Article Text

Abstract
BACKGROUND Erythromycin has been reported to have an inhibitory effect on chronic inflammatory airway disease and chronic infiltration of neutrophils into the airway. Bleomycin (BLM) often induces interstitial lung fibrosis following acute lung injury. A study was undertaken to investigate the effects of erythromycin (EM) on experimental bleomycin-induced acute lung injury in rats.
METHODS Bleomycin-induced lung injury was assessed by light microscopic examination, measurement of neutrophil elastase activity and of the interleukin 8 (IL-8) content in bronchoalveolar lavage (BAL) fluid. The potential inhibitory effect of erythromycin was assessed by overall comparison of erythromycin untreated (BLM alone), concurrently treated (BLM + EM), and pretreated (BLM + pre-EM) groups.
RESULTS The neutrophil count and concentration of neutrophil-derived elastase in BAL fluid were significantly different in the three groups. The morphological changes of lung injury were also less extensive in rats pretreated with erythromycin. However, these protective effects were not marked in the group concurrently treated with erythromycin. Moreover, the concentration of IL-8 in the BAL fluid tended to be less in the erythromycin treated groups; however, there were no significant differences between the bleomycin-treated groups.
CONCLUSION Erythromycin exhibits a prophylactic effect on acute lung injury induced by intratracheal administration of bleomycin, which is possibly associated with a downregulation of neutrophil-derived elastase.
- erythromycin
- bleomycin
- acute lung injury
Statistics from Altmetric.com
Bleomycin-induced lung injury in rats is a common experimental model used to examine inflammatory and fibrotic changes in the lung interstitium.1-3 Pathological features of the acute phase in bleomycin-induced lung injury is indicated by a prominent accumulation of neutrophils in the lung parenchyma.4 5These neutrophils cause progressive airway damage by the release of oxygen radicals and proteolytic enzymes, including neutrophil elastase.5-8 Interleukin-8 (IL-8) is a powerful cytokine inducing neutrophil accumulation into inflammatory sites.9-13
Diffuse panbronchiolitis (DPB) is a well known inflammatory airway disease in Mongolian nations14 15; however, the prognosis for DPB has been improved significantly by long term, low dose erythromycin treatment.16 17 In patients receiving oral erythromycin the increase in neutrophils in bronchoalveolar lavage (BAL) fluid was significantly reduced.18 In one study in which a lipopolysaccharide-induced acute lung injury in a rat model was used to study the effect of erythromycin it was found that erythromycin inhibited the release of IL-8 into the airways.19-21While consensus regarding the primary mechanism by which erythromycin improves the prognosis of DPB has not been established, it is possibly the result of its known anti-inflammatory effect.22 23
This study examined the inhibitory effects of erythromycin in bleomycin-induced lung injury and evaluated the mechanisms of the prophylactic effect of erythromycin on acute lung oedema and neutrophil chemotaxis in rats.
Methods
Male, four week old, Sprague-Dawley rats weighing an average of 250 g each were randomly divided into treatment groups for administration of the following agents: bleomycin (BLM) (Nippon Kayaku, Co Ltd, Tokyo, Japan) at 4.5 mg/kg in normal saline (0.6 ml) instilled into the trachea under general anaesthesia by ether at day 14, and/or erythromycin (EM) (Dainabott, Co Ltd, Osaka, Japan) 12 mg/kg in 10% ethanol administrated orally for seven or 21 days.
The number of rats ranged from 13 to 20 per group, and groups were defined as follows: group 1: BLM alone (n = 15); group 2: BLM + EM (from day 14 to day 21, n = 15); group 3: BLM + pre-EM (from day 1 to day 21, n = 20); group 4: EM alone (from day 1 to day 21, n = 13); and saline control (instilled into the trachea at day 14).
