Article Text

Statistics from Altmetric.com
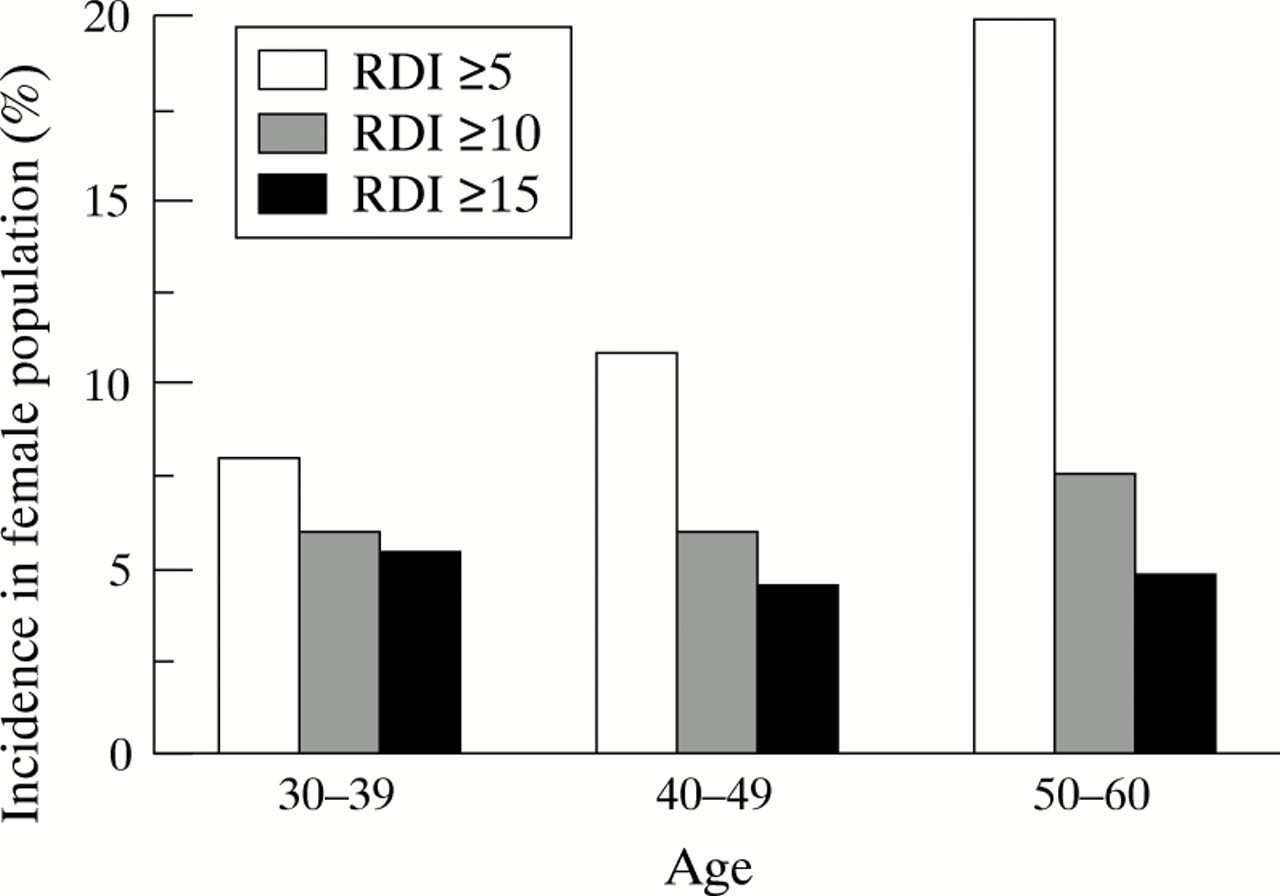
Until recently the occurrence of sleep disordered breathing in premenopausal women has been considered to be so low as to be insignificant and, as a result, research into the consequent cardiovascular risk in this group has been completely neglected. However, recent epidemiological evidence based on sleep clinic data suggests that the incidence of significant sleep disordered breathing in young women (30–49 years) is as high as 4.9% (fig1).1 Furthermore, while morbidity of women in the general population is lower than in men, recent epidemiological evidence suggests that five year survival is significantly poorer in women with obstructive sleep apnoea (OSA) than in a similar population of men.2 Thus, assessment of factors which may contribute to poorer outcomes in these women is important.

