Article Text

Abstract
BACKGROUND The association between occupational quartz exposure and ventilatory function was investigated in men in a general population after adjusting for other potential determinants of outcome.
METHODS All eligible men aged 30–46 years living in western Norway (n = 45 380) were invited to a cross sectional community survey. This included a self administered questionnaire (with respiratory symptoms, smoking habits and occupational exposures), spirometric recordings (using dry wedge bellow spirometers), and a chest radiograph (65% attendance). Measurements of forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) were obtained in 91% (n = 26 803) of those who participated, 26 106 of whom performed successful spirometric tests and had normal chest radiographs and remained for further analysis. Age, body mass index, and technician standardised residuals ((observed minus predicted value)/residual standard error) of maximum FEV1/height2 and FVC/height2 were used as outcome variables for adjusted lung function levels, respectively.
RESULTS Occupational quartz exposure was reported by 13% (n = 3445) of those who participated in the survey, with a mean duration of seven years. Among those exposed to quartz, significant inverse linear relationships were observed between years of exposure and FEV1 level and the ratio of FEV1/FVC, independent of host characteristics. Multiple linear regression analyses showed that the difference in FEV1 associated with each year of quartz exposure was –4.3 ml (95% Cl –1.1 to –7.5 ml; p = 0.01) compared with –6.9 ml (95% Cl –4.7 to –9.1 ml; p<0.01) from smoking 20 cigarettes/day for one year after adjusting for age, atopy, asthma, wheezing, marital status, and other occupational exposures.
CONCLUSION In men aged 30–46 years with occupational quartz exposure and normal chest radiographs the duration of occupational quartz exposure was an independent predictor for spirometric airflow limitation.
- quartz
- occupational exposure
- smoking
Statistics from Altmetric.com
The area of western Norway consists mainly of mountains that are rich in quartz minerals with an average of up to 30% quartz in virgin rock.1 Crystalline silica is the most abundant element in quartz. In 1985 occupational quartz exposure was reported on self administered questionnaires by 9% of all men aged 30–49 years living in this area.2 The main industries with such exposure included construction work, sandblasting, tunnelling, road work, mining, and foundry work. Dust analyses from these work processes performed in similar Swedish industries showed that respirable dust had a mean fraction of free silica of 12–44%.3
Inhalation of large amounts of quartz dust may activate alveolar macrophages with release of proteolytic enzymes and destruction of alveolar walls resulting eventually in emphysema.4 From studies mainly among coal and gold miners there is also growing evidence of a causal association between moderate to high levels of quartz exposure and reduced level of forced expiratory volume in one second (FEV1) in the absence of radiological silicosis.5
Regulations have been introduced in Norway to protect and monitor workers exposed to silica.6 Since 1937 medical surveillance programmes have included chest radiographs every third year for such workers. The threshold limit for respirable (<5 μm) crystalline silica was introduced in Norway in 1978 and was set at 0.2 mg/m3.7 Despite the existing regulations in Norway and personal protection, occupational quartz exposure may still have a detrimental effect on lung function. Community based estimates are lacking of quantitative relationships between occupational quartz exposure and lung function.8 ,9
The objectives of the present survey of men aged 30–46 years with normal chest radiographs from the general population were to examine the ventilatory effects of occupational quartz exposure from about 1965 onwards and to identify possible susceptible subgroups.
Methods
This cross sectional community survey was performed in 35 neighbouring municipalities (Hordaland county and Sauda municipality) in western Norway. The 1990 census showed that the working population of men aged 30–45 years in this area was occupied in agriculture and fishing (4%), industry (35%), and private as well as public services (61%).10 Industrial occupations in men included mining and oil drilling (3%), foundry work (4%), tunnelling and road work (12%), construction work (15%), and other industrial work processes (66%).
The study population included all eligible men living in the study area on 1 January 1988 who were born between 1944 and 1958 (n = 45 380). They were invited to participate in a cross sectional survey which included a self administered questionnaire, height and weight measurements, as well as spirometric tests and chest radiography.11 A total of 29 611 subjects (65%) participated and spirometric recordings were obtained in 91% (n = 26 803), of whom 26 302 subjects obtained three acceptable and reproducible recordings with questionnaire data and chest radiographs that were included for analysis.