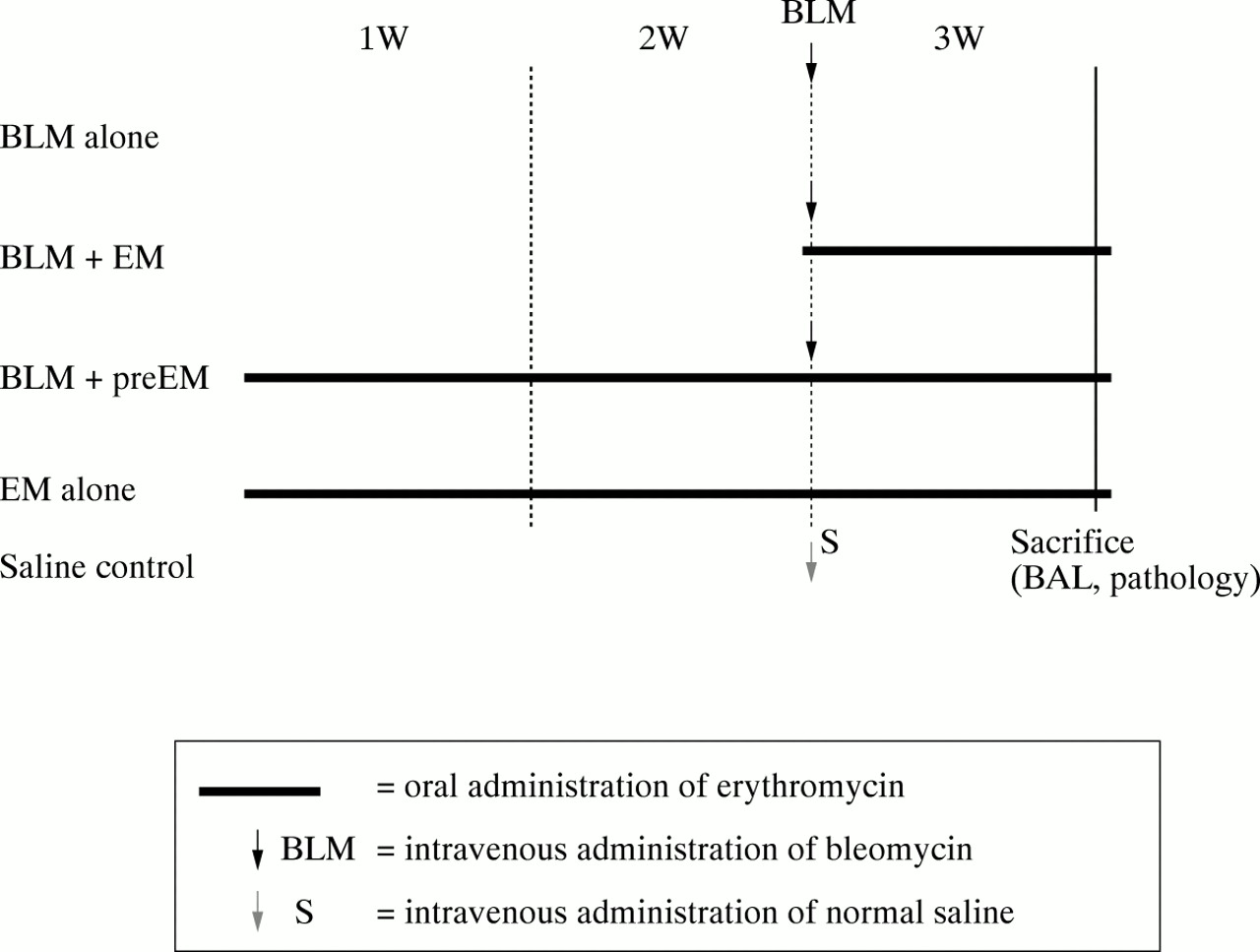
All rats were sacrificed at day 21 for evaluation of lung pathology, BAL cells and fluid. In the EM alone and 10% ethanol/saline groups, no remarkable findings were found. However, one rat in the BLM alone group, two in the BLM + EM group, and four in the BLM + pre-EM group died from acute aspiration pneumonia (fig1).

Bleomycin (BLM) and erythromycin (EM) administration schedules for each group.
ANALYSIS OF BAL FLUID
Rats were sacrificed under ether anaesthesia at day 7 after BLM treatment. BAL was performed by injection of 5 ml saline each (25 ml total) into the trachea through an intratracheal tube.24Recovery ratios of lavage fluids ranged from 60% to 70% and were not significantly different among groups. BAL cells were separated by centrifugation at 1500 rpm for 10 minutes and were used for measurement of neutrophil elastase activity, IL-8 content, cell population, and cell number.
Neutrophil elastase
Neutrophil elastase activity in BAL fluid was measured with a photoreader by measuring the change in substrate methoxy-succinyl-alanyl-alanyl-prolyl-valyl p-nitroanilide (Sigma, USA).25-27
IL-8 assay
IL-8 concentration in BAL fluid was measured with an enzyme-linked immunosorbent assay (ELISA) kit (Panafarm Lab, Kumamoto, Japan).28
Biopsy, histology, and graphical estimation
Lung tissue was removed and stained with haematoxylin-eosin (HE) for light microscopic evaluation. “Interstitial oedema” and “infiltration of inflammatory cells” were photographically evaluated as a bleomycin-associated acute lung injury. Adobe Photoshop 3.0J was used to detect these areas, and five longitudinal lung sections in each group were used for evaluation. The “ratio” was indicated by the number of black pixel areas.
