Article Text

Abstract
BACKGROUND IgG subclass deficiency is often associated with recurrent pulmonary infections. The prevalence of deficiency in a large well characterised group of patients with bronchiectasis has not previously been established.
METHODS Serum IgG subclass concentrations in 89 patients with bronchiectasis were compared with those obtained from a group of 82 age and sex matched normal healthy controls. Sputum IgG subclass concentrations were also assessed in 44 of the patients. Albumin was measured as a marker of protein transudation from plasma to determine the degree of local IgG subclass production.
RESULTS The serum concentrations of IgG1, IgG2 and IgG3 were increased in the patients compared with the control group whereas IgG4 concentrations were not. There was an overall incidence of deficiency of 1% for subclasses 1–3 and 5% for subclass 4 in patients with bronchiectasis based on observed concentrations being below the lower limit of the control group range. The concentrations of IgG subclasses in sputum were partly dependent upon the degree of inflammation as assessed by the macroscopic appearance of purulence. A comparison of the ratio of sputum:serum subclass concentration and sputum:serum albumin, however, revealed that all of the subclasses were present at greater concentrations than could be accounted for by transudation alone.
CONCLUSIONS A new normal control range for serum IgG subclasses has been established and from this range it was found that IgG subclass deficiency in a group of unselected patients with bronchiectasis was comparatively rare. A significant degree of local IgG production was also suggested in the lungs of these patients.
- IgG subclasses
- bronchiectasis
- sputum
- normal ranges
Statistics from Altmetric.com
IgG subclasses have been measured in patients with chronic or recurrent respiratory infections by several groups and estimates of the incidence of deficiency of one or more of the subclasses in these patients has been as high as 38%.1 This has led various authors to suggest that these disease conditions may be associated with a variety of single or combined subclass deficiencies, notably IgG2,2 ,3 IgG3,1IgG4,2 ,4 or the combination IgG2and IgG4.5
Differences in the incidence of deficiency reported in patients by various groups can often be explained by the source and nature of the normal range used for comparison. The values from as few as 20 individuals have been used to define normal limits for healthy adults,6 and ranges have been established using a variety of criteria—for example, the entire range of values derived from control samples,6 the 5th and 95th percentiles,7 or two standard deviations about the mean.1 ,2 The last definition relies on a normal distribution of values. As previously suggested, both this and the use of percentile ranges would naturally identify a proportion of normal healthy individuals as being subclass deficient.8 This was illustrated in a study of IgG2 levels in healthy blood donors where the levels were not normally distributed and more subjects had values greater than 3SD below the mean than would be predicted.9 Furthermore, the use of different laboratory immunoassays to establish normal ranges and patient values may also account for discrepancies in the results from various groups.
A final problem relates to the patient groups studied, since many reports include a heterogeneous population with either persistent or intermittent respiratory infection with the results subsequently applied to specific disease entities. IgG subclass deficiency in bronchiectasis is thought to be associated with the development of the condition.10 There were, until recently, two major studies in this patient group, both of which suggested that the incidence of IgG subclass deficiency is low,11 ,12 and in one of these studies the control group consisted of patients with established lung disease rather than healthy subjects. However, a recent study from Spain in patients with bronchiectasis ranging in age from 10–74 years has suggested a much higher incidence.13 This group used a percentile range from control values which, as discussed above, naturally identifies a proportion of normal individuals as deficient. The true incidence of deficiency in bronchiectasis is thus unclear. Identification of IgG deficiency in these patients is important since benefit may be derived from replacement therapy. However, local antibody production in the lung may be more important than serum immunoglobulin levels, particularly as the lung is the site of infection and inflammation in these patients, and would therefore be important in antibody dependent clearance mechanisms although this aspect has yet to be evaluated in bronchiectasis.
The purpose of the studies reported in this paper is twofold; firstly, to establish the incidence of serum IgG deficiency in a large group of patients with bronchiectasis compared with age and sex matched healthy control subjects, and secondly,to assess the presence of IgG subclasses in the lung secretions of patients with bronchiectasis and to determine the extent of local in situ production.