QUESTIONNAIRE
The self administered questionnaire elicited information on physician diagnoses, respiratory symptoms, smoking habits, and occupational exposures to quartz and other dusts or gases as well as three different work processes (foundry, tunnelling and rock drilling).11 History of asthma was defined as having a physician’s diagnosis of asthma. Atopy was defined as having a history of hay fever or a physician’s diagnosis of atopic dermatitis. Wheezing was defined as ever having wheezing in the chest.
Never smokers were men who never had smoked daily and ex-smokers included those who had stopped smoking prior to the survey. In current smokers the quantitative effect of cigarette smoking was measured in pack-years.12 This was calculated by multiplying the duration of smoking (in years) by the average number of cigarettes smoked daily divided by 20. Ex-smokers and other smokers (pipe or cigar smokers) were included in the multivariate analyses as separate dummy variables (1 = yes, 0 = no). Outcome in the reference category (never smokers) was therefore defined when all the variables of smoking were 0.
The English translation of the question on occupational quartz exposure was: “At work have you ever been exposed to quartz dust or stone dust with quartz?” The alternative answers were “Yes”, “No” or “Don’t know”. If “Yes”, then state: “How many years altogether have you been exposed to such dust at work” (number of years).
SPIROMETRIC TESTS
Forced expirations were recorded using three dry wedge spirometers (Vitalograph S-model).11 Each subject performed up to eight repeated measurements until three acceptable forced expiration manoeuvres were obtained with the two highest values of forced vital capacity (FVC) reproducible within 300 ml.13 All FEV1 and FVC values were corrected to body temperature and pressure saturated conditions (BTPS) by twice daily recordings of room temperature and barometric pressure.
Maximum values of FEV1 and FVC were divided by height squared, respectively, to obtain homoscedasticity in between subject variability of lung function levels. This was necessary to get unbiased estimates of ventilatory function. Predicted maximum values for FEV1/height2 and FVC/height2, respectively, were calculated using linear regression models with age and body mass index (BMI) of the subjects as well as the technician status as explanatory variables in reference subjects from this survey. These included healthy asymptomatic never smokers without occupational quartz exposure (n = 3027). For FEV1/height2(l/m2) the regression coefficients were: –0.0067/year for age, 0.0111 for BMI of 22–25.9 kg/m2, –0.0140 for BMI of 26–29.9 kg/m2, and –0.0478 for BMI of ⩾30 kg/m2 and –0.0140 for temporary versus permanent technicians. The equation had a constant of 1.6268 and a residual standard error (RSE) of 0.1529. For FVC/height2(l/m2) the corresponding coefficients were –0.0069, 0.0263, –0.0100, –0.0697, –0.0151 and 1.9553, respectively, and the equation had an RSE of 0.1828. Standardised residuals of maximum FEV1/height2 (SFEV1/h2) and FVC/height2 (SFVC/height2) were calculated by dividing the residual (observed minus predicted) by the RSE for each variable and used as dimensionless outcome variables for FEV1 and FVC levels, respectively.
CHEST RADIOGRAPHY
Chest radiographs with posteroanterior view (10 ×10 cm) were carried out using a Siemens X-ray generator Polyphos 30 M combined with an image intensifier RBV 57 with a Canon Camera ZXI-100. All radiographs were analysed through a magnifier that yielded 25% enlargement. Each film was read twice in a random order by two independent experienced radiologists and again by a third reader if any abnormality was observed by at least one reader.14 All three readers were unaware of the exposure data or clinical status of the subjects to which the films belonged.
ANALYSIS OF DATA
All analyses were performed using the BMDP package.15Unpaired t tests were used to compare mean values. Differences between prevalences were tested by chi-square tests. Comparison of mean values adjusted for covariables was performed by one way analyses of covariance. Test for trend was performed by linear regression analysis. A significance level of p = 0.05 (two tailed) was used in all analyses.
