Article Text

Abstract
Parasites of the genusMammomonogamus affect the respiratory tract of domestic mammals but have only rarely been reported in humans. In this case report the diagnosis of human syngamosis is described following bronchoscopic examination of a patient whose initial symptoms were simply of community acquired pneumonia. The patient had a persistent and productive cough with intermittent fever during 10 days of observation. After bronchoscopic extraction of the parasites and treatment with albendazole he recovered fully. This is one of the first recognised cases of human syngamosis in Korea.
- syngamosis
- pneumonia
Statistics from Altmetric.com
As has been described in other case reports,Mammomonogamus attacks mammals but has rarely been reported in humans. Leiper1 recorded the first case of human syngamosis in a patient who lived in St Lucia. Subsequent reports2 are few and most have originated from tropical areas of the world including South America and the Caribbean, as well as one case from the Philippines and one from Thailand.
We report a case of human syngamosis that was originally diagnosed as community acquired pneumonia. To our knowledge this is the first case in Korea and the second case to be reported in Eastern Asia.
Case report
A 61 year old Korean man presented with fever and malaise that had lasted for seven days. He produced 80–100 ml of purulent sputum daily. His symptoms had begun in Yeongil, Red China where he owned a restaurant. On his return to Korea he presented to our hospital. He had drunk some turtle blood, a traditional nutrient, five days before the onset of his symptoms. The lungs revealed bilateral rhonchi. At this time he had a normal blood chemistry profile, urinalysis, and stool examination. The white blood cell count was 15 400/mm3 with eosinophilia (20% of total leucocytes).
A chest radiograph taken on admission showed nodular and peribronchial streak density in the right middle and both lower lung fields. An HRCT scan showed multifocal and peribronchial infiltration. The mycoplasma antibody was positive (1:80). Roxithromycin was prescribed. Because productive cough with intermittent fever persisted, a bronchoscopic examination was performed 10 days later and revealed that the bronchi of both lower lobes and the bronchus of the right middle lobe contained many parasites. They could not be extracted easily because they attached themselves to the segmental and subsegmental bronchial walls (fig 1). With biopsy forceps and endobronchial suction many pairs of copulating parasites were aspirated.

Bronchoscopic findings in anterior basal segment of right lower lobe. The male is smaller and attached to the copulatory bursa of the female body, giving the characteristic Y-shaped appearance of Mammomonogamus laryngeus. The black arrow indicates the female parasite attached to the bronchial wall.
He has had no further complaints since the bronchoscopy and treatment with additional albendazole (400 mg) for three days.
Description of parasite
The worm is blood red to reddish-brown in colour because of haemophagia and has a typical Y-shaped appearance. The Y shape consists of two nematodes, with the female constituting the long reddish-brown arm and the shorter pale arm is the male worm which is attached to the side of the female worm. Under the microscope a formalin fixed parasite showed a cup shaped buccal capsule with several teeth at its base and no leaf crowns.