Methods
PATIENTS AND CONTROLS
Eighty nine patients with bronchiectasis (55 women) of mean age 58.4 years (range 23–81) were studied. The diagnosis of bronchiectasis was established radiologically by bronchography or high resolution CT scanning. The aetiology of the disease was unknown although in most patients the onset of symptoms followed a childhood illness such as whooping cough or pneumonia. All 89 patients had a persistent cough and daily sputum production, only two were current smokers but most (51) had never smoked. None had cystic fibrosis or α1-antitrypsin deficiency. All were regularly attending a specialist bronchiectasis clinic and were clinically stable at the time of being studied with no evidence of pyrexia or acute increase in cough, breathlessness, or sputum production. None of the 89 patients had received antibiotic therapy within the four week period preceding the study. All patients provided a 10 ml venous blood sample and the serum was obtained by low speed centrifugation and stored at –40°C until analysed. Sputum samples (collected into sterile containers for four hours from waking) were provided at the same time by 44 of the patients (28 women) of mean age 60.7 years (range 39–81) and were classified as mucoid, mucopurulent, or purulent according to the macroscopic appearance of the samples as previously described.14 Sputum sol phase was obtained by refrigerated high speed centrifugation (50 000g) for 90 minutes and stored at −40°C until analysed.
In addition, venous blood was collected from 82 normal healthy subjects (51 women) of mean age 56.9 years (range 22–90) and serum was obtained. None of these control subjects had a history of chronic respiratory disease or recurrent respiratory tract infections (11 were current smokers). None was suffering from acute upper or lower respiratory tract infection or receiving any prescribed medication at the time of the study.
MATERIALS AND LABORATORY METHODS
The four IgG subclasses were measured in serum samples from patients and controls and in sol phase sputum from patients by radial immunodiffusion using prepoured plates (The Binding Site, Birmingham, UK) containing subclass specific sheep polyclonal antisera. Subclass concentrations of the samples were obtained by reference to purified protein standards applied in accordance with the manufacturer’s recommendations. The lower limit of detection was 0.0025 g/l for each IgG subclass and within batch coefficients of variation (CV) were equal to or less than 5% for all subclasses in sputum and serum (n = 6). The between batch CV was less than 8% for each subclass (n = 6), confirming the reproducibility of these assays for the measurement of IgG subclasses in both sputum and serum samples.
To determine the possibility of IgG subclasses in sputum being under or overestimated, samples of mucoid, mucopurulent, and purulent sputum were measured before and after the addition of a known quantity of purified IgG subclass (The Binding Site, Birmingham, UK). No major overestimation was observed, with results varying from +5% to –20% of the predicted value.
Albumin in serum and sputum from the 44 patients (where sputum was collected) was measured by radial immunodiffusion using 1% agarose in 0.1 M barbitone buffer (pH 8.6) containing 3% polyethylene glycol 8000 and sheep polyclonal antibody to human albumin (The Binding Site, Birmingham, UK). Plates were incubated at room temperature for 48 hours and the precipitation ring diameter was measured to the nearest 0.5 mm. Albumin values were obtained by interpolation from a standard curve constructed from a pooled normal serum standard (44.4 g/l). The lower limit of detection of the assay was 0.03 g/l, within batch CV was 7% (n = 6), and between batch CV was 9% (n = 5).
STATISTICAL METHODS
Serum IgG subclass values in patients were compared with control subjects. Deficiency of IgG subclass levels in the patient group was identified as values which fell below the lower limit of the control group. Sputum IgG subclass values were divided according to the nature of the secretions (mucoid, mucopurulent, and purulent) and compared. Sputum: serum albumin ratios were calculated and compared with sputum:serum IgG subclass ratios to assess the contribution of transudation from plasma and hence the inferred degree of local production as described previously.15 All data were expressed as medians and ranges. Differences between groups were analysed using the Mann-Whitney U test for non-parametric data (paired and unpaired, where appropriate) and accepted as significant at p < 0.05.
Results
SERUM IgG SUBCLASSES
All subclasses were detected in each serum sample obtained from both patients and healthy control subjects. The individual values and the medians and ranges for the patients with bronchiectasis and healthy subjects are shown in fig 1A–D. In patients the median serum concentration of IgG1 was 6.89 g/l (range 2.50–14.87), for IgG2 was 3.74 g/l (0.32–7.81), and for IgG3 was 0.79 g/l (0.06–4.38). These were significantly higher (p < 0.001) than the median concentrations observed in the control subjects (IgG1 5.25 g/l, range 2.52–14.12; IgG2 2.91 g/l, range 0.63–7.28; IgG30.5 g/l, range 0.10–2.30). Values for IgG4 (median 0.26 g/l, range 0.02–3.41) were similar to the control group (median 0.31 g/l, range 0.03–5.51).