Multiple linear regression analysis was used in selecting factors important for prediction of lung function level. Categorical variables were introduced into the equation using dummy variable technique. A full model was fitted that included occupational quartz exposure and all other potential determinants of outcome. The presence of possible susceptible subgroups were analysed by studying modification in the additive model. The following variables were considered as potential modifiers: history of asthma, atopy, wheezing, marital status, and smoking, as well as occupational airborne exposures other than quartz. Marital status was included in the model as a marker of socioeconomic status.16 Age was added in the full model since age and duration of quartz exposure were weakly correlated (correlation coefficient 0.18; p<0.001).17 With all the potential confounders in the model, modification of the effect of quartz was studied by introducing covariate-exposure product terms one by one and retaining them in the final model according to the statistical significance of the regression coefficients (p<0.05).
Results
Of the 26 302 subjects with successful spirometric tests and questionnaire data 196 (0.8%) were excluded because of pathological changes on their chest radiographs (presence of calcifications, pleural or interstitial changes, changes in heart configuration or big vessels, anomalies or other findings) leaving the remaining 26 106 subjects for further analyses (table 1). Of these, 23 001 (88%) answered the question on exposure to quartz; 3425 (13%) answered “yes”, 12 727 (49%) answered “no”, and 6849 (26%) answered “don’t know”. The work processes in which exposure to quartz was reported were foundry work only (14%), rock drilling only (12%), tunnelling only (5%), two of these (23%), three of these (10%), and unspecified (36%).
Self reported occupational quartz exposure and duration by different host variables and standardised residuals of FEV1/height2(SFEV1/h2) and FVC/height2(SFVC/h2) in men aged 30–46 years with normal chest radiographs participating in a cross sectional survey in 35 municipalities in South West Norway (n=26 106)
Subjects exposed to quartz (13%) had a mean (SD) duration of exposure of 7.1 (6.2) years. Table 1 shows the distribution of host variables and lung function levels in the different exposure groups. Height was identical in all groups (mean 1.79 (0.06) m), but those exposed to quartz were 1.4 kg heavier (80.3 (11.7) kg; p<0.01) than subjects answering “no” or “don’t know” (78.9 (11.0) kg). Those exposed for ⩾15 years were about two years older (p<0.01) than the others. The prevalence for each variable of a history of asthma, atopy and wheezing was higher (p<0.05) among subjects exposed to quartz than in those not exposed, whereas no difference was observed in the prevalence of single marital status in the two groups. The proportion of current smokers was higher (p<0.01) in those exposed compared with those not exposed and cigarette consumption increased with duration of exposure (table 1).