Age specific estimates of sleep disordered breathing in women. Contrary to many reports, these data suggest that the incidence of significant sleep disordered breathing in young women (most of whom will be premenopausal) is a significant public health issue. Modified from Young et al.1
Cardiovascular control in men with OSA
Men with OSA have an excess of known cardiovascular risk factors such as hypertension, obesity (particularly central obesity), and increased insulin resistance.3 There is increasing evidence to suggest that OSA interacts adversely with these factors. This interaction occurs during both wakefulness and sleep. Epidemiological evidence assembled in a community based population study in the USA suggests that, after adjusting for independent risk factors associated with hypertension, OSA was independently responsible for up to a fivefold increase in the incidence of hypertension.4 Furthermore, Carlson and coworkers5 suggest that, while OSA is an independent risk factor for hypertension, it also has an additive effect when combined with age and obesity. Thus, blood pressure control is seriously compromised in men as a result of the presence of OSA. Similar potential risks have not been investigated in women with obstructive sleep apnoea.
During sleep, men with OSA have repetitive obstructive respiratory events which are associated with characteristic pathophysiological changes in ventilation and haemodynamics. Fluctuations in haemodynamic parameters which accompany obstructive apnoea during sleep in men include initial bradycardia (vagally mediated) followed by tachycardia associated with arousal at apnoea termination.6 Similarly, systemic blood pressure decreases towards the conclusion of the apnoea followed by a surge in both systolic and diastolic pressure associated with arousal occurring at apnoea termination. Surges in sympathetic nerve activity are believed to be predominantly responsible for haemodynamic fluctuations which are associated with obstructive respiratory events during sleep.7-9 These changes in sympathetic nerve activity during obstructive events in sleep result from a number of factors including blood gas fluctuations (hypoxia and hypercapnia),10 large dynamic swings in intrathoracic pressure,11 ,12 and arousals from sleep.13While the result of these is an increased sympathetic tone overnight, increased sympathetic tone persists into the daytime in men with OSA.14 ,15 Daytime sympathetic tone in these patients is reduced to normal levels once effective treatment with nasal continuous positive airways pressure (CPAP) has been established.16
In men there is some evidence that OSA increases the risk of vascular events and increases mortality independently of other known risk factors.3 ,17 ,18 Haemodynamic fluctuations associated with obstructive events during sleep may contribute to the increased vascular risk in these men. Haemodynamics during obstructive apnoeas occurring in sleep have not to date been specifically investigated in either premenopausal or postmenopausal women.
Ventilatory control during the menstrual cycle
Until recently sleep disordered breathing in premenopausal women was believed to be a very rare occurrence. One of the predominant reasons cited for the supposed decreased incidence of sleep disordered breathing in premenopausal women was that they have greater central chemoreceptor drive, especially during the luteal phase of the menstrual cycle.19 ,20 It is well described that minute ventilation increases during the luteal phase of the menstrual cycle and, further, that ventilatory responsiveness to hypercapnia is increased during this phase.21-23 Furthermore, basal minute ventilation and ventilatory responsiveness to hypercapnia are both potentiated in men receiving synthetic progesterone (medroxyprogesterone acetate).24 Thus, increased ventilatory responsiveness during the luteal phase of the cycle is specifically modified by changes in serum progesterone concentrations.
