Article Text

Statistics from Altmetric.com
The plain chest radiograph, although useful in the assessment of acute asthma, mainly to exclude unsuspected pneumothorax, collapse or consolidation,1 ,2 is unable to demonstrate more subtle changes within the lungs of asthmatic patients. The ability of high resolution computed tomography (HRCT), with a theoretical resolution of 100 μm, to examine small structures within the chest is now being exploited in the investigation of asthma. Recent studies have focused on the visualisation of acute airway responses to bronchoconstrictor and bronchodilator stimuli as well as airway and lung parenchymal changes in chronic asthma.
Measurement techniques using HRCT
High resolution computed tomography has evolved from a combination of improvements in scanner hardware and the software used to reconstruct the images. The single most important feature in improving the spatial resolution is the slice thickness or collimation. In practice this is usually 1–1.5 mm. The second important feature of HRCT is to reconstruct the image using a high spatial frequency algorithm. This decreases contrast resolution and increases the visibility of image noise, but it significantly improves spatial resolution.3 Other features of HRCT are quick scan times to reduce motion artefact, and the use of targeted reconstruction when necessary. These techniques allow selected areas of the lungs to be viewed at close to the inherent maximal spatial resolution of the scan system. The data are manipulated in digital form by sophisticated software to produce the final image. Lung slices can then be examined for evidence of airway and parenchymal lung disease according to recognised criteria. HRCT scanning now has an established role in the investigation of diffuse parenchymal lung disease and bronchiectasis.4 The main disadvantages in the application of HRCT scanning in humans are radiation dose, the complexity of HRCT data analysis for the more complex edge finding algorithms,5 and technical problems over selection of phantoms for verification.
MEASUREMENT OF AIRWAY SIZE
HRCT scanning has been used in a number of recent studies to measure airway size in asthma. The main technical problem arises in defining the bronchial wall and lumen boundaries. A wide range of different measurement techniques have been used.
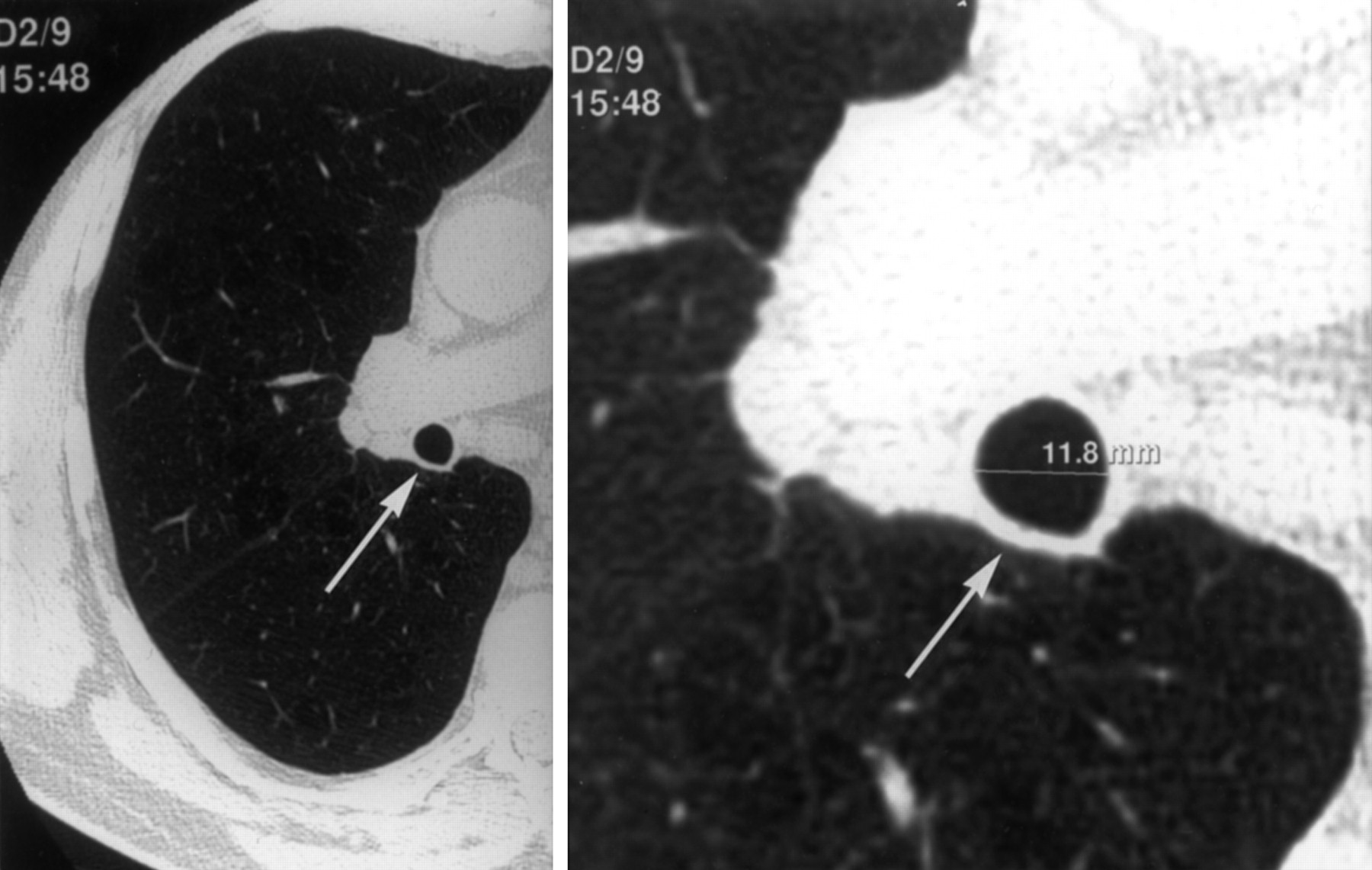