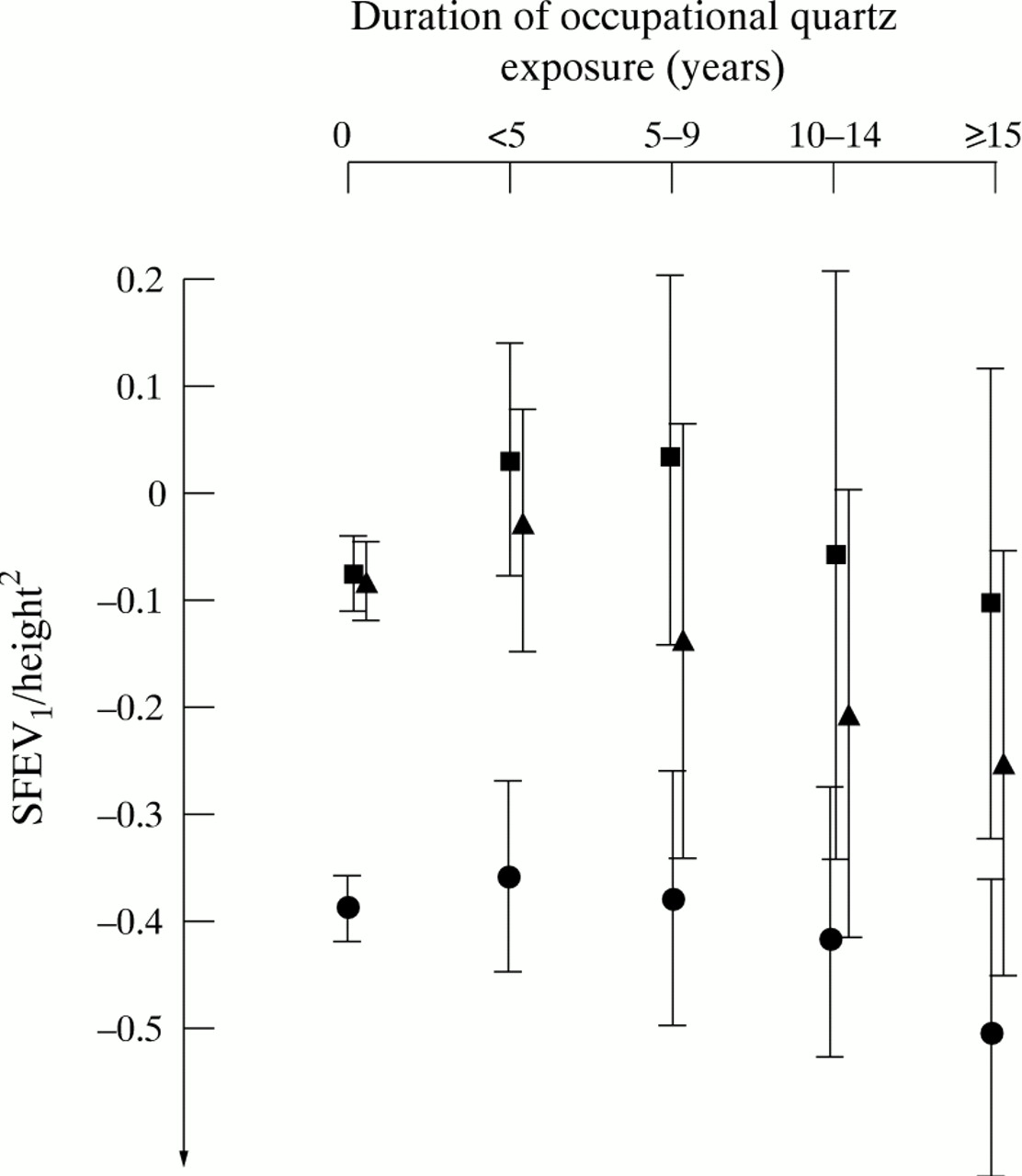
Crude values of SFVC/h2 and SFEV1/h2 were higher in those exposed for less than five years than in those not exposed, but decreased thereafter with duration of exposure (table 1). Although the crude FVC level was higher (p = 0.01) in all men exposed to quartz (mean SFVC/h2 –0.031 (1.000)) than in those not exposed (mean SFVC/h2 –0.081 (1.016)), the crude FEV1 level was lower (p = 0.01) in the former group (mean SFEV1/h2 –0.247 (1.052)) than in the latter group (mean SFEV1/h2 –0.195 (1.055), table 1). After adjusting for age and smoking, this difference in FVC increased, whereas the difference in FEV1 disappeared. Among those exposed the observed inverse relationship remained after adjusting for age and smoking using one way analysis of covariance, being more marked for FEV1 than for FVC (fig 1). Similar associations were also observed within each smoking category for FEV1 (fig 2) and for FVC in ex-smokers and current smokers.

Age, body mass index, and technician adjusted standardised residuals (mean, 95% confidence intervals) of maximum FEV1/height2(SFEV1/height2) and FVC/height2(SFVC/height2) in men aged 30–46 years by number of years with occupational quartz exposure adjusted for age and pack years in cigarette smokers as well as dummy variables for ex-smokers and other smokers using one way analysis of covariance (n = 15 173).

Age, body mass index, and technician standardised residuals (mean, 95% confidence intervals) of maximum FEV1/height2(SFEV1/height2) in men aged 30–46 years by number of years with occupational quartz exposure in different smoking groups: never smokers (squares) (n = 5154); ex-smokers (triangles) (n = 3736), and current smokers (circles) (n = 6359).
After adjusting for smoking, subjects exposed to quartz for 1–2 years had significantly higher adjusted lung function levels (mean differences in FEV1 of 42 ml (p<0.05) and FVC of 68 ml (p<0.01) for a man of height 1.8 m) than in those not exposed. In subjects exposed for less than five years the adjusted FEV1level decreased from those exposed for 1–2 years (n = 795) to those exposed for 3–4 years (n = 413) with the mean SFEV1/h2 being –0.153 (1.015) and –0.225 (1.016), respectively, although these levels were not statistically different (p = 0.2).
