Article Text

Abstract
BACKGROUND Nitric oxide (NO) plays an important part in the regulation of many physiological functions and may also be involved in several pulmonary diseases. Endogenous NO is synthesised by different isoforms of NO synthase (NOS) from l-arginine.
METHODS The effect of inhaledl-arginine 0.75 g (six normal and six asthmatic subjects), 1.5 g (six normal and six asthmatic subjects), and 3 g (seven normal and six asthmatic subjects) has been studied in a double blind placebo controlled, randomised, parallel group design study. In addition, the effect of a single dose (3 g) of inhaled l-alanine has been assessed in five normal and five asthmatic subjects.
RESULTS l-arginine increased exhaled NO in a dose-dependent fashion with a maximum at 60 minutes. The cumulative effect of l-arginine (3 g) on NO in asthmatic subjects, expressed as the area under the curve in arbitrary units (au) and compared with the effect of placebo (0.9% NaCl), was significantly higher (mean 0.11 au; 95% confidence interval (CI) 0.03 to 0.19) than in normal subjects (0.012 au; 95% CI 0.002 to 0.022). There was a negative correlation (r = –0.72) between the increase in exhaled NO and the fall in forced expiratory volume in one second (FEV1) (0.034 au, 95% CI 0.030 to 0.038) after 3 gl-arginine in asthmatic subjects. Inhalation of 3 g ofl-alanine produced a similar reduction in FEV1(0.033 au, 95% CI 0.007 to 0.059) but no significantly different changes in exhaled NO (0.017 au, 95% CI 0.001 to 0.039) compared with placebo (0.020 au, 95% CI 0.001 to 0.042).
CONCLUSIONS An increase in the amount of substrate for NOS increases the formation of endogenous NO.l-arginine may have therapeutic potential in diseases in which there is defective production of NO, but in asthma it may amplify the inflammatory response in the airways.
- nitric oxide
- l-arginine
- asthma
Statistics from Altmetric.com
Nitric oxide (NO) is a gaseous mediator which plays a key role in the physiological control of the airways and in the pathophysiology of airway diseases.1 It is present in the exhaled air of animals and humans2 3 and the concentration of exhaled NO is increased in patients with asthma4 and bronchiectasis.5 NO may be derived from different cells in the respiratory tract and appears to be involved in a large range of functions including vascular regulation, neurotransmission, host defence, and cytotoxicity.6 Endogenous NO is synthesised from the amino acid l-arginine by the enzyme NO synthase (NOS).6 There are three different isoforms of NOS. Constitutive enzymes (cNOS) have been found in endothelium and neurones7 8 and are activated by a rise in intracellular calcium in response to physiological stimuli.9 An inducible calcium-independent enzyme (iNOS), which may be expressed after induction with cytokines and endotoxin in a number of cell types,6 10 is increased in the airway epithelium of asthmatic patients11 and its expression can be reduced by glucocorticoids.12 In the pulmonary circulation NO is synthesised in endothelial cells by an endothelial NOS (eNOS). Endogenous NO may have a different role in the airways. When produced in small amounts by cNOS activation it may be beneficial in relaxing airway smooth muscle, but it may have deleterious effects when produced in higher concentrations from iNOS. NO is a potent vasodilator and may contribute to the plasma exudation and to the hyperaemia of asthmatic airways.1 On the other hand, high concentrations of NO provide a non-specific defence mechanism in the respiratory tract and it has been shown that knock-out mice that lack the iNOS gene are significantly more susceptible to infections.13 14 l-arginine has been used in the long term treatment of arginine succinase deficiency15 and may also prevent some complications of diabetes mellitus.16 Moreover, it has been suggested that l-arginine improves the impaired coronary microcirculation of hypercholesterolaemic subjects.17 These effects of l-arginine may be due to increased formation of endogenous NO. We have previously shown that oral l-arginine increases exhaled NO in normal subjects.18 Since l-arginine is the substrate for NO synthesis, we have investigated the effect of inhaledl-arginine and another amino acid, l-alanine, which is not a substrate for NOS, on exhaled NO in normal and asthmatic subjects. We also investigated the dose-response relationship between inhaled l-arginine and exhaled NO.