The choice of window level and window width affects the size of bronchi seen on the HRCT scanner console. In human and animal studies most investigators have used a window level of between –450 and –600 Hounsfield units (HU) and a window width of 1350–1600 HU. The simplest method is demonstrated by Boulet et al 6 who used electronic calipers to measure the internal diameter of second and third generation bronchi in humans. These were drawn directly onto the CT console video display unit by the operator (fig 1). Internal diameter and wall thickness of the intermediate bronchus could be clearly distinguished. Problems arose when smaller bronchi were studied as the interfaces between lumen, wall and lung parenchyma became harder for the operator to define as they became increasingly indistinct (fig2). Forkert and co-workers7 tried to overcome this problem by using a density plot of a straight line drawn perpendicular to the airway wall. The wall edge was assumed to lie at the mid point between airway lumen and wall densities. This technique does not rely on the subjective estimation of lumen/wall interface and the authors found that airways as small as 0.88 mm could be measured. The reproducibility of this technique was not, however, estimated and the investigators used image analysis of redigitised analogue images which introduces several sources of potential errors. Amirav and co-workers5 used a more complex edge finding program to estimate objectively bronchial cross sectional area in pigs. These investigators used Perspex phantoms to validate the technique and suggested that bronchi as small as 1 mm could be measured with close agreement with phantom measurements. McNamara and co-workers8 used sweet potato phantoms in their study in dogs (potato has similar attenuation to soft tissue) and confirmed an optimum window level of –450 HU for estimation of bronchial cross sectional area. However, their actual measurements were made from tracings of CT photographs. Another novel technique used by Seneterreet al 9 examined normal human lungs in vivo by HRCT scanning at minimum window width (2HU) and varying window levels. This technique gives a crisp “black and white” representation of bronchi (fig 3) from which the investigators could make repeatable measurements of bronchi down to 0.8 mm (sixth generation) in diameter. This particular technique requires extreme manipulation of the image and will need validation with morphometric or phantom studies.