The ratio of FEV1/FVC was slightly lower among subjects exposed to quartz than in those not exposed, being 79.1% versus 79.6% (p<0.001), respectively, after adjusting for age and smoking using one way analysis of covariance. Among those exposed this adjusted ratio decreased gradually from 79.3% in subjects exposed for less than five years to 78.6% in those exposed for ⩾15 years (test for trend p<0.01), with the effect of quartz exposure not being significantly different between the smoking categories.
Multiple linear regression analysis among subjects exposed to quartz showed that both SFEV1/h2 and SFVC1/h2 were dependent on smoking, whereas only SFEV1/h2 was dependent on duration of quartz exposure after adjusting for age, atopy, asthma, wheezing, marital status, and other occupational exposures (table 2). Based on the regression coefficient for pack years (–0.0139) and the RSE (0.1529) in a man of height 1.8 m, this corresponded to a reduction in FEV1 level of 0.0069 (–0.0139 × 0.1529 × (1.8)2) litres when smoking 20 cigarettes/day for one year. Similarly, FEV1 decreased by 0.0043 litres (p = 0.01) for each year exposed to quartz after adjusting for the other covariables in table 2. The corresponding reduction in FVC level due to smoking was 0.0047 litres (p<0.01). Years of quartz exposure squared did not add significantly to the models in table 2. Age squared added significantly to the models (p<0.05 for SFEV1/h2 and p<0.01 for SFVC1/h2) but did not change the effects from years of quartz exposure in table 2.
Estimated multiple linear regression models for adjusted 2-150SFEV1/h2 and SFVC/h2, respectively, in quartz exposed subjects (n=25422-151)
Subjects with a history of asthma and wheezing had a significantly (p<0.01) lower adjusted FEV1 than those without, with a difference of 351 ml and 148 ml, respectively (table 2). The adjusted FEV1 was 85 ml lower (p<0.01) in single men than in married/divorced men after adjusting for the other covariables in table 2. Introduction of interaction terms between years of quartz exposure (as a continuous variable) and age, asthma, atopy, wheezing, marital status, smoking, and other occupational exposures into the models one by one showed that none of these was a significant modifier of the effect of quartz exposure on adjusted FEV1 and FVC levels, respectively (table 2).
When the 798 subjects with a history of asthma and/or wheezing were excluded from the models in table 2, the effects of years of quartz exposure on adjusted FEV1 and FVC levels remained basically unchanged. In never smokers only (n = 537) the regression coefficients for years of quartz exposure on FEV1 and FVC levels were –0.0132 (95% CI –0.0273 to –0.0009) and –0.0030 (95% CI –0.0175 to 0.0115), respectively.
When subjects involved in foundry work or tunnelling were excluded from the models in table 2, the relationships between duration of quartz exposure and adjusted FEV1 and FVC levels remained unchanged. However, when all subjects who had worked in rock drilling (n = 1135) were excluded, the effect of duration of quartz exposure on FEV1 was reduced by 48% in the remaining 1407 subjects (regression coefficient –0.0045 (95% CI –0.0129 to 0.0039)).
Mean FEV1 levels in subjects exposed to quartz by different work processes are shown in fig 3 after adjusting for age and smoking using one way analysis of covariance. Among subjects exposed to only one work process, significantly lower FEV1 values were observed in rock drillers than in foundry workers (p<0.05).

{kind=link}
{kind=link}
{kind=link}
Age, body mass index, and technician standardised residuals (mean, 95% confidence intervals) of maximum FEV1/height2(SFEV1/height2) in men aged 30–46 years exposed to quartz in foundry work, tunnelling and rock drilling only adjusted for age and pack years in cigarette smokers as well as dummy variables for ex-smokers and other smokers using one way analysis of covariance (n = 1070).
Discussion
In men aged 30–46 years with occupational exposure to quartz and normal chest radiographs significant inverse linear relationships were observed between duration of occupational quartz exposure and the FEV1 level and the ratio FEV1/FVC, independent of host characteristics. Consequently, in these young adult men without any radiological abnormalities we observed an obstructive type of lung function impairment which could be attributed to quartz exposure.