Methods
PATIENTS
Twenty four healthy subjects (14 men) and 23 patients with stable asthma (15 men) were recruited. All were non-smokers who had no history of respiratory or cardiovascular disease and were not receiving long term medication. Patients with stable asthma had positive skin prick tests (>3 mm) for at least two common inhaled allergens and baseline forced expiratory volume in one second (FEV1) was >70% of the predicted. Subjects had increased airway responsiveness, defined as a provocative concentration of methacholine causing a 20% reduction in FEV1 (PC20) of <8 mg/ml. None was using concomitant medication except for on-demand inhaled short acting β agonists. There was no history of upper respiratory tract infection for at least four weeks prior to the study. Subjects did not consume any caffeine for two hours before the l-arginine medication. All subjects gave their written consent to the study which was approved by the ethics committee of the Royal Brompton Hospital.
STUDY DESIGN
Before entering the study all subjects were seen on a screening visit during which a questionnaire, PC20 methacholine, and skin prick tests were performed. The study consisted of two visits separated by an interval of three days. On each study day a single dose of l-arginine (Sigma, Poole, Dorset, UK) was inhaled. Subjects received 0.75 g (six normal, six asthmatic subjects), 1.5 g (six normal, six asthmatic subjects), or 3 g (seven normal, six asthmatic subjects). The three study doses were dissolved in different volumes of normal saline (0.75, 1.5 and 3 g of l-arginine in 10, 20, and 40 ml, respectively) to obtain a concentration of 0.075 mg/ml (pH 5.5, mOsm 664). l-arginine or normal saline control (also in volumes of 10, 20, or 40 ml) was inhaled via an ultrasonic nebuliser (DeVilbiss, Heston, UK; output 4.7 ml/min) whilst wearing a noseclip. An additional group of five normal and five asthmatic subjects inhaled a single dose (3 g) ofl-alanine (Sigma, Poole, Dorset, UK) (pH 5.9, mOsm 836) dissolved in 40 ml of normal saline, or 40 ml of normal saline, during two different occasions separated by an interval of three days. Inhalation delivery was designated time 0 and exhaled NO and FEV1 were measured before medication and then every 30 minutes for five hours. Pulse and supine blood pressure were measured before and 30 minutes after administration of treatment. The study was designed in a double blind, placebo controlled, randomised, parallel group fashion.
EXHALED NITRIC OXIDE MEASUREMENTS
Exhaled NO was measured using a modified chemiluminescence analyser (Logan Research LR2000; Rochester, UK) sensitive to NO from 1 ppb (by volume) to 5000 ppb and with a resolution of 0.3 ppb, which was designed for on-line recording of exhaled NO concentration as previously described.19 In addition to NO, the analyser also measures carbon dioxide (resolution 0.1% CO2; response time 200 ms) and sample pressure and volume in real time. The sampling rate of the analyser was 25 ml/min for all measurements. The analyser was calibrated using certified NO mixtures (90 ppb and 500 ppb) in nitrogen (BOC Special Gases, Guildford, UK). Measurements of exhaled NO were made by slow exhalation (5–6 l/min) from total lung capacity for 15–20 s against a mild resistance to exclude nasal contamination.20 The value corresponding to the plateau of the end-exhaled CO2 reading (5% CO2) was taken as representative of an alveolar sample. In these measurements the pressure during expiration was kept constant (3 (0.4) mm Hg) by using a visual display of expiratory flow measured by pressure and volume sensors in the analyser.
PULMONARY FUNCTION AND METHACHOLINE PROVOCATION TESTS
FEV1 and forced vital capacity (FVC) were measured using a dry spirometer (Vitalograph, Buckingham, UK), the best of three manoeuvres being expressed as a percentage of the predicted value. Airway responsiveness was measured in asthmatic subjects by methacholine provocation challenge. The solution was nebulised with a hand-held nebuliser (Dosimeter MB3; MEFAR Bovezzo, Italy) with an output of 100 μl. The PC20 was calculated by interpolation of the logarithmic dose-response curve.
DATA ANALYSIS
The cumulative effect of l-arginine, placebo, orl-alanine was expressed as the area under the curve. Estimates of difference between l-arginine and placebo orl-alanine and placebo were presented as mean differences with 95% confidence intervals. Comparisons between the groups were made by a paired t test. A p value <0.05 was considered significant.
Results
There was a dose-dependent increase in exhaled NO with a maximal effect at 60 minutes in asthmatic subjects (fig 1B) but not in normal subjects (fig 1A).