HRCT scan of human intermediate bronchus (arrowed). Window level –600 HU, window width 1250 HU. Slice thickness 1.5 mm. The operator has used electronic calipers to measure the internal diameter on the console.
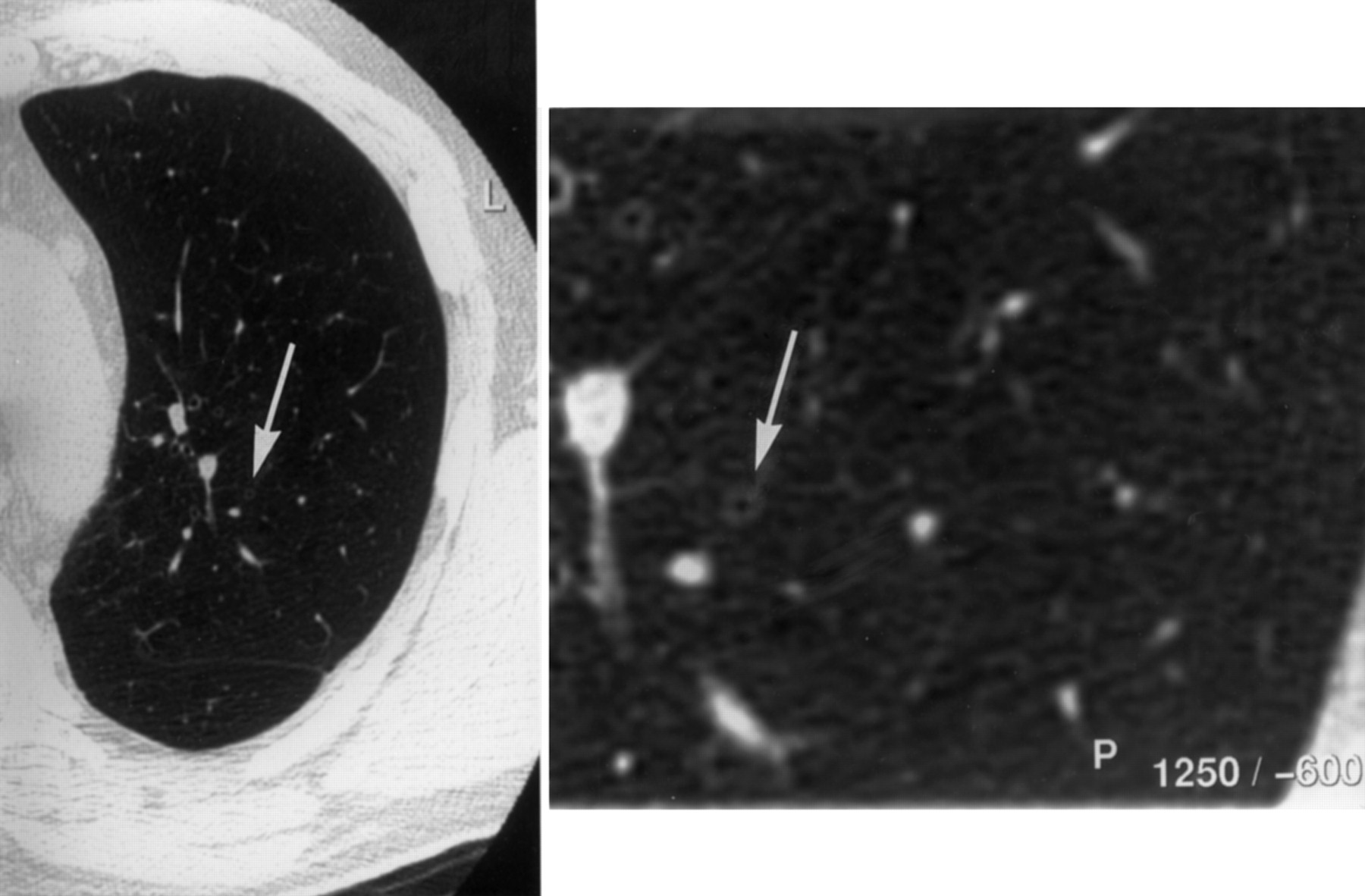
An example of a small bronchus (arrowed) in the left lung examined at the same window level, window width, and slice thickness as fig 1. The right hand image has been enlarged but demonstrates how the wall/lumen boundary is much less distinct than in fig 1. This bronchus is approximately 1.5 mm in diameter.