The validity of the observed relationship between quartz exposure and adjusted lung function may have been biased by several factors. Firstly, selection bias may have affected our results. Previous analyses, however, have shown that the participants in this cross sectional survey had similar demographic characteristics, smoking habits, and respiratory symptoms to all men aged 30–45 years from the general population in Norway.11 On the other hand, health selection could explain the significantly higher adjusted FVC level observed in subjects exposed (and in particular those exposed for 1–2 years) compared with that seen in the non-exposed subjects. This supports previous observations that those who enter dusty professions have better lung function than those who do not (primary health selection).18 This is supported in the present paper by the fact that the exposed group consisted of more smokers than the non-exposed group. Nevertheless, we demonstrated an inverse dose response relationship within those exposed with duration of exposure. Thus, the observed effect from duration of quartz exposure on adjusted lung function level was probably an underestimate of the true effect since health selection also tends to make susceptible subjects leave dusty occupations at an earlier stage than healthy workers (secondary health selection), thereby underestimating the true effect of the exposure.17
Altogether 0.8% of the participants in our study were excluded due to abnormalities detected on the small size radiographs. Theoretically, false negative radiographs with regard to silicosis could have been included in our analysis. However, this would tend to strengthen the observed association between duration of quartz exposure and spirometric airflow limitation as these potential subjects would probably have a more restrictive pattern of lung function impairment.9
Secondly, the presence of any recall bias in our survey was minimised when the self administered questionnaire was answered at home prior to participation in the survey and with the spirometric technician unaware of the answers given. The relationship between exposure and reduced lung function may have been biased towards a falsely high value if subjects with reduced lung function tended to recall any exposure better than subjects with normal lung function or, as we observed, that subjects with quartz exposure reported more respiratory symptoms than non-exposed subjects. However, the relationship between duration of quartz exposure and reduced FEV1 remained significant after excluding those reporting a history of asthma and/or wheezing. Although self administered questionnaires are widely used in occupational exposure assessments in general populations, measurement errors and misclassification may occur,19 though not always.20 Previous studies have found the misclassification to be non-differential, making it more difficult to detect any relationship between exposure and outcome.21This is further strengthened in our survey since the outcome variable was based only on objective spirometric measurements. The validity of an identical question to that used in our survey on occupational quartz exposure has in a previous cross sectional community study in the same area shown a high specificity (98%) and a low sensitivity (36%).2 For a given exposure with a low prevalence, a high specificity has a greater effect on the estimated outcome variable than a high sensitivity.22 The optimal quantitative exposure assessment should include indices of both level and duration of exposure. Our quantitative assessment of quartz exposure, however, included only duration of exposure (in years) with a high probability of misclassification. Furthermore, duration of exposure was missing in 24% of the exposed subjects. It is also likely that individuals in our survey exposed for many years may have had very low exposures. In the previous general population survey in the same area as ours 63% of those exposed regarded their quartz exposure to be low.2
Thirdly, we have no information on the exposure status in the subjects with missing information (12%) on quartz and in those answering “don’t know” (26%). Subjects in these two groups had similar personal characteristics to those not exposed (table 1). Given that the subjects in the former two groups would be included in the non-exposed group, this would not alter the observed effect within the exposed group.
Fourthly, duration of quartz exposure could also be a surrogate indicator of other correlated mixed occupational exposures such as other mineral dusts, gases, vapours and fumes.23 Most studies on occupational quartz exposure have been done in miners, quarrymen and foundry workers where free silica usually comprises less than half of the total respirable dust exposure.24 Such workers are also exposed to a mixture of occupational contaminates including nitrous gases and diesel exhaust emissions, although previous studies have shown that the effects of free silica usually predominated.25 Subjects exposed for a longer period of time could also be fundamentally different (more heavily exposed or exposed to more agents or different work processes) from those exposed for a shorter period. Consistent with this we observed that subjects exposed for 10 years or more had higher prevalences of two or more work processes (foundry, tunnelling and rock drilling) than those exposed for less than 10 years, being 60% and 46%, respectively (p<0.01). In a 23 year community follow up study of men initially aged 22–54 years living in the same area as the subjects in the present study we have previously observed that occupational quartz exposure and 10 other occupational agents were highly associated with each other.23 It would therefore be difficult to identify the effects from individual agents. To reduce the influence of possible correlated exposures in our survey we observed, in the small number of rock drillers only (n = 312), that the effect of years of quartz exposure on FEV1 remained (regression coefficient –0.0100 (95% CI –0.0333 to 0.0133)), although it did not reach statistical significance in the small number of subjects. In future studies the precision and validity of the exposure characterisation may be improved by asking subjects about participation in work processes in which specific agents may be involved, as well as asking them about the agents themselves.26
The classification of smoking in this survey was based on self reported information from a standardised questionnaire. A previous general population study in the same area showed good agreement between self reported smoking habits and venous carboxyhemoglobin levels.27 The use of pack years instead of a qualitative classification of exposure (light, medium and heavy) in current smokers was chosen to give a more precise quantification of the cumulative burden on ventilatory function from daily cigarette smoking as well as the duration of smoking. Ex-smokers were analysed in a separate group since we lacked information on time from smoking cessation.12 Using a qualitative classification in smokers instead of pack years in the multivariate analysis did not alter our observed relationships. Residual confounding by smoking could have affected the relationship between duration of occupational quartz exposure and adjusted FEV1 level. However, a similar effect was also observed in never smokers (although the effect failed to reach the 5% level of statistical significance), which indicated that residual confounding by smoking could not explain this relationship.
