Article Text

Abstract
Bronchiectasis developing following colectomy for ulcerative colitis has been reported in a few cases. This may be the first report of bronchiectasis developing after colectomy for Crohn’s disease. The close temporal relationship to colectomy, lack of bacterial pathogens in the sputum, and an impressive response to oral steroids suggest a difference in pathogenesis from idiopathic bronchiectasis.
- bronchiectasis
- Crohn’s disease
- colectomy
Statistics from Altmetric.com
There is a well recognised association between inflammatory bowel disease and bronchiectasis.1-3 The development of bronchiectasis after colectomy has been described in ulcerative colitis.1-3 We present what may be the first reported case of bronchiectasis developing shortly after colectomy in Crohn’s disease.
Case report
A 30 year old woman with a 16 year history of inflammatory bowel disease, initially judged to be ulcerative colitis, underwent total colectomy and ileostomy in June 1994 and anorectal excision in August 1995. Histological appearances were diagnostic of Crohn’s disease with deep fissure-like ulcers extending into the submucosa and muscularis propria, transmural inflammation, and granulomas in the submucosa and regional lymph nodes. A diagnosis of Crohn’s disease was further supported clinically by the subsequent development of a vaginal fistula. Three months after colectomy she developed a severe cough productive of a quarter cup of purulent sputum daily requiring hospital admission in November 1994. In June 1995 computed tomographic (CT) scanning demonstrated marked bronchial wall thickening with widespread extensive bilateral cylindrical bronchiectasis of mild to moderate severity (fig 1B). No bronchiectasis had been seen on sections through the lower lobes from a CT scan of the abdomen performed two months after colectomy (fig 1A).

(A) CT section through lower lobes two months after colectomy showing no evidence of bronchiectasis. (B) CT section through lower lobes one year after colectomy showing unequivocal bronchiectasis with prominent bronchial wall thickening.
She had no previous respiratory symptoms and normal chest radiographic appearances. There was no history of asthma, pneumonia, significant respiratory illness in early childhood, hay fever, excema, rhinosinusitis, or significant gastro-oesophageal reflux. She had never smoked. There were no other extraintestinal manifestations of Crohn’s disease and she denied symptoms suggestive of collagen vascular disease. Intermittent medications have included inhaled steroids, mesalazine, antibiotics, and oral corticosteroids. There were no abnormalities on general or respiratory examination. Liver function tests and autoantibodies were normal apart from a smooth muscle titre of 160. The immunoglobulin profile, including immunoglobulin G subclasses, was normal. Aspergillus serology and skin prick tests to Aspergillus fumigatus were negative. A sweat test was normal. Repeated sputum cultures grew no respiratory pathogens and were negative for acid fast bacilli. The cell type was neutrophils. Spirometric and plethysmographic volumes were normal, as was gas transfer factor, but the expiratory limb of the flow-volume curve showed a moderate reduction in airflow at low lung volumes. Bronchofibroscopy demonstrated severe generalised mucosal inflammation and purulent secretions.
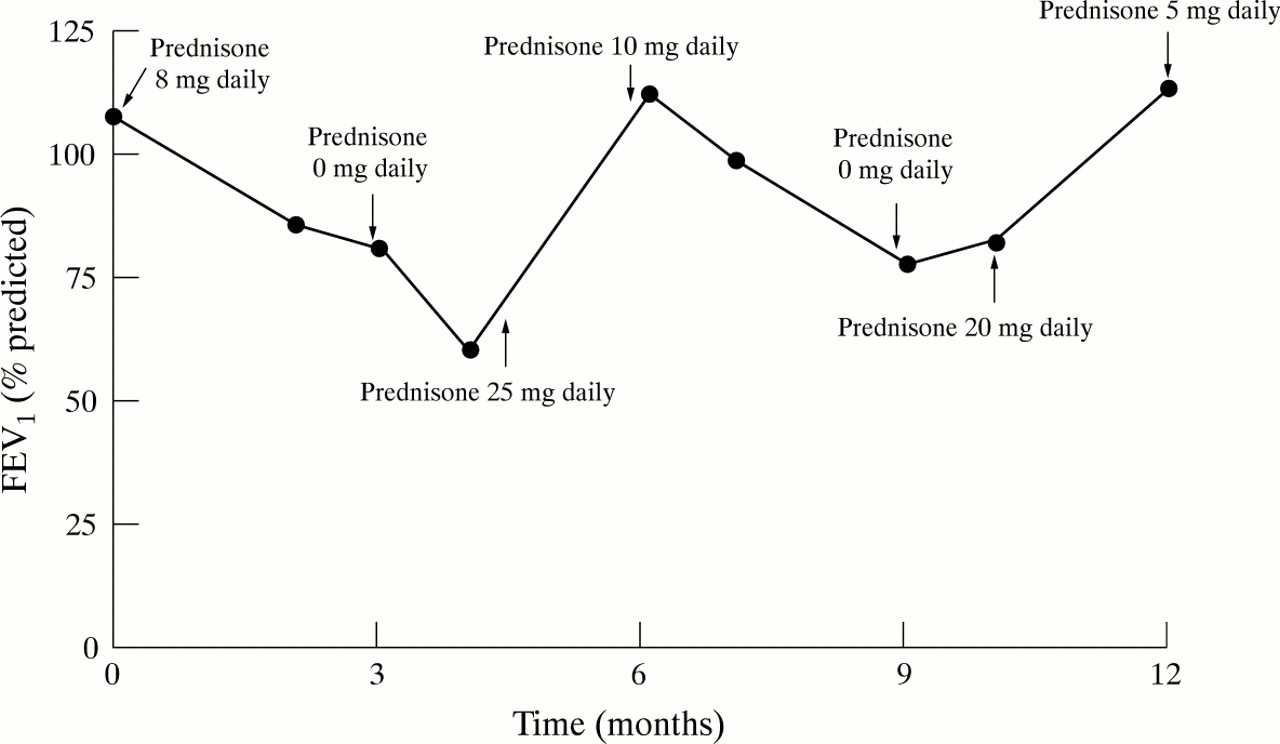
Despite regular postural drainage, high doses of inhaled corticosteroids (budesonide via Turbohaler 1600 μg twice daily), and broad spectrum antibacterial therapy, she required readmission in February 1996. She continued to produce half a cup of green sputum daily with no respiratory pathogens on multiple sputum cultures. She did not respond to intensive physiotherapy and intravenous antibacterial therapy (including cefuroxime, metronidazole, ceftazidine and gentamicin), but with the introduction of oral corticosteroids a large reduction in sputum and an increase in percentage predicted FEV1 from 60% to 113% was observed. Despite compliance with high dose inhaled corticosteroids she has shown a consistent requirement for oral steroids (fig 2) but remains well with minimal sputum production and normal lung volumes on a small maintenance dose of oral corticosteroids. Repeat CT scanning with expiratory sections in October 1996 showed unequivocal—albeit partial—regression of bronchial wall thickness with no change in the diffuse extent of bronchiectasis.