STATISTICAL ANALYSIS
The statistical significance among the three groups of animals was tested with the Kruskal-Wallis rank test, a p value of less than 0.01 being considered significant. If significant, partwise comparisons between the two groups were performed using the Mann Whitney non-parametric test, a p value of less than 0.01 again being considered significant.
Results
BAL FLUID CELL COUNT
The mean (SD) total BAL fluid cell count in rats treated with BLM alone was 344 (155) × 103/ml) compared with 201 (76) for BLM + EM, 194 (49) for BLM + pre-EM, and 148 (56) for EM alone. Differences between the three groups (BLM alone, BLM + EM, and BLM + pre-EM) were statistically significant (table 1).
Comparison of total cell count in BAL fluid, percentage of neutrophils, and neutrophil counts among four groups
NEUTROPHIL RATIO IN BAL CELLS
The mean (SD) neutrophil ratios were 45.6 (17.1)% in the BLM alone group, 34.7 (21.7)% in the BLM + EM group, 8.6 (6.9)% in the BLM + pre-EM group, and 0.0% in the EM alone group. Significant differences were revealed in all of the groups. The mean (SD) neutrophil count was calculated as 156.9 (26.5) × 103/ml for BLM alone, 69.7 (16.5) × 103 for BLM + EM, 17.0 (3.4) × 103 for BLM + pre-EM, and 0 (0) for EM alone (table 1).
NEUTROPHIL ELASTASE ACTIVITY IN BAL FLUID
The sensitivity of the assay for neutrophil elastase was 0.1 nM (nmol/l). For BLM alone, 11 of 14 cases (71.4%) were measurable; for BLM + EM, nine of 13 cases (69.2%); for BLM + pre-EM, five of 16 cases (31.3%); and for EM alone, three of 13 cases (23.0%). There were significant differences between the three groups (BLM alone, BLM + EM, and BLM + pre-EM) and Mann Whitney’s U test revealed statistical significance between BLM alone and BLM + pre-EM (p<0.01) (fig2).
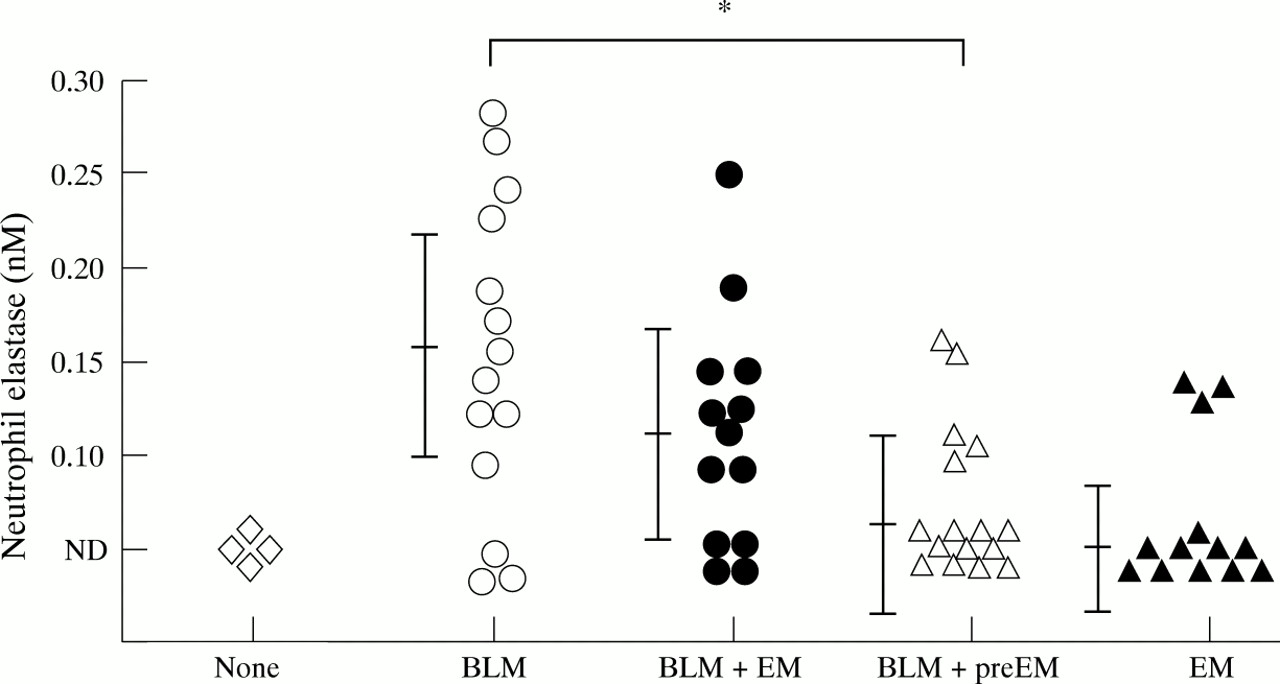
Comparison of neutrophil elastase activity in BAL fluid between groups. The activity of the BLM + pre-EM group was significantly inhibited compared with that of the BLM alone group (*p<0.10). ND = not detectable (<0.10 nM).