Dose-response curve of exhaled NO following inhalation of l-arginine in (A) normal and (B) asthmatic subjects. *p<0.05; **p<0.01.
The cumulative effect of l-arginine (3 g) on NO compared with the effect of placebo (0.9% NaCl) was significantly higher in asthmatic subjects (mean 0.11 au, 95% CI 0.03 to 0.19) than in normal subjects (0.012 au, 95% CI 0.002 to 0.022; p<0.001) (fig 2A). There was a negative correlation (r = –0.72; p<0.01) between the increase in exhaled NO and the fall in FEV1 (0.034 au, 95% CI 0.030 to 0.038) after 3 g l-arginine in asthmatic subjects (fig 2B). Inhalation of 3 g of l-alanine produced a similar reduction in FEV1 (0.033 au, 95% CI 0.007 to 0.059, p<0.05), but no significantly different changes in exhaled NO (0.017 au, 95% CI 0.001 to 0.039) compared with placebo (0.020 au, 95% CI 0.001 to 0.042; p>0.05) (fig 3A and B).
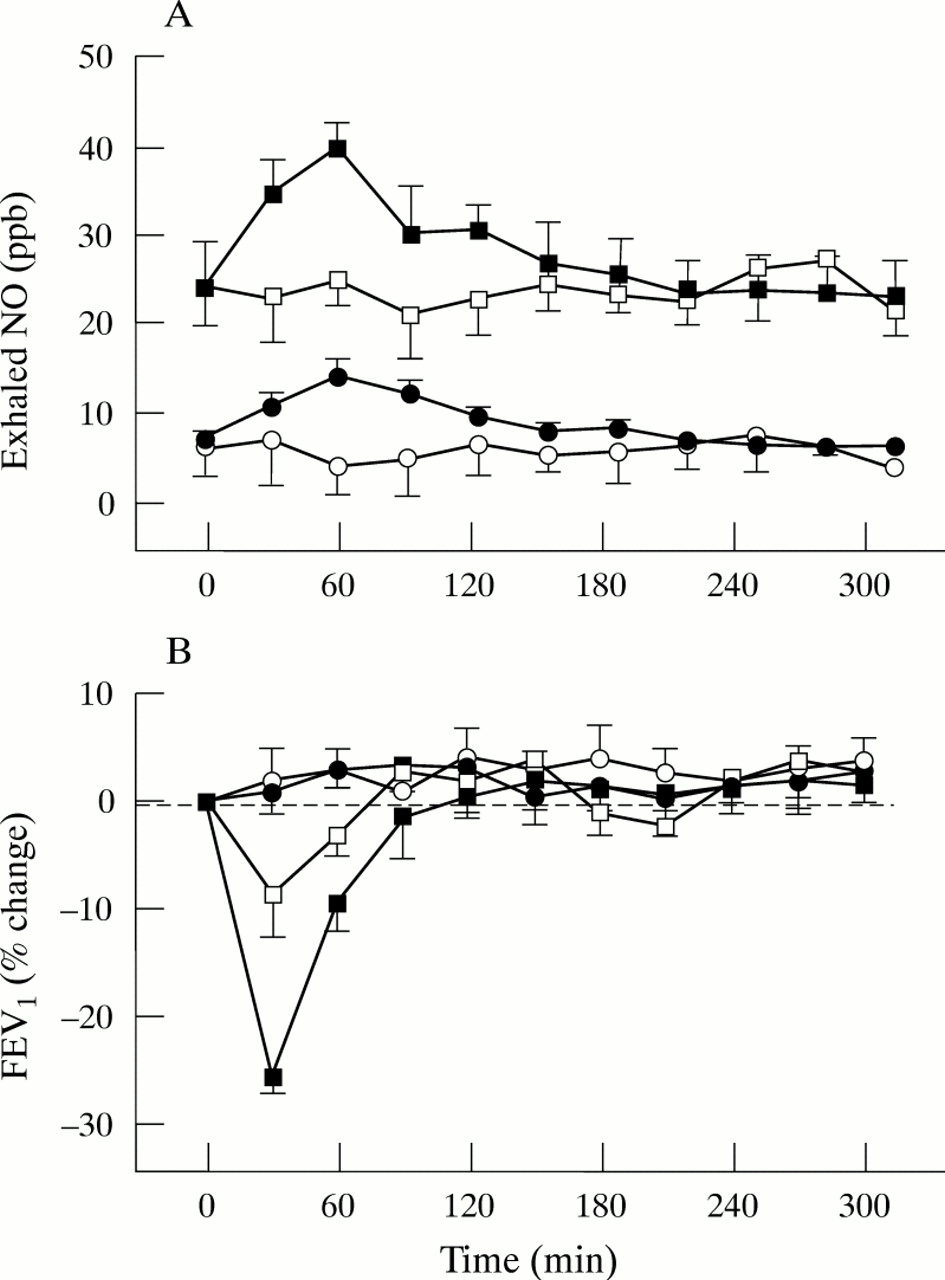
(A) Exhaled NO and (B) FEV1 following inhalation of l-arginine 3 g in normal (•) and asthmatic subjects (•) or saline in normal (○) and asthmatic subjects (□).