While ventilation and central chemoreceptor drive have been extensively studied throughout the normal menstrual cycle during wakefulness, little attention has been focused on menstrual cycle related breathing parameters during sleep. In women without significant sleep disordered breathing (having an apnoea/hypopnoea index of <5/hour of sleep), the incidence of apnoea or hypopnoea over the entirety of the night is unchanged by the phase of the cycle.25 During the transition from wakefulness to sleep a decrease in central chemoreceptor drive occurs such that, at sleep onset, central apnoea is common in healthy subjects with a consequent rise in end tidal carbon dioxide (CO2) pressure of 0.3–1.1 kPa.26 The decrease in central chemoreceptor drive at sleep onset, as indicated by the incidence of central apnoea, and the rise in end tidal CO2 pressure are not influenced by hormonal fluctuations associated with the normal menstrual cycle.27 The hypoxic ventilatory response during sleep tends to be higher during the luteal phase of the menstrual cycle.28
Cardiovascular and haemodynamic changes associated with the menstrual cycle
Generally, the menstrual cycle is protective against cardiovascular disease. This is, however, primarily a result of blood composition which, as a result of high levels of serum oestradiol, tends towards lower levels of low density lipoproteins (LDL) and relatively higher levels of high density lipoproteins (HDL),29 both of which protect against atherosclerotic plaque formation in blood vessels. There is also some suggestion that oestradiol plays a role in attenuating the endothelial mediated vasoconstrictor responses to substances such as angiotensin, especially in such high concentrations as are present during pregnancy.30 ,31 Thus, haemodynamics have little effect in the premenopausal protection against cardiovascular disease. In healthy women at rest there are conflicting reports in the literature concerning the status of haemodynamics, particularly the daytime blood pressure at rest; however, most studies which have included measurement of serum hormone concentrations in the experimental protocol suggest that blood pressure at rest does not vary significantly over the course of the menstrual cycle in normotensive women.21 ,32-36