(A–D) IgG subclass concentrations in serum from 89 patients with bronchiectasis and 82 healthy control subjects. Medians are indicated by solid lines.
Six patients had values at or below the lower end of the normal range. One patient had a low IgG1 level, one a low IgG3 level, four had low IgG4 levels (one patient also had low levels of IgG2). Based on the established healthy control range, the overall deficiency of IgG1, IgG2, and IgG3 was 1% and was slightly higher (5%) for IgG4 in this patient group.
SPUTUM IgG SUBCLASSES
The 44 patients who also supplied sputum samples had serum IgG subclass concentrations within the normal range established from the control group as shown in table 1. There was no relationship between serum subclass concentration and the nature of the secretions produced by these patients (table 1, fig 2A, B). All immunoglobulin subclasses were identified in each sputum sample studied, with the exception of two samples in which IgG4 was undetectable (< 0.0025 g/l). The median sputum concentrations and ranges are shown in table 1 and fig 2. In general, the concentration of subclasses in each secretion was in the order IgG1 > IgG2> IgG3 > IgG4.
Median values (and ranges) of IgG subclasses in sputum and serum from 44 patients with bronchiectasis
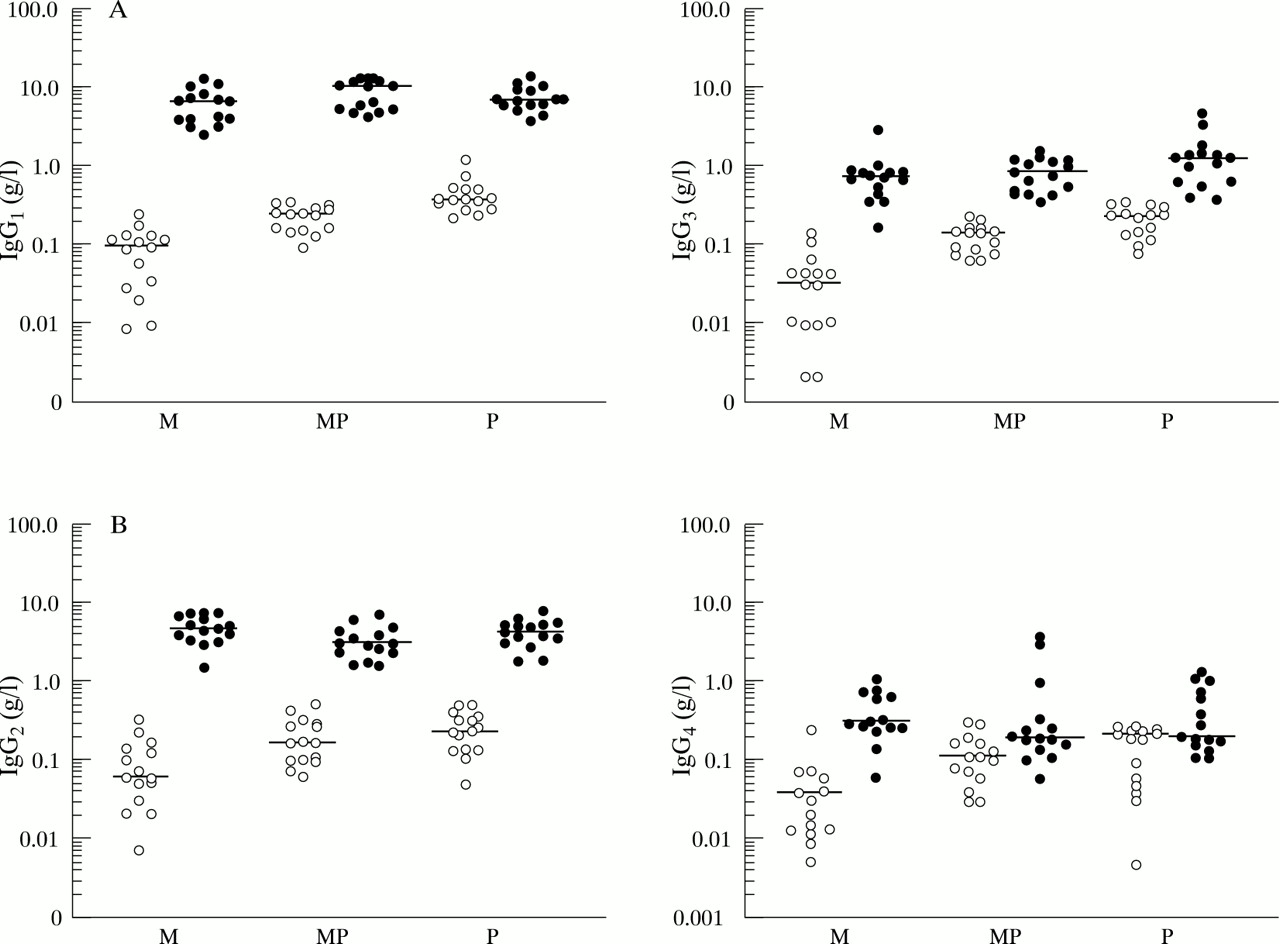
(A, B) IgG subclass concentrations in paired sputum and serum samples from patients with bronchiectasis. Median values are indicated by a solid line. Open circles represent sputum values and closed circles represent serum values. The values are divided into the three sputum colour categories (M = mucoid; MP = mucopurulent; P = purulent).