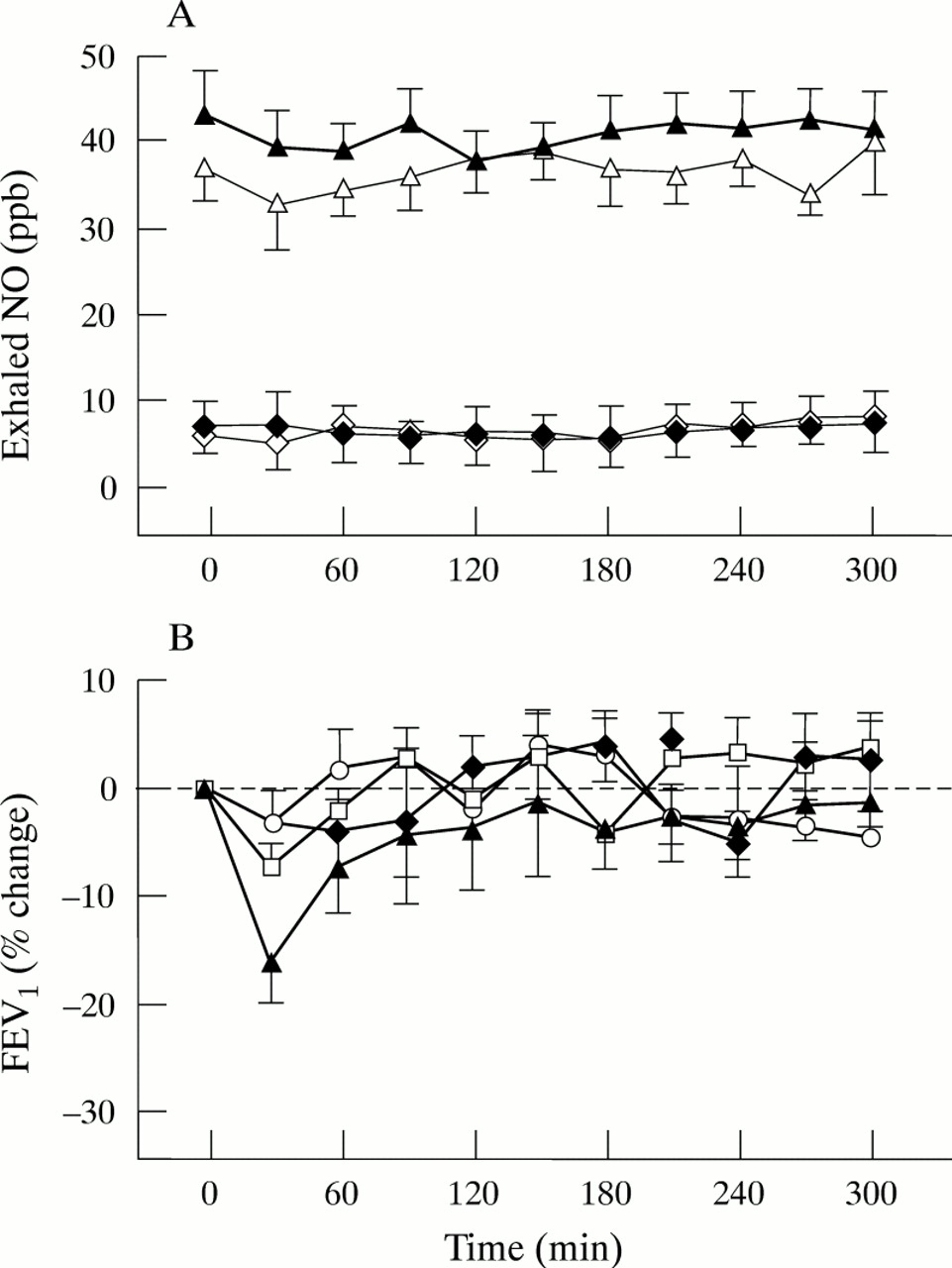
(A) Exhaled NO and (B) FEV1 following inhalation of l-alanine (3 g) in normal (♦) and asthmatic subjects (▴) or saline in normal (⋄) and asthmatic subjects (▵); p<0.05.