While blood pressure at rest appears uninfluenced by the stage of the menstrual cycle, in conditions of physical stress (cold stress and isometric exercise) blood pressure responses are potentiated during the luteal phase of the menstrual cycle.37 Furthermore, blood pressure responses to hyperoxic hypercapnia are significantly increased during the luteal phase of the cycle (fig 2).21 The influence of the cycle on blood pressure during hypercapnia is so strong that, in ovulatory cycles, the pressor response (defined as the increase in blood pressure for each kPa increase in end tidal CO2) is always higher during the luteal phase of the ovulatory cycle than it is during the follicular phase.21Since no influence of the phase of the menstrual cycle was shown on hypercapnic heart rate responses in this study, the predominant haemodynamic mechanism responsible for the potentiated hypercapnic pressor response during the luteal phase of the cycle is thought to be an increased peripheral vascular resistance response. Current literature suggests that the autonomic nervous system (and specifically the sympathetic nervous system) is predominantly responsible for the enhanced pressor response to physical stress. While the actual output of the sympathetic nervous system either remains unchanged or is slightly decreased by the presence of increased serum progesterone concentrations (both during the normal menstrual cycle38and in men receiving exogenous progesterone39), sympathetic responses (sweating, cardiovascular toxicity of cocaine) are enhanced in the presence of increased serum progesterone concentrations.38-40
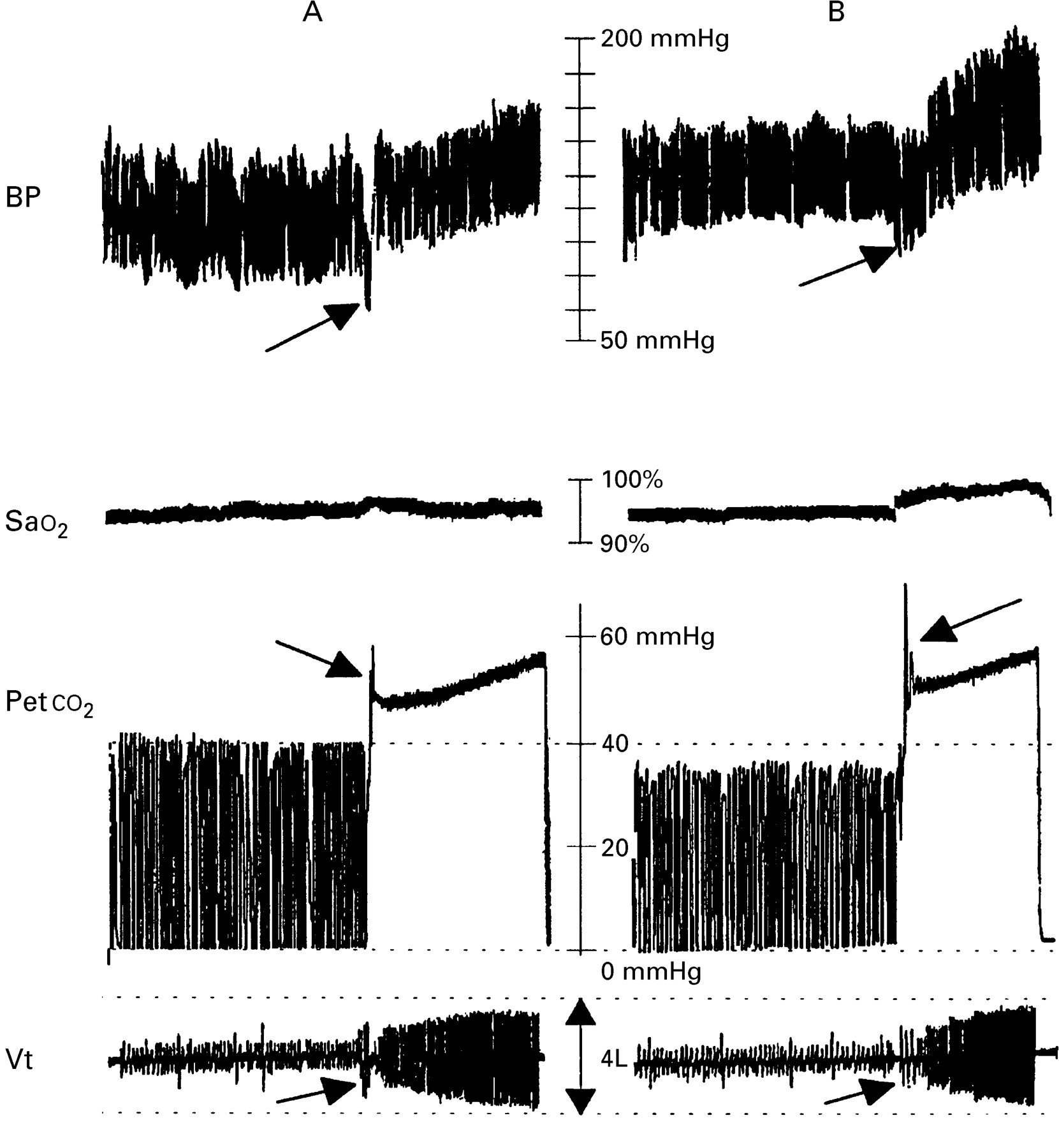
Cardiorespiratory responses to acute hyperoxic hypercapnia during (A) follicular and (B) luteal phase of the cycle. This study clearly shows an enhanced pressor response during the luteal phase of the menstrual cycle. The arrows on the figure indicate the beginning of hypercapnia after 5 min of normal tidal breathing.
While it is generally suggested that postmenopausal women have a significantly greater risk of developing OSA than premenopausal women, only one study has investigated the influence of hormone replacement therapy (HRT) on severity of obstructive apnoea in this population.41 A slight improvement in the severity of apnoea in REM sleep only was found after administration of HRT.