The median sputum concentration of all subclasses generally increased with purulence. This increase was significant between mucoid and mucopurulent samples (p < 0.005) and mucoid and purulent samples (p < 0.001) for all subclasses. Differences between mucopurulent and purulent samples were only observed for IgG1 and IgG3 (p < 0.005).
IgG subclass concentrations were lower in sputum than in serum, with the exception of IgG4 in some samples (fig 2B). The median concentration of IgG1 and IgG2 in mucoid sputum was 1–2% of the serum value (table 1), whereas the relative concentration of IgG3 and IgG4 in sputum was higher, being 4% and 6% of the serum value, respectively. The ratio of sputum:serum concentration for IgG1 increased progressively from mucoid to mucopurulent samples (p < 0.01) and mucopurulent to purulent samples (p < 0.001) as shown in table 1. In subclasses IgG2, IgG3, and IgG4 the ratio of sputum:serum concentration increased from mucoid to mucopurulent secretions (p < 0.01) but no further increase was observed in purulent samples (table 1). A similar pattern emerged when the sputum:serum IgG subclass ratios were corrected for the sputum:serum ratio of albumin to assess local production (table 1, fig3), although fewer differences reached statistical significance (IgG1, mucoid to purulent: p < 0.01; IgG2mucoid to mucopurulent: p < 0.001; IgG3 mucoid to mucopurulent or purulent: p < 0.02; and IgG4 mucoid to mucopurulent or purulent: p < 0.05).