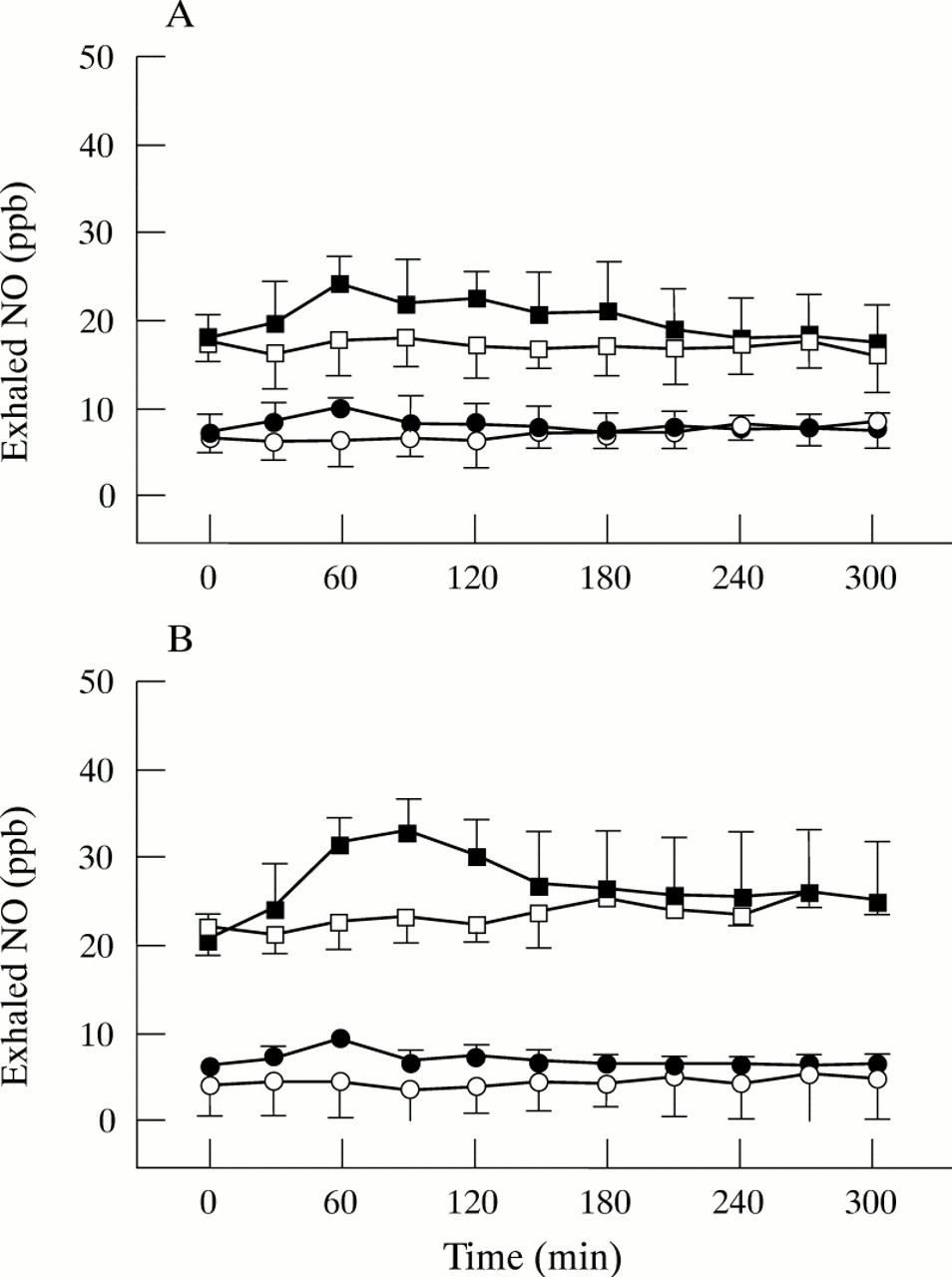
The pattern of NO change following 0.75 g and 1.5 gl-arginine was the same as for the highest dose (fig 4A and B). There was no significant change in FEV1 afterl-arginine administration at these two doses (1 (2.1)% and –10 (3.4)%, respectively, p>0.05).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Exhaled NO following inhalation ofl-arginine 0.75 g (A) and 1.5 g (B) in normal subjects (●) and asthmatic subjects (•) or saline in normal subjects (○) and asthmatic subjects (□); significance of difference from saline:*p<0.05, **p<0.01.