In premenopausal women with OSA there is no evidence of fluctuation in indices of severity of sleep disordered breathing (respiratory disturbance index (RDI), apnoea length and decrease in arterial oxyhaemoglobin saturation (Sao 2)) throughout the menstrual cycle during non-REM sleep.42During REM sleep a marginal improvement in RDI and decreases in Sao 2 have been reported during the luteal phase of the menstrual cycle.42 Increased central chemosensitivity associated with the luteal phase of the menstrual cycle is probably responsible for this observed improvement in OSA during this phase. Arousal resulting from respiratory events not meeting standard criteria as outlined by Rechtschaffen and Kales in 196843 (subcriterion events) were not analysed in this study. It may be that, because of increased chemosensitivity during the luteal phase of the menstrual cycle, arousal resulting from obstructive events during sleep may be hastened during the luteal phase as a result of increased sensitivity to blood gas fluctuations. As a result, the length of the obstructive events may not have met the standard criteria of more than 10 seconds to be counted as an obstructive apnoea or hypopnoea. However, considering that a large proportion of the haemodynamic response to obstructive events during sleep is associated with arousal and is independent of changes in blood gas tensions,44 these subcriterion events remain a significant risk factor when considering haemodynamic control during sleep apnoea.
Cardiovascular risk in premenopausal women
While the premenopausal status generally protects against cardiovascular disease, certain populations of women are excluded from this protection—for example, premenopausal diabetic women experience a considerably increased risk of cardiovascular morbidity and mortality compared with healthy premenopausal women. Recent surveys suggest that the incidence of death from cardiovascular disease in diabetic women aged 15–44 (most of whom will be premenopausal) is