{kind=link}
{kind=link}
{kind=link}
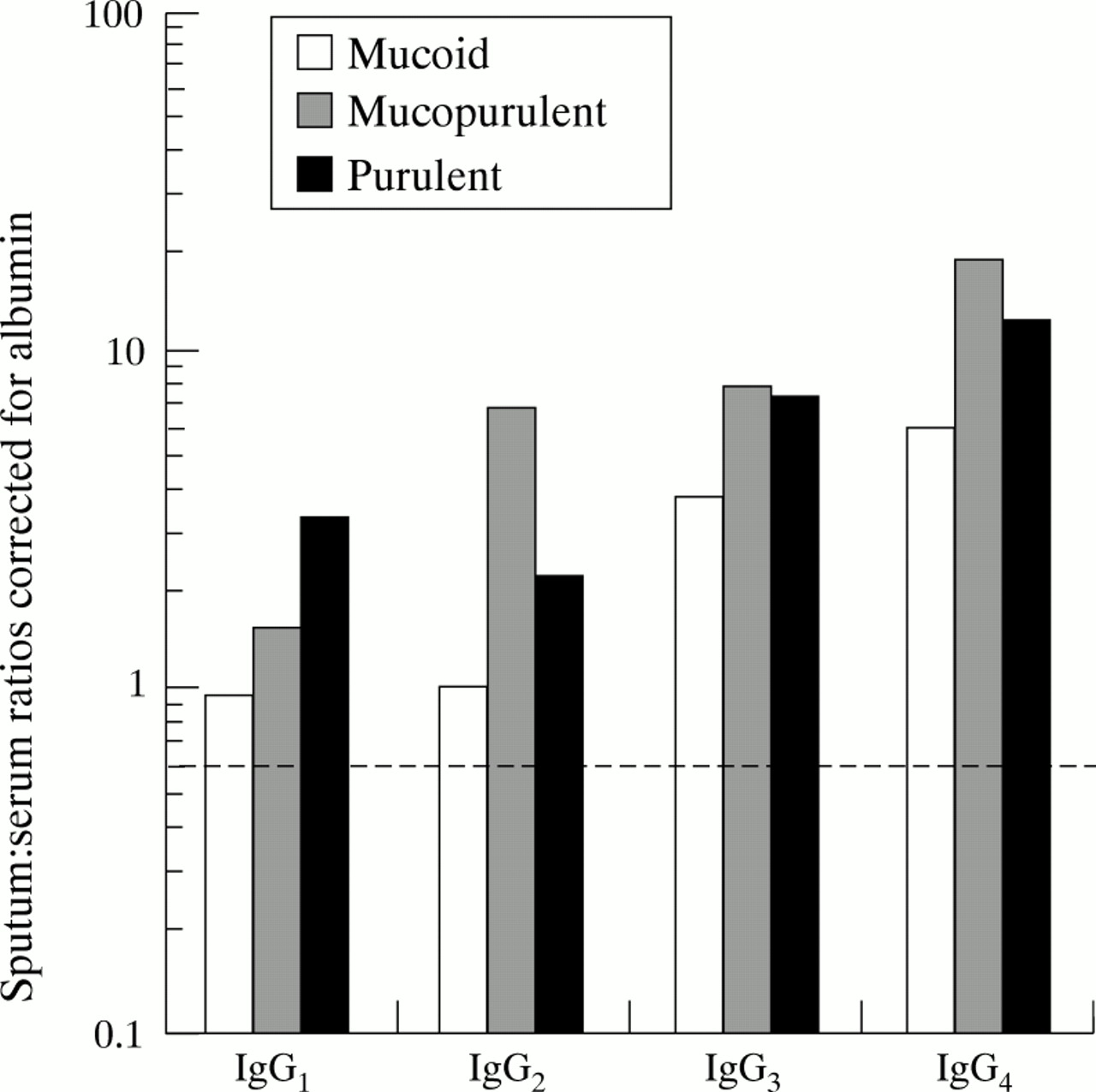
Median sputum:serum IgG subclass ratios corrected for the sputum:serum ratio of albumin. The dashed line represents the expected ratio if both IgG and albumin enter the lung by diffusion alone. The results are shown divided into the three sputum colour categories.
Discussion
This study establishes a new range for serum IgG subclasses in healthy adults. The entire range of values from this group of control subjects was compared with values obtained from patients with bronchiectasis in order to determine the incidence of IgG subclass deficiency in this chronic lung disease. The two groups were of equivalent size and were matched for age and sex. All measurements were made by the same laboratory using consistent measurement techniques. Examination of the control range described here reveals that the lower limit for each subclass was consistently lower than those of control ranges published previously,6 ,9 ,12 ,16 which is probably due to our use of the entire range of measured values instead of 95th and 97th centile ranges or two standard deviations from the mean. French and Harrison have already shown that the frequency distributions of IgG subclasses in the serum of healthy adults is skewed, and that the use of the entire range or 95th centile range for each subclass is more acceptable than ranges defined by standard deviations.9
Using our control range, six patients with bronchiectasis (6.6%) had serum IgG subclass values lower than healthy subjects, and the relative deficiency in this sample population was 1% for IgG1, IgG2 and IgG3, 5% for IgG4, and 1% for IgG2 and IgG4 in combination. The most widely quoted normal range is that of Oxelius and colleagues6 and, using that range, 12 of our patients would be classified as having IgG1 deficiency, two IgG2 deficiency, 12 IgG3 levels below and three at the limit of the range, and one with IgG4 deficiency (13%, 2%, 13%, and 1%, respectively). The range we describe is wider than that reported by Oxelius et al,6probably because their group only consisted of 20 healthy subjects and different laboratory methods were used. It would appear that our normal control range is more relevant, particularly since the same measurement techniques were used throughout and the whole of the normal age and sex matched control range was employed for comparative purposes. The results presented here show that serum IgG subclass levels in this group of adult patients with bronchiectasis associated with chronic sputum production are predominantly normal. In addition, the data presented here indicate that the IgG levels for the group as a whole ware higher than the normal healthy control subjects. This latter finding is consistent with data published by other workers,11 ,12 suggesting increased activity of the immune system in response to chronic infection.