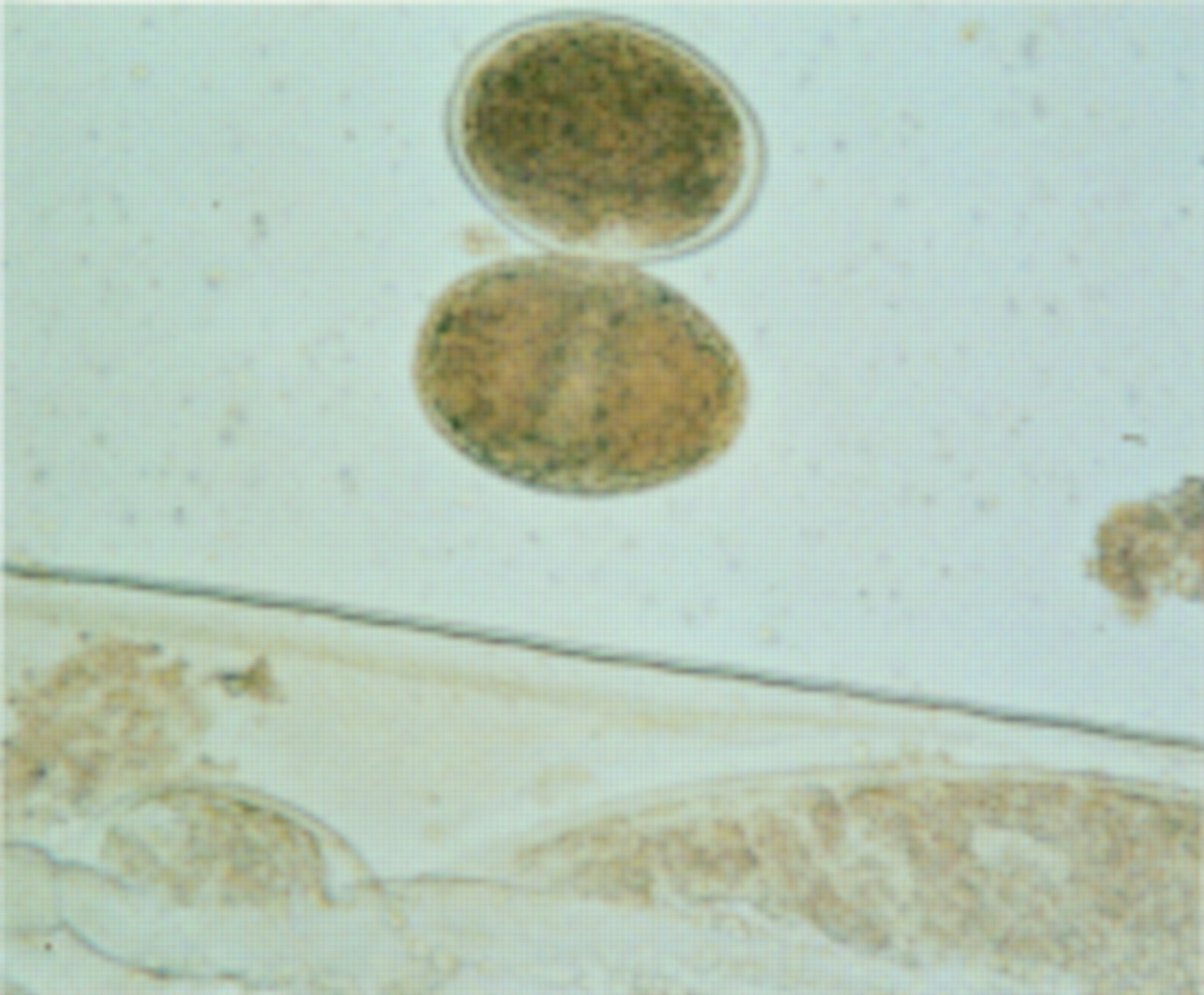
The female worms are 10.0 mm long and 380 μm wide with an intestinal uterus containing many eggs. The posterior end of the female is sharp and pointed and the short male bursa is folded into the female genital organ. The male worms are 3.5 mm long and 250 μm wide. Eggs are ellipsoid, non-operculated, measuring 40 × 80 μm (fig 2). It was identified as Mammomonogamus laryngeus.
{kind=link}
{kind=link}
Eggs are ovoid and non-operculated.
Discussion
The genus Mammomonogamus is a common parasite of domestic ruminants, particularly cattle and cats.3 Up to the present time only about 100 cases of human infection by this parasite have been reported in the medical literature.
There are two hypotheses concerning the life cycle ofM laryngeus in the human host. The first suggests that patients become infected by the adult.4Parasites migrate from the pharynx to the larynx and trachea, for unknown reasons, after ingestion of food or water contaminated by the intermediate host. This mode of transmission is suggested by the observation that the eggs of the parasite do not develop at body temperature in the patient’s trachea and by the estimation that symptoms begin to appear 6–11 days after contamination. The time required for the development of Syngamus trachea in the avian host from the infectious larval stage to the adult is known to be about three weeks.5 The alternative hypothesis is that the parasite has a pulmonary cycle (gastrointestinal tract/blood/lungs), with the trachea and bronchi being the preferred sites.6 ,7 Infected patients have commonly eaten food, possibly salad, vegetables or fruits, that has been contaminated with embryonated eggs, infective larvae or earthworms, snails, or slugs containing infective larvae. The larvae are released into the intestinal tract, then penetrate the intestinal wall and reach the alveoli within 24 hours . Within seven days the larvae become adult parasites and migrate to the upper bronchial tree where they copulate and produce eggs in approximately three weeks.6 ,8
The mode of infection is unclear in our patient. He had never travelled to areas where the other cases originated and had no contact with domestic mammals. As he developed symptoms five days after drinking uncooked turtle blood, we consider it is possible that he was infected by drinking the blood which contained the adult form of the parasite. Our patient was initially diagnosed as having community acquired pneumonia, probably because the parasites were in the segmental and subsegmental bronchi, which differed from other cases in whom the parasites were observed in the larynx,9 the posterior pharynx,2 and the tracheal wall.10
Syngamus infection is difficult to diagnose even when the organism produces symptoms. The diagnosis is usually made when the worms are expelled during a severe episode of coughing or are extracted by fibreoptic bronchoscopy.4
In our case we identified the adult copulating parasites by fibreoptic bronchoscopy. Removal of the parasites was enough to terminate the symptoms. Although there are no studies proving the effectiveness of antihelminthic drugs, they may be used to consolidate the cure.4 ,7