approximately 19 times that in healthy premenopausal women, while for the same age group in men the risk is approximately 12 times that of a comparable healthy population.45 Furthermore, the incidence of cardiovascular disease is similar in premenopausal diabetic women when compared with an age matched male diabetic population. However, in the age group 45–74 (which would include most perimenopausal or postmenopausal women) the risk of cardiovascular death as a ratio of the normal population is similar in men and women (twice the normal population in men and three times the normal population in women).45Thus, previous experience has identified at least one premenopausal group at significant risk of adverse cardiovascular events. Premenopausal women with OSA may be another unidentified subgroup of premenopausal women with a similarly increased risk of developing adverse cardiovascular events.
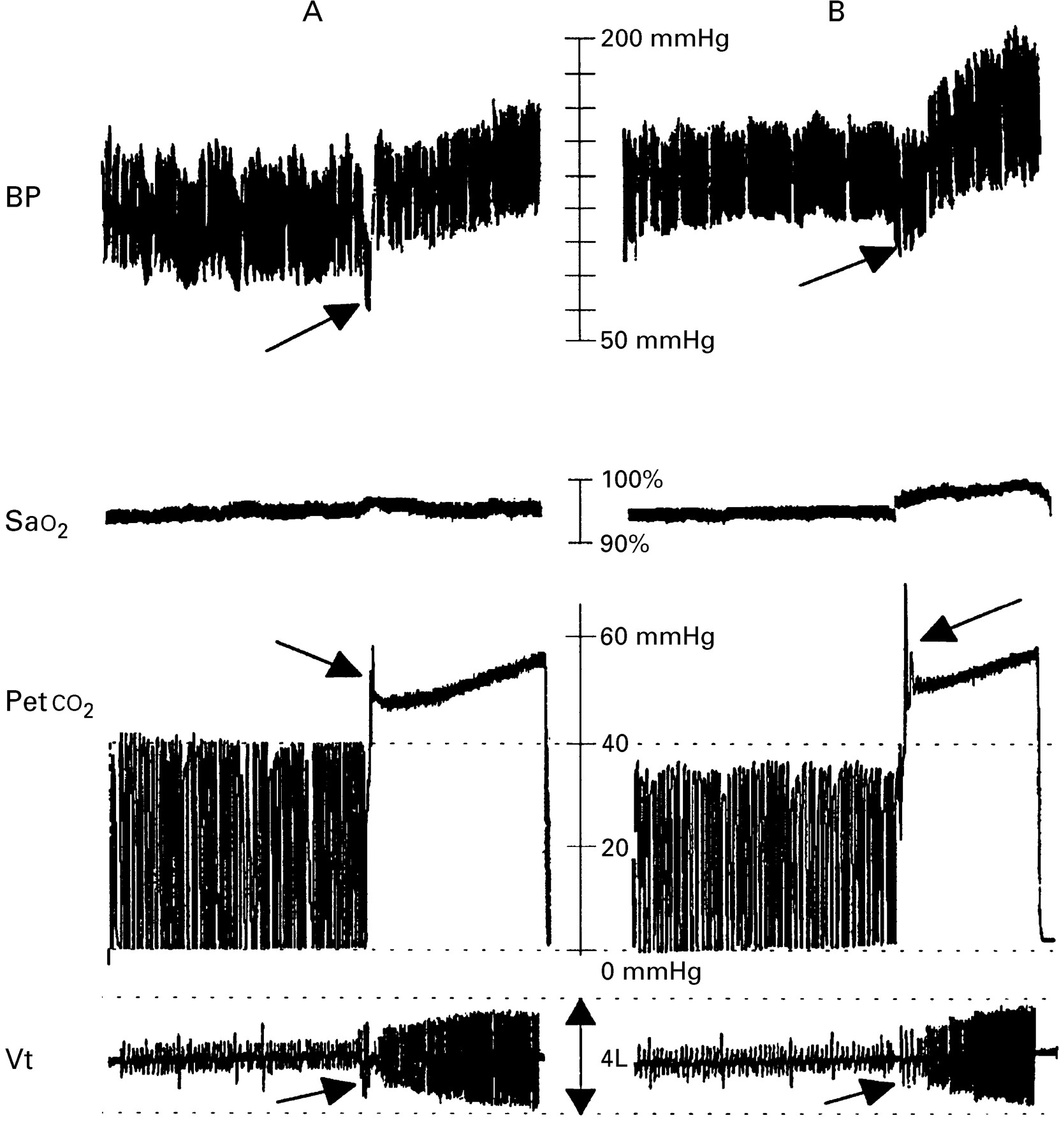
A recent investigation of haemodynamics during sleep in premenopausal women with apnoea has revealed that the blood pressure profile resulting from apnoea during sleep is similar in men and premenopausal women (fig 3), with a decrease in blood pressure towards the end of the apnoeic period and a surge in blood pressure during the hyperpnoeic phase following arousal. Furthermore, heart rate variability according to the stage of the apnoeic cycle (early apnoea, late apnoea, or hyperpnoeic phase) is similar in men and premenopausal women.42

Haemodynamic consequences of apnoea during sleep in (A) a man and (B) a woman. The haemodynamic responses to apnoea include a decrease in blood pressure and heart rate during the course of the apnoea termination followed by a surge in both during the hyperpnoeic phase following apnoea termination.
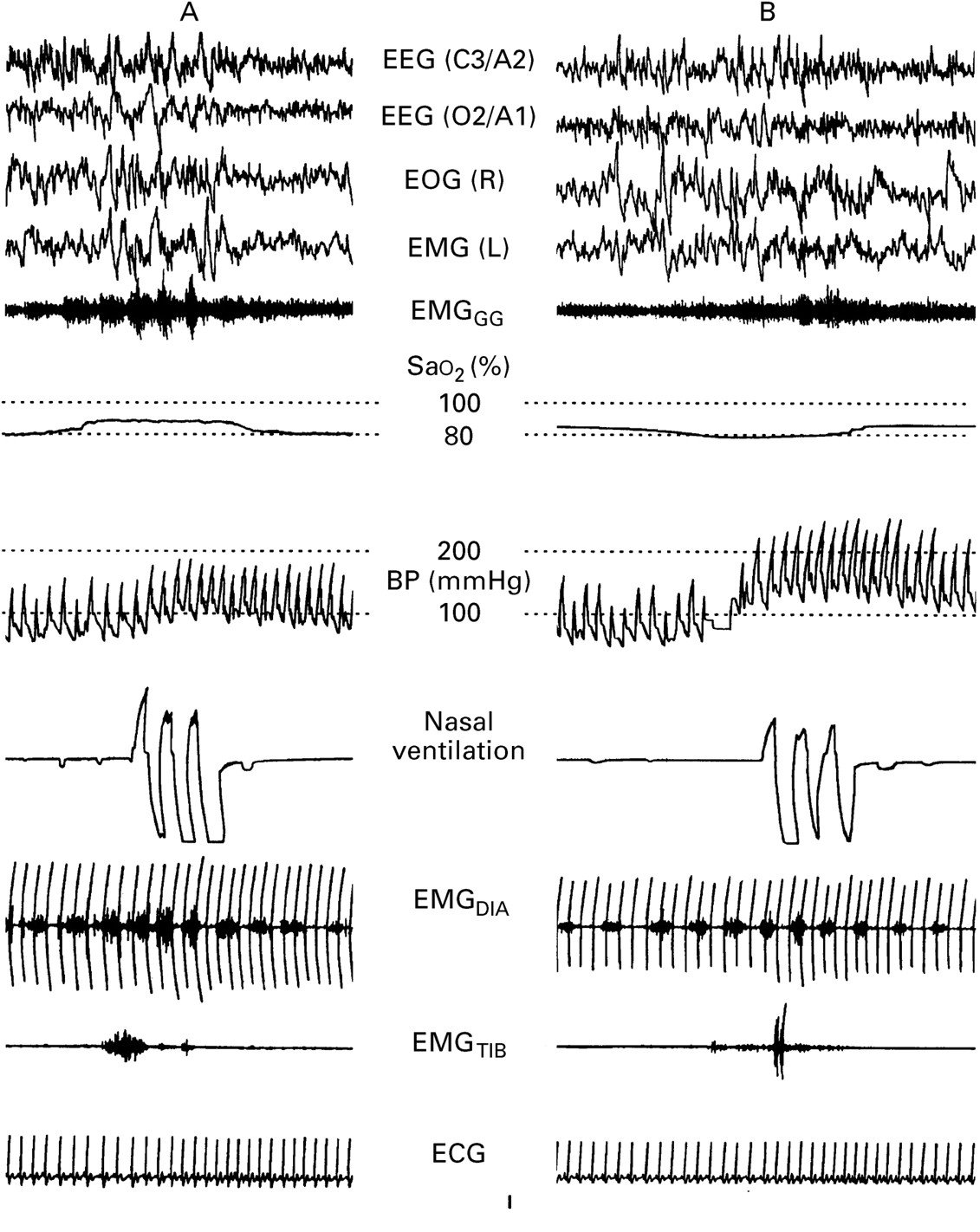