The studies here, however, conflict with the results of the study by de Gracia and colleagues13 who reported that 48% of patients with bronchiectasis had low serum concentrations of IgG subclasses. The majority of patients classified as deficient had low levels of IgG2 (29%) with no reported deficiency of IgG1and similar incidences of IgG3 and IgG4deficiency (3% and 4%, respectively). This may reflect the use of a percentile control range where the lower limits for each of the four IgG subclasses were much higher than the lowest limits observed in the healthy control subjects reported here. Our data support the previous suggestion that the use of such ranges naturally identifies a proportion of healthy individuals as being subclass deficient.8 This is particularly relevant to the IgG2 subclass results since, in the study by de Gracia and colleagues,13 the lower limit of their control range was 1.1 g/l compared with 0.63 g/l which was the lowest value measured in the healthy control range in this study. From the data provided in the paper by de Gracia and colleagues13 it was not possible to re-calculate the number of their patients who would remain IgG subclass deficient when compared with our control range and whether this was related to the younger age of the patients they studied (10–74 years).
Studies of serum IgG subclasses, however, are probably more relevant to systemic infections than they are to infections of the mucosal surface where local IgG production also occurs,17 ,18 and we have therefore studied IgG subclasses in secretions from some of the patients. Protein diffusion from plasma is responsible for a proportion of the immunoglobulin found in secretions, and this component increases with inflammation.15 Previous studies from our laboratory have shown that inflammation correlates positively with sputum purulence in patients with bronchiectasis,19 and therefore part of the increased sputum IgG levels (expressed in absolute concentrations or as % serum in table 1) in mucopurulent and purulent secretions will reflect increased transudation from plasma. In addition, a proportion of the IgG may be locally produced by resident lymphocytes and this may also increase with lung inflammation as has been shown for IgA and confirmed by staining of IgA subclass bearing plasma cells in bronchiectatic lung tissue.20
Absolute concentrations of IgG1 and IgG2exceeded those of IgG3 and IgG4 in all sputum samples assayed, and in purulent samples the concentrations of all IgG subclasses were greater than in mucoid samples. This, in part, reflects greater protein transudation from plasma which has been shown to be present in purulent sputum samples19 but the data also suggest an increase of local production. Separating local production from that due to transudation from plasma can be difficult. There can be little doubt that there is a major degree of local IgG4production because in some samples the sputum concentration exceeded that found in serum (fig 2). Comparison with albumin can provide some clarification for other samples and subclasses because it enters the lung by diffusion from plasma.21 If the albumin concentration in sputum is expressed as a percentage of its concentration in serum and compared with the corresponding value for each IgG subclass, a ratio of approximately 0.6 will result if both proteins are entering the lung by diffusion alone.22 It has therefore been suggested that ratios greater than 0.6 indicate significant local production.22 Comparison of the observed ratio with the expected ratio (0.6) enables an approximate estimate of the amount produced locally to be made.
The median value of the albumin-corrected ratio exceeded 0.6 for all subclasses in each sputum category studied (table 1). The proportion produced locally also showed some differences between subclasses. In mucoid sputum samples approximately 50–60% of the IgG1and IgG2 was produced in the lung (median ratios compared with albumin 1.42 and 1.38, respectively), whereas local production accounted for 80–90% of the IgG3 and IgG4(median ratios compared with albumin 3.65 and 5.90, respectively). Overall, the absolute concentrations of IgG1 and IgG2 still predominated in these secretions (table 1). In purulent samples the absolute concentrations of all IgG subclasses were greater than in the mucoid samples. Although this reflects increased protein transudation associated with inflammation, there is also evidence for increased local production. Between 70% and 80% of the IgG1 and IgG2 in purulent samples was produced locally, as indicated by median ratios compared with albumin of 3.20 and 2.13, respectively. This increased proportion of local production also rose to 93% for IgG3 and 95% for IgG4, with median ratios compared with albumin of 8.33 and 12.12, respectively. The absolute amount of IgG1 and IgG2, however, still exceeded that of IgG3 and IgG4 in these samples.