{kind=link}
{kind=link}
{kind=link}
The same slice of intermediate bronchus (arrowed) as in fig 1 at a window level of –600 HU and a window width of 2 HU. The wall/lumen interface is crisply delineated but this method has not been validated by phantoms.
The thickness of airway wall in post mortem specimens of lung has been calculated from tracings of the internal and external perimeter of the airway.10 ,11 An advantage of this technique is that the measurements remain constant at different lung volumes. These studies have established the presence of increased airway wall thickening in some cases of asthma. Similar measurements of the airway circumference could be used to calculate the size of airways seen on HRCT scanning.
It appears, therefore, that HRCT scanning can be used to measure bronchi as small as 1 mm in diameter. Several unresolved methodological issues remain, however. It is not known how closely the CT measurements compare with in vivo airway dimensions. For example, airway secretions may result in an overestimation of airway wall thickness and there is little information on the reproducibility or comparison of the different techniques used.
Acute airway responses
Direct visualisation of acute bronchial responses has previously been achieved by tantalum bronchography12 and more recently bronchial calibre has been measured by quantitative videobronchoscopy.7 These procedures are highly invasive, and videobronchoscopy is limited by the size of bronchoscopes and has only been described in anaesthetised dogs. HRCT scanning has now been used in both animals and humans as the first non-invasive method to study the site and degree of acute changes in airway calibre.
The initial studies5 ,8 ,13-15 to measure variation in bronchial size in response to bronchoconstrictor stimuli were restricted to in vitro or animal experiments. Brown and colleagues13 ,14 examined anaesthetised dogs by HRCT scanning to measure changes in the size of the airways in response to aerosolised and intravenous histamine. Airways down to 1 mm diameter were measured. There was a 10–100% decrease in airway area throughout all sizes of bronchi following histamine administration, with no relation seen between airway size and reactivity. These authors concluded that the bronchoconstriction was predominantly controlled by local airway mechanisms rather than being due to the unequal distribution of histamine. The study in anaesthetised pigs by Amiravet al 5 established dose related airway constriction using intravenous methacholine and again found heterogeneity in airway responsiveness. Excised canine lungs have also been examined by HRCT scanning8 and, as well as confirming the ability of HRCT to distinguish airway narrowing, McNamara and co-workers also noted the phenomenon of a paradoxical decrease in bronchial wall thickness during bronchoconstriction. They speculated that, if this change was not artefactual, it may be due to a reduction in bronchial wall blood volume. In addition to investigations by various workers into changes with bronchoconstriction, Wetzel and co-workers16 have used HRCT scanning to visualise hypoxic bronchodilation in anaesthetised pigs.
Okazawa and coworkers17 have measured bronchial wall thickness and looked for the site of methacholine induced bronchoconstriction in human asthmatic subjects and controls using HRCT scanning. They found significant bronchoconstriction in all sizes of airways with the greatest change being found in those 2–4 mm in diameter. For a similar reduction in forced expiratory volume in one second (FEV1) both groups showed a similar reduction in mean airway luminal area. The walls of the smaller airways in the asthmatic subjects were significantly thicker than those of controls. In the normal airways bronchial wall thickness was seen to decrease on bronchoconstriction, similar to the same group’s findings in canine lungs.8 This reduction was not seen in the asthmatic airways and the authors suggest that this failure of the bronchial wall area to reduce on bronchoconstriction may be a contributing factor to hyperresponsiveness in asthma.
