Article Text
1995 Review and Position Statement

Statistics from Altmetric.com
The first British guidelines on asthma management were published in 1990 after a joint initiative between the British Thoracic Society, the Royal College of Physicians of London, The King’s Fund Centre, and the National Asthma Campaign.1 ,2 It was intended that they should be regularly reviewed and they were updated in 1992 with guidelines on the management of asthma in children also included. The revised guidelines were published in 1993 as a supplement to Thorax 3 and the summary charts appeared simultaneously in the British Medical Journal.4 That revision included a number of areas of controversy and listed areas of uncertainty which required further research.
The Guidelines Coordinating Committee (see below for list of participants), representing the Standards of Care and Education Committees of the British Thoracic Society and the National Asthma Campaign, and in liaison with the Audit and Research Unit of the Royal College of Physicians of London, met in early 1995 to discuss whether a further revision of the Guidelines was necessary. In addition to the areas of controversy noted in 1993, the Coordinating Committee identified a number of areas where new work had been undertaken and where review might be necessary. These areas were circulated to all members of the 1992 Guidelines Committee (consisting of paediatricians, general practitioners, chest physicians, general physicians, Accident and Emergency physicians, and nurses) who were asked if they wished to take part in a review of the Guidelines and if they agreed with the list of topics for review. Those who no longer wished to take part were replaced by participants with similar professional backgrounds. Individuals were then identified to write background papers on the areas for review and these were circulated to all members for comment. Finally, all participants came together for two days at the Royal College of Physicians of London on 29 and 30 June 1995 to discuss these background papers and to agree the summary statements. This paper represents a summary of this process and is intended to be read in conjunction with the 1993 Guidelines3 as many