HISTOLOGICAL ASSESSMENT OF ACUTE LUNG INJURY
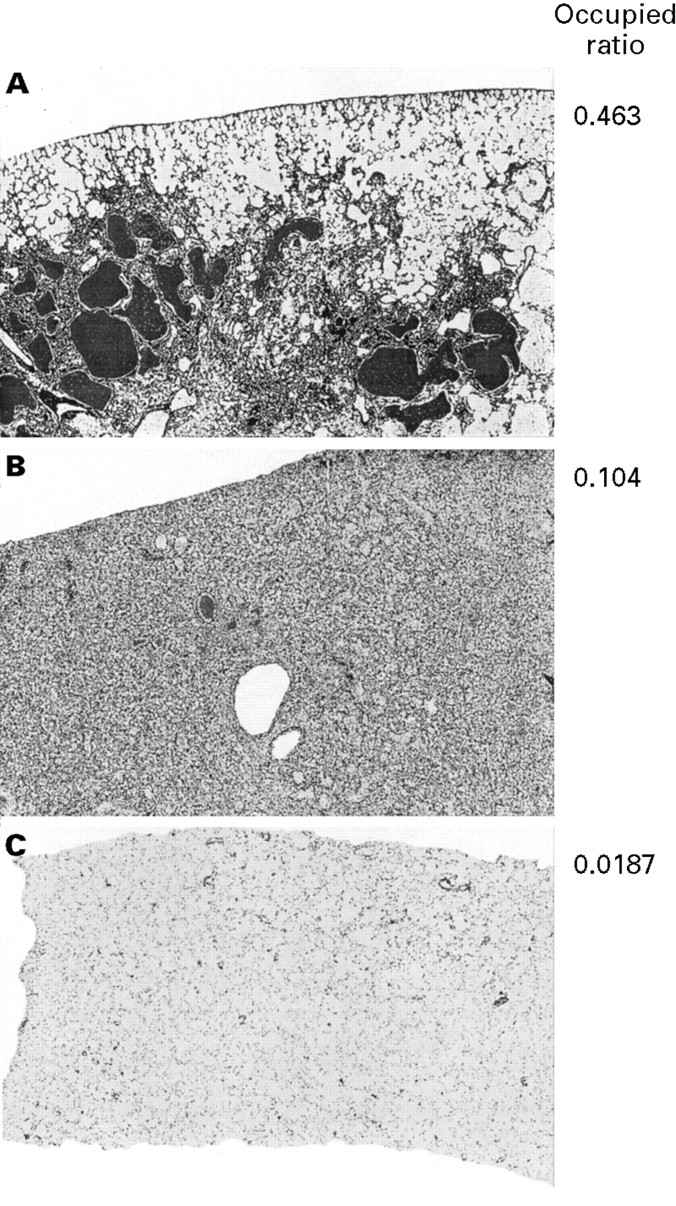
Areas of cell infiltration and oedema were taken as an indication of acute lung injury and were assessed by graphical software Photoshop 3.0J and stained with black colour. The ratio was 0.463 in the BLM alone group, 0.104 in the BLM + pre-EM group, and 0.0187 in the EM alone group (fig 3).

Typical views of pathology graphically modified by Photoshop 3.0J graphic software in (A) the BLM alone group, (B) the BLM + pre-EM group, and (C) the normal saline group. The number of pixels in the area stained black was counted as acute lung injury. The ratio was 0.463 in the BLM alone group, 0.104 in the BLM + pre-EM group, and 0.0187 in the normal saline group. These ratios were decreased in the erythromycin pretreated group.