In summary, these findings emphasise the usefulness of HRCT scanning in defining the site and scale of dynamic airway changes in detail not previously possible. The initial animal studies show a heterogeneous response of airways to bronchoconstrictor stimuli and also confirm that individual airways can be followed over time. The study in humans17 has shown non-invasively the site of bronchoconstriction directly. These studies have verified HRCT techniques for clinical studies examining responses of the larger airways to stimuli and drugs.
Abnormalities in chronic asthma
MUCOID IMPACTION AND COLLAPSE
There is a long recognised association between uncomplicated asthma and lobar or segmental collapse seen on plain radiographs, but HRCT scanning is able to resolve these changes in much smaller areas of the lung. Paganin and co-workers18 examined the HRCT scans and plain chest radiographs of 57 non-smoking asthmatic subjects without allergic bronchopulmonary aspergillosis (ABPA) and 10 controls. The control scans and radiographs were all normal. Plain radiographs of asthmatic subjects showed no areas of mucoid impaction and suggested consolidation or infiltration in only five (9%). In contrast, HRCT scans of asthmatic subjects showed mucoid impaction or collapse in 12 (21%) and seven (12%), respectively. Ten asthmatics underwent treatment with high dose oral corticosteroids following which all the above abnormalities resolved. There was no correlation between the severity of asthma and extent of reversible abnormalities. Grenier and co-workers20 examined 50 asthmatic subjects and 10 controls by CT scanning and found mucoid impaction in 16.5% of asthmatics but none in the control group. These studies suggest that even apparently mild asthmatic subjects (Aas19 score 1–2) may have unsuspected areas of mucoid impaction. The clinical significance of this abnormality is uncertain but these studies do demonstrate the sensitivity of HRCT scanning in detecting mucoid impaction.
EMPHYSEMA, AREAS OF HYPERLUCENCY AND AIR TRAPPING
Investigators examining smokers undergoing elective thoracotomy for bronchial carcinoma21-24 have confirmed that CT and HRCT scans are highly sensitive in confirming the presence and degree of emphysema. Subjective descriptions of CT and HRCT appearances of emphysema include areas of non-peripheral and peripheral low attenuation,21 pulmonary vascular pruning and distortion,21 ,23 vascular disruption,25 or obvious bullae.22 Investigators have also described an objective technique, the “density mask”,22 which can quantify the areas of reduced attenuation. The HRCT appearances of emphysema are distinct from areas of hyperlucent lung due to reduced perfusion seen with mosaic perfusion.26 ,27
There is uncertainty over the nature of similar hyperlucent areas seen on CT scans of asthmatic subjects and whether these represent either emphysema with alveolar wall destruction or simply non-destructive hyperinflation. Estimations of prevalence of emphysema in asthmatic lungs using CT or HRCT scanning range from 0% to 80%.18 ,28-31 Kinsella and co-workers used CT scanning with 10 mm slices to examine smokers and chronic asthmatics.28 Asthmatic subjects with high total lung capacity showed no evidence of emphysema (defined by abnormally low attenuation, vascular disruption, or obvious bullae) whereas all the smokers with a total lung capacity of more than 120% predicted had emphysema. Lynch et al 31 examined 48 asthmatics (21 smokers) and 27 controls by HRCT scanning. None had evidence of ABPA but some were being investigated for suspicion of bronchiectasis. They found that asthmatic subjects with emphysema smoked more and had poorer lung function than those without. Paganinet al 29 used HRCT scanning to examine 126 asthmatics who had never smoked. Criteria for diagnosing emphysema were based on the validated CT/pathology study by Foster et al.21 The prevalence of emphysema correlated with asthma severity (Aas score); up to 80% of those with Aas score 4–5 showed features of centrilobular emphysema. The highest emphysema scores were seen in those who were non-allergic with more severe disease. Emphysema was not seen in any of the controls. Most CT studies are performed at full inspiration but there is evidence that expiratory CT may detect areas of air trapping due to unsuspected small airway disease32 ,33 and more work is needed to further characterise this phenomenon in asthmatic subjects.