The results therefore suggest that there is significant local production of all IgG subclasses in the lungs of these patients with bronchiectasis. This local production increases in the presence of purulent secretions, indicating an enhanced local immune response where neutrophil infiltration and the presence of neutrophil elastase has been demonstrated.10 ,19 These general conclusions, however, are based upon median values and the assumed contribution of immunoglobulin by diffusion from plasma. Individual values showed a wide range and in two subjects IgG4 was not detected in the sputum (see results). Both subjects had serum IgG4 levels within the normal range of this study (0.28 and 0.19 g/l, respectively), but it should be noted that the presence of IgG4 in the plasma does not guarantee its detection in secretions. The diffusion gradient, even in the presence of inflammation, results in approximately 1–3% of plasma protein entering the secretions19 and this would be beneath the limit of detection of the assay for IgG4 for all samples. Thus, the presence of detectable IgG4 in the secretions is largely dependent upon local production. The failure to identify IgG4 in the secretions of these two patients suggests a possible absence of local production in the lung. An alternative possibility is the binding of antibody to bacterial antigens, thereby reducing the amount detectable in the sol phase of the sample. Further studies will be necessary to clarify these possibilities. Examination of the other subclass data for these two patients revealed that the first patient had detectable levels of all other subclasses although the sputum to serum ratio for IgG1 compared with albumin was less than 0.6 (0.17) which indicates a value below that expected by diffusion alone. Ratios for IgG2 and IgG3corrected for albumin did, however, indicate some local production (0.63 and 1.52, respectively). The second patient had IgG1, IgG2, and IgG3 subclass ratios corrected for albumin of 3.1, 1.8, and 2.4, respectively, suggesting that the deficiency was restricted to IgG4 in this patient.
Closer study of individual data from the remaining patients indicated that five (11%) and three (7%) had IgG1 and IgG2 ratios of 0.6 or less compared with albumin. In the IgG2 group one of the observed low ratios was associated with a marked increase in protein transudation which can overwhelm evidence of local production.15 In the other patients the low ratio compared with albumin may again represent local consumption of antibody by binding to bacterial antigens.
The interpretation of these sputum results remains uncertain at present. There can be no normal range available for IgG subclasses in sputum although Merrill et al 23 have studied IgG subclasses in normal lavage samples. The authors concluded that there was clear evidence for local production of IgG3 and IgG4 in the lung. Review of the data suggests that the lavage and serum values for albumin and IgG1 and IgG2 were similar (ratio of 1.0) and the authors concluded that their data did not indicate local production of these subclasses. They did not take into account, however, the larger size of IgG compared with albumin and hence their data, like ours, indicate a degree of local production of all subclasses even in health. Nevertheless, the added complication of disease makes it uncertain whether the results presented here represent the expected or a suboptimal response to bronchiectasis. We are therefore unable to determine whether the IgG subclass concentrations found in sputum from patients with bronchiectasis are lower than would be expected in the secretions of patients with the presence of an ongoing inflammatory response without a previous history of chronic or recurrent infection. Further studies are indicated to compare the degree of local production of each subclass and, more appropriately, the specificity and function of each of the subclasses, particularly at the site of infection within the lung where the effectiveness of antibody dependent clearance mechanisms will be critical for the removal of bacteria. The relationship between IgG and IgA concentrations and function in the airways will also be important and would determine whether quantitative or qualitative local immunoglobulin deficiency, rather than systemic deficiency, can be implicated in the disease process.
Acknowledgments
The authors wish to acknowledge the financial support of the United Birmingham Hospitals Endowment Fund, the British Lung Foundation and the General Hospital Bicentenary Appeal Fund. Grateful thanks also to Mrs Esther Ford for help in the preparation of the manuscript.