IL-8 CONTENT IN BAL FLUID
The concentration of IL-8 in the BAL fluid at day 7 after BLM inoculation was 0.692 (0.265) ng/ml in the BLM alone group, 0.429 (0.249) ng/ml in the BLM + EM group, 0.452 (0.305) ng/ml in the BLM + pre-EM group, and 0.389 (0.149) ng/ml in the EM alone group, which were not significantly different (fig 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Median (SD) levels of IL-8 in BAL fluid measured by the ELISA method. The levels were not significantly different (NS) in any of the groups but tended to decrease in the BLM + pre-EM group compared with the BLM alone group.
Discussion
This study analysed the inhibitory effect of erythromycin on bleomycin-induced acute lung injury and found that, by pathological analysis, the most marked changes such as interstitial oedema and infiltration of inflammatory cells into the lung were induced at day 7 following bleomycin treatment.
Pretreatment with erythromycin prior to bleomycin + erythromycin decreased the 2.29-fold increase in total BAL cell count with bleomycin alone to a 1.32-fold increase compared with that with erythromycin alone. The neutrophil ratio in the BAL fluid in the BLM + EM group was 0.444 (69.7/156.9) compared with that of the bleomycin alone group. Furthermore, the neutrophil ratio in the BLM + pre-EM group was 0.106, which indicated that erythromycin caused marked inhibition of neutrophil infiltration into the airway in bleomycin-induced lung injury. An inhibitory effect of erythromycin on neutrophil chemotaxis in patients with chronic bronchitis and diffuse panbronchiolitis has been reported previously.10 16 18 This study suggests a similar mechanism of action for erythromycin since inhibition to neutrophil chemotaxis was related to bleomycin-induced acute lung injury (table 1).
The effect of erythromycin on neutrophil elastase activity was also examined. Neutrophil elastase, in general, increases vascular leakage,19 20 induces neutrophil chemotaxis in tissues,7 and injures bronchial epithelial cells.8 9 In the present study erythromycin significantly inhibited neutrophil elastase activity in the BAL fluid of the BLM + pre-EM group compared with the BLM alone group (fig 2). However, in the BLM + EM group the inhibitory effect of erythromycin on neutrophil elastase activity was not significant despite a 50% reduction of neutrophils in the airway (fig 2, table 1). These findings suggest that erythromycin may have inhibited neutrophil chemotaxis into the airway but did not directly inactivate neutrophil elastase activity in BAL fluid, similar to the erythromycin-induced improvement in chronic bronchial inflammatory disease previously reported.10Erythromycin has been reported to inhibit the release of oxygen radicals from neutrophils, which contributes to the prevention of lung injury.9 19 20 In view of Tamaoki’s report, increased cAMP may also be involved in preventing vascular leakage.29
IL-8, cloned by Matsushima,11 is known to promote neutrophil chemotaxis and may be present in the progressive phase of bleomycin-induced lung injury and fibrosis. In the present study the average IL-8 concentration in the BAL fluid was 0.389 ng/ml in the group given normal saline and 0.692 ng/ml in the bleomycin alone group, which was not significantly different. There were no significant differences between the four groups. Since IL-8 can be released from multiple cell sources (epithelial cells, vascular endothelial cells, interstitial cells and inflammatory cells12 13 ), the distribution of IL-8 in the lung tissue may be complicated. Analysis of the inhibitory effect of IL-8 by the anti-IL-8 antibody will be useful for evaluating the role of IL-8 in bleomycin-induced lung injury. The inhibitory effect of erythromycin on IL-8 production has been confirmed.21 Further studies are needed to elucidate the precise effect of erythromycin on IL-8, whether direct or through other cytokines such as TNF-α or IL-1β.11
In summary, erythromycin inhibited neutrophil infiltration into the airway of rats included in this study. Neutrophil elastase activity was accompanied by inhibition of the neutrophil count, and bleomycin-induced acute lung injury was associated with neutrophil elastase activity. Prior treatment with erythromycin was more effective on bleomycin-induced acute lung injury than simultaneous treatment with erythromycin; however, IL-8 as a strong neutrophil chemotactic factor tended to be reduced by erythromycin but was not significantly different when compared with the bleomycin alone group. Significant inhibition of neutrophil numbers and neutrophil elastase activities in BAL fluid by erythromycin appeared to be less related to the IL-8 content of the BAL fluid.