Although there is little doubt that HRCT scanning is sensitive to the changes of emphysema in smokers’ lungs, the specificity of the technique in asthmatic lungs is not known. Despite this, it does seem that emphysema—or at least “terminal air space enlargement”34—is a frequent finding on HRCT examination of asthmatic lungs and that its severity may be proportional to the severity of asthma. Paganin and co-workers29 suggest that the pathogenesis of emphysema in (non-smoking) asthmatics may be quite different from that of smoking related emphysema. Instead of direct destruction of the distal air space they suggest that the respiratory air space enlargement may be produced by fibrotic change and airway remodelling. Future studies will need to define carefully the pathology demonstrated by HRCT scanning, but it seems that the degree of terminal air space enlargement could be used as a guide to the degree of overall remodelling.
BRONCHIECTASIS AND BRONCHIAL DILATATION
HRCT scanning has an established role in the diagnosis of bronchiectasis.35 Several studies have shown a higher prevalence of bronchiectasis in non-ABPA asthmatics compared with controls using HRCT scanning.18 ,29-31 These bronchiectatic changes were defined anatomically as bronchial dilatation but were usually asymptomatic. In these studies bronchiectasis was deemed to be present if the bronchial diameter was greater than that of the accompanying artery.36 ,37 Most studies then subdivide it, according to the Reid criteria,38 into three types: cylindrical, varicose, or cystic. Lynch and colleagues31 have suggested that this definition may overestimate the prevalence of bronchiectasis. In their asthmatic group 36% of the bronchi fulfilled the criteria for bronchiectasis but so did 26% of the control bronchi, although there was a difference in the techniques used as fewer slices were taken from the control group. Others have found no features of bronchiectasis in healthy controls.18
There is some conflict as to the prevalence of bronchiectasis in uncomplicated (that is, non-ABPA) asthma. Reported rates vary from 80% of moderately severe asthmatics (Aas score 3)18 to only 18% of asthmatics with positive skin tests but no other features of ABPA.30 Despite this discrepancy, which may have been due to a difference in patient groups and scanning techniques, it is clear that bronchiectasis or bronchial dilatation detectable on HRCT scanning is an established complication of non-ABPA asthma. These changes do not appear to respond to oral steroids18 and are probably permanent. It might be reasonable to suppose that there is a natural progression from the milder to the more severe forms but this has not been studied. The most recent study by Paganin and co-workers29 suggested that the prevalence of all forms of bronchiectasis increased with disease severity and, like the emphysematous changes, the abnormalities found on HRCT scanning were more extensive in the subjects with the highest Aas scores. Grenieret al 20 found the incidence of bronchiectasis in non-ABPA asthma to be 28.5% in 50 patients. There was not such a clear cut relationship with asthma severity as in the previously described study, but the number of affected lobes was significantly greater in the more severely affected patients.
BRONCHIAL WALL THICKENING
Lynch et al 31 found bronchial wall thickening in 42 of 44 asthmatic subjects (92%) compared with five of 27 controls (19%) and Angus et al 30 found bronchial wall thickening in nine out of 11 non-ABPA asthmatics and 16 out of 17 ABPA asthmatics. The two studies of Paganin and coworkers18 ,29 also confirm increased prevalence of bronchial wall thickening in asthmatics and Grenier et al 20 report an incidence of 82%. The pathological nature of the thickened walls is not known. It may be due to chronic inflammation or established peribronchial fibrosis. The failure of response to oral steroids18 tends to support the concept that this is a fixed structural change in the lung and a marker of airway remodelling. However, the effect of more prolonged treatment on bronchial wall thickening has not been studied.
In an attempt to clarify the relationship between bronchial wall thickening and airway reactivity Boulet et al 6 objectively quantified wall thickness by HRCT scanning in non-smoking asthmatics. Although they studied smaller bronchi it was found that only the wall of the intermediate bronchus could be reliably measured, due mainly to its large size and convenient orientation. In the asthmatic group with an element of fixed airflow obstruction thicker walls were associated with a lower PC20for methacholine. This study has limitations, since the finding in the intermediate bronchus may be unrelated to changes in smaller airways.
