, as in cystic fibrosis.Coughing and the Valsalva manoeuvre are used during contrast echocardiography to promote right to left shunting across a patent foramen ovale, and indeed coughing is felt to be the most effective manoeuvre to demonstrate such shunting.7
Any child with an unexplained stroke requires a careful cardiological examination, particularly if there are risk factors such as an indwelling venous access device and a chronic cough. If transthoracic echocardiography shows no abnormality then more invasive investigations should be considered such as transoesophageal echocardiography.
Transcatheter techniques such as that used in our patient can offer significant advantages over open surgery in patients with cystic fibrosis. Postoperative recovery is quicker with less interruption to physiotherapy, and the avoidance of sternotomy may have important implications for any proposed heart-lung transplantation.