The increase in blood pressure from immediately before apnoea termination to the maximum blood pressure occurring during post-apnoea hyperventilation is significantly higher during the luteal phase of ovulatory menstrual cycles (fig 4). The increase in the magnitude of the pressor response during the luteal phase is particularly marked during REM sleep, being twice that occurring during the follicular phase.42

{kind=link}
{kind=link}
{kind=link}
{kind=link}
An example of apnoea occurring during (A) the follicular and (B) the luteal phases of the cycle in one subject. The figure shows a significantly potentiated increase in blood pressure following apnoea termination despite similar apnoea length, decrease in Sao 2 and level of arousal (as indicated by a similar duration of alpha in the EEG and similar magnitude of genioglossal EMG activity).
The haemodynamic responses to obstructive apnoeas during sleep are therefore similar in women to those previously reported in men. However, while there is a slight improvement in sleep disordered breathing during the luteal phase of the menstrual cycle, the haemodynamic consequences of apnoea are significantly amplified during this phase. The potentiated pressor response to obstructive apnoeas in sleep during the luteal phase of the menstrual cycle is most probably mediated by upregulation of peripheral catecholamine receptors.
In conclusion, while mortality data have not been reported specifically in premenopausal women with sleep disordered breathing, increased variability in blood pressure in men with OSA is thought to be associated with their increased cardiovascular risk (stroke, acute myocardial infarction and sudden cardiac death).5 Similar cardiovascular variability has been shown to occur in premenopausal women with OSA and, furthermore, this variability is accentuated during the luteal phase of the cycle. We therefore suggest that premenopausal status in these women may not protect against the cardiovascular risk known to accompany OSA in men, and that the existence of hormonal fluctuations associated with the menstrual cycle, far from being protective, may be a confounding factor in cardiovascular risk in this population.