In this issue of Thorax Awadh et al 39 describe a relatively simple method of estimating airway wall thickness of segmental and subsegmental bronchi by HRCT. Measurements of bronchial wall thickness and luminal diameter were averaged from all bronchi with a luminal diameter of >1 mm in five selected scan levels per subject. From these values the ratio of airway wall thickness to total diameter(T/D ratio) and the percentage wall area (WA%) were determined. A total of 40 asthmatics were subdivided into three groups—a history of near fatal asthma (n = 14); moderate asthma (n = 12); mild asthma (n = 13)—and 14 normal controls were studied. The mean FEV1 values were significantly lower in the first two asthmatic groups (68% and 73%, respectively) compared with the mild asthmatic group (102%), which suggests that these individuals had more severe disease. The main findings are that patients with asthma have greater airway wall thickening than normal subjects and that those with severe disease have thicker airways than patients with milder disease. These findings are in keeping with post mortem studies in asthma10 ,11 and would support the concept of chronic inflammation causing bronchial wall thickening and remodelling. Nevertheless, there remain unanswered questions about the reproducibility of the measurements used in this study. Also, in the absence of information on reversibility testing to acute bronchodilator and/or short course steroid treatment, it is uncertain whether the airway wall thickening found in the more severe asthmatic patients indicates irreversible changes to the structure of the airways.
CHRONIC ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS (ABPA)
Central (proximal) bronchiectasis has long been recognised as a pathognomic feature of asthma complicated by ABPA.40Panchal et al 41 compared CT scanning with bronchographic appearances in 21 patients with ABPA and concluded that CT scanning had a sensitivity of 70% and a specificity of 92% compared with bronchography. Radiation doses were minimised by using thick slices of 4–8 mm. Had they used HRCT it is likely that the sensitivity would have increased. Using 3 mm HRCT slices Anguset al 30 found bronchiectasis in 14 out of 17 patients with ABPA; the disease was central in 39 of the 43 affected lobes studied. However, central bronchiectasis was seen in three lobes of the non-ABPA subjects. This study also found an increased incidence in pleural thickening, parenchymal shadowing, and emphysema in the ABPA group compared with non-ABPA asthmatic controls. Because the ABPA group were on larger doses of steroids and had poorer spirometric values, it is unclear whether these features were due specifically to ABPA or to more severe asthma. Other studies42 ,43 have found a similar incidence of bronchial dilatation in ABPA. In summary, central bronchiectasis seen on CT scanning in asthmatic subjects is strongly, but not exclusively, related to ABPA. It is not known whether ABPA shows any other classical features on HRCT scans which distinguish it from other forms of chronic asthma.
Future studies using HRCT scanning in asthma
PATIENT SELECTION AND METHODS
Future studies will need to define carefully the patient groups under examination. In the published studies in chronic asthma different patient groups were examined and different HRCT techniques and scoring methods were used. Some investigators used the ATS criteria44 to define their asthmatic group, others used less narrowly defined criteria. Not surprisingly, the smokers studied by Lynch and coworkers31 were more likely to have emphysema than non-smokers. Varying CT window levels (–600 to –800) were used to view the lungs with varying window widths (1000–2000 HU). The thickness and spacing of slices also varied from 3 mm thick slices at 9 mm intervals31 to 1 mm slices at 15 mm intervals.29 The optimum number of slices is not known and will be dictated by cost, local expertise, scanner availability, and ultimate radiation dose. We suggest that a minimal examination should at least include one cross section of each lobe. In serial examinations for research purposes it may be difficult to justify the radiation dose from multiple slices taken at close intervals of 10–15 mm. Future developments in scanner hardware and software may theoretically improve resolution beyond the current limit of 100 μm.