Discussion
Our study shows that inhaled l-arginine induces a significant increase in exhaled NO in normal and asthmatic subjects suggesting that there is evidence of a change in the activity of endogenous NOS in response to increased availability of substrate. The increase in exhaled NO was dose-related in asthmatic subjects but not in normal subjects and was also more significant in asthmatic subjects than in normal subjects. This may reflect differences in sensitivity of endogenous NOS to different doses of l-arginine between normal and asthmatic subjects. The increased exhaled NO in asthmatic patients is likely to be due to increased expression of iNOS which has a greater utilisation of l-arginine than constitutive enzymes as it results in greater NO production. The increase in exhaled NO was maximal at 60 minutes after administration ofl-arginine by inhalation. The main source of NO is not yet certain but there is some evidence to suggest that high concentrations of NO are formed in the nasopharynx21 and this may be related to the high density of blood vessels in the nasal mucosa. NO may be also derived from the airway epithelium, the alveoli (epithelium or endothelium), or inflammatory cells such as macrophages. Previously we have reported that the increased levels of NO found in patients with asthma are derived predominantly from the lower respiratory tract.19 Moreover, we have shown that the administration of a non-selective NOS inhibitor, l-NAME, by nebulisation to normal and asthmatic subjects produces a fall in exhaled NO levels while the more selective iNOS inhibitor, aminoguanidine, reduces exhaled NO only in patients with asthma. This suggests that the high levels of NO in patients with asthma may be attributable to induction of NOS.22 iNOS is expressed to a greater extent in the airway epithelium of patients with asthma than in normal subjects23 and iNOS induction may be inhibited by glucocorticoids whereas cNOS is unaffected.24 25 Our finding that exhaled NO can be increased by l-arginine suggests that it is possible to increase the NOS activity in normal and asthmatic subjects by increasing the availability of the substrate.
NO may have an important role in asthmatic subjects in amplifying the inflammatory response in the airways.1 The bronchoconstriction observed after l-arginine may be produced by a direct effect of NO on the permeability of blood vessels. It has recently been reported in an in vitro study that when iNOS is expressed the increased production of nitric oxide enhances airway plasma leakage, suggesting an important role for NO in the inflammatory process that occurs in diseases such as asthma.26 High NO concentrations may have toxic and even cytotoxic effects mediated by the formation of peroxynitrite radicals27 which may contribute to airway inflammation.
Since the increase in exhaled NO following l-arginine inhalation is more pronounced in asthmatic subjects than in healthy controls, there is a possibility of essentially reduced substrate availability in asthmatics compared with healthy subjects.
There may also be a non-specific inflammatory component to bronchoconstriction since l-alanine also caused a significant fall in FEV1 (but of less magnitude than withl-arginine). The increase in endogenous NO production was not associated with any measurable change in blood pressure or heart rate, suggesting that the increased formation was insufficient to affect the systemic circulation. Previous studies ofl-arginine infusions have reported conflicting results.l-arginine induced a modest hypotensive effect in normal subjects after intravenous administration. This effect has been related to increased NO formation in systemic endothelial cells.28In contrast, it has been reported that low dose intravenousl-arginine has no effect on systemic blood pressure or peripheral perfusion29 ; however, a higher plasma concentration of l-arginine does reduce blood pressure and increase heart rate.30
In summary, our data demonstrate that NO is endogenously produced within normal and asthmatic human airways and this production can be increased by the availability of the substrate. However, high levels of NO may contribute not only to airway obstruction but also to airway hyperreactivity observed in subjects with asthma. The increased production of NO by l-arginine may be useful in diseases in which there is defective production of NO.
Acknowledgments
We thank the British Lung Foundation for their support.