{kind=link}
{kind=link}
Serial measurement of FEV1 in relation to oral corticosteroid therapy. Airflow obstruction increased markedly on two occasions when therapy was withdrawn. Prompt improvement was noted with reinstitution of therapy.
Discussion
We believe this to be the first report of bronchiectasis developing within a year of colectomy in a patient with Crohn’s disease. There is a well recognised, albeit rare, association between bronchiectasis and inflammatory bowel disease. Kraft et alreviewed 1400 patients with inflammatory bowel disease for respiratory symptoms over a 40 year period and found only six cases of bronchopulmonary pathology, consisting of five patients with ulcerative colitis and a single patient with Crohn’s disease (who had chronic bronchitis but not bronchiectasis).1 Neilly et al performed a detailed respiratory assessment of 29 patients with Crohn’s disease relative to a control group matched for age, sex, and smoking.4 No patient had chronic sputum production or overt bronchiectasis and lung function indices were essentially normal.
A recent review of the literature included 33 well detailed cases with inflammatory bowel disease and pulmonary manifestations.3The five patients with Crohn’s disease had airways obstruction, chronic bronchitis or cryptogenic organising pneumonia, but not bronchiectasis. Bronchiectasis was seen in six of the 28 patients with ulcerative colitis, including three who developed severe bronchopulmonary suppuration a few days or weeks after colectomy. Butland et al had previously described unexplained chronic bronchial suppuration in seven patients with ulcerative colitis, including three with rapidly progressive bronchiectasis developing within a year of colectomy.2
The absence of a documented association between bronchiectasis and Crohn’s disease does imply rarity and raises the possibility of a chance association. However, strong circumstantial support for a real association include a clear temporal relationship to colectomy and, unlike idiopathic bronchiectasis, a repeated failure to identify bacterial pathogens and an impressive response to oral corticosteroids. The diffuse nature of the inflammatory process, seen both at bronchoscopy and on CT scans, is also compatible with a link to inflammatory bowel disease.
Chronic bronchial suppuration developed within months of colectomy and within a year bilateral bronchiectasis had developed de novo, as judged by serial CT appearances. Failure to isolate bacterial pathogens on repeated sputum culture and a need for oral corticosteroid therapy are both reported features of bronchiectasis associated with ulcerative colitis,2 ,3 in contrast to idiopathic bronchiectasis. This suggests that the pathogenesis of bronchiectasis in inflammatory bowel disease may be primarily autoimmune and that infection does not play as prominent a role as in the genesis of idiopathic bronchiectasis by the “vicious circle” mechanism.5 ,6 It has been suggested that, following colectomy, the bronchial tree (which has the same embryological origin as the bowel) becomes the new epitopic target for the immune system.7
In conclusion, we believe that this case demonstrates what may be the first report of bronchiectasis developing after colectomy for Crohn’s disease. The close temporal relationship to colectomy, failure to identify bacterial pathogens, and an impressive response to oral steroids suggest a difference in pathogenesis to idiopathic bronchiectasis.