Adding age to the final models in table 2 could possibly result in overcorrection of the covariables since the outcome variables were already age adjusted. Despite this, a significant effect was still observed between years of quartz exposure and FEV1reduction. The alternative of no adjustment of age in table 2 would be worse since it could be argued that we had not sufficiently adjusted for differences in age in the different groups.
In agreement with previous community studies we observed that the prevalence of daily cigarette consumption increased from those without occupational exposure to those exposed.28 ,29 Our observed adjusted effect from cigarette consumption on FEV1 (6.9 ml/pack year) was almost identical to that observed in men from previous cross sectional studies in Norway, Canada, South Africa and USA, being 6.5,30 7.0,12 ,31 and 7.432 ml/pack year, respectively.
Several studies among coal,33 gold,4 and hard rock miners,34 as well as granite35 and pottery workers36 have found a significant association between occupational quartz exposure and spirometric airflow limitation. These observations have been performed in men aged ⩾45 years and with ⩾20 years of high exposure levels. However, limited community based information is available on the association between occupational quartz exposure and FEV1 status. In a general population our findings are in agreement with previous studies where occupational quartz exposure was related to reduced level of FEV1 26 ,28 and accelerated decline in FEV1.23 The average age of the men in these studies, however, was 15–25 years older than that in our present survey.
The adjusted annual difference in FEV1 associated with each year of quartz exposure observed in the present survey (approximately 4 ml/year) was less than that observed in South African gold miners (approximately 9 ml/year)4 ,31 and British coal miners (approximately 7 ml/year).33 These miners were on average about 15 years older, had higher dust exposures (mean respirable crystalline silica concentrations of approximately 0.3 mg/m3), and had ⩾15 years longer duration of exposure than our subjects. In agreement with previous cross sectional studies33 we did not find evidence that smoking potentiated the effects from quartz exposure, as reported in a Swedish follow up study35 and in South African gold miners,37 nor did we observe any of the other host variables (history of asthma, atopy, wheezing or marital status) to be significant modifiers on the effects from occupational quartz exposure on lung function level.
In this large cross sectional community survey of men aged 30–46 years with normal chest radiographs an inverse relationship was observed between duration of quartz exposure and spirometric airflow limitation, independent of host characteristics. Despite existing regulations up to 1989 against occupational quartz exposure in Norway, we observed that such exposures are associated with an increased risk of developing chronic obstructive pulmonary disease. In 1989 the threshold limit value for respirable crystalline silica was further reduced to 0.1 mg/m3. Standardised pulmonary function testing should, however, also in the future be part of the medical surveillance of workers exposed to quartz. This should be done prior to employment and at regular intervals thereafter.38 Further studies should be performed to improve the exposure characterisation from quartz in different work processes including rock drillers and to learn about the underlying toxicological mechanisms. Preventive strategies including better public awareness of the hazards and better technology to control silica dust should be taken to give workers better protection from quartz exposure.9
Acknowledgments
The authors acknowledge the staff at the National Health Screening Service for data collection and making the data file. This survey was supported by grants from the Research Council of Norway and Confederation of Norwegian Business and Industry.