Once the HRCT images are obtained investigators have quantified the abnormalities seen in different ways. If subjects are simply scored for the presence or absence of an abnormality then a subject with one small area of affected lung will have the same statistical validity as a subject with widespread similar abnormalities. Paganin et al 29 confirmed the presence or absence of individual abnormalities for each lobe and gave a simple summative score for total abnormalities for each patient. While a final score is appealing, this method’s main drawback is that the relative contribution to overall remodelling made by any one abnormality is unknown. A relatively minor but common abnormality would have a disproportionate effect on the final score. We tried to simply quantify the amount of bronchiectasis in our groups of asthmatic patients with ABPA or Aspergillus fumigatus skin test positivity by summing the total amount of affected lobes in each group examined.30 This method appears to give a good impression of the overall prevalence and severity of the abnormality in the group examined. Until we know the relative importance of the major abnormalities seen it would be reasonable to report the numbers of patients or lobes with each abnormality.
The reproducibility of measurements obtained by HRCT scanning is still in question. Few of the investigators examining airway size and responses describe repeated measurements of the same bronchi and two of the studies in chronic asthma used consensus scoring by two or three radiologists but without reference to any inter-observer or intra-observer variability.18 ,29 Grenier et al 20 tested agreement between four radiologists in describing findings in 50 asthmatics. One observer read the same scans twice within three months to assess intra-observer variability. They found wide variation in the reporting of mucoid impaction and air space consolidation but significant agreement between observers about the frequency of bronchial wall thickening and bronchiectasis. The intra-observer agreements for the presence of bronchiectasis and bronchial wall thickening were excellent and good, respectively, but only fair for mucoid impaction. It is not known whether consensus scoring has an advantage over individual radiologists’ scores and future investigators will need to describe scoring techniques, especially if following the appearance of asthmatic lungs over time. There may be a role for control scans in ensuring reproducibility.
APPLICATIONS
Acute airway responses
The studies examining acute airway responses in animals and humans suggest that HRCT scanning may be used to measure directly the site of responses to bronchoconstrictor and bronchodilator stimuli. The ability to define the main site of action of bronchodilator drugs may allow more accurate targeting of drugs and delivery devices.
Assessment of chronic asthma
The studies examining airway and parenchymal changes in chronic asthma were predominantly cross sectional in design and only one18 re-examined the patients following treatment (with oral corticosteroids). At present the relative contributions of each abnormality to the overall functional impairment is unknown and there is scope for further cross sectional studies to clarify the relationship between the various HRCT abnormalities and lung function in asthma.
There have been no long term studies of HRCT scanning in asthma and this technique now offers a new non-invasive method of following the changes in asthmatic lungs and comparing treatment strategies. Previous studies of lung function in asthmatic subjects has shown an accelerated rate of decline in FEV1 in some groups45 ,46due to mechanical change and remodelling of the lungs.47-49 Spirometric testing is an insensitive technique in detecting small (<2 mm) airway disease as these airways account for only about one sixth of the total resistance to airflow.50 Many other functional techniques have been used to look for small airway disease including low density gas spirometry and measurement of closing volume.51 These tests may have the advantage of quantifying the functional disability but do not demonstrate the actual site and nature of the remodelling. In contrast, HRCT scanning can directly illustrate the site and nature of abnormalities. There is interest in the concept of early anti-inflammatory measures in asthma being used to protect against permanent damage and remodelling52 and longitudinal studies in asthmatic patients using HRCT could be used to identify patients most at risk of remodelling and consequent worsening lung function.
Conclusion
High resolution computed tomography has shown details of asthmatic lungs not previously obtainable. The principal disadvantages are cost and radiation dose. It can now be used to describe the site and size of large airway responses to stimuli in humans. HRCT scanning can also show a wide range of airway and parenchymal abnormalities even in subjects with mild asthma; the clinical significance of these is not known but there is an approximate correlation between severity of asthma and degree of abnormality which may represent remodelling of the asthmatic lungs. The ability to visualise and quantify remodelling in asthma non-invasively has great potential for assessing the long term history of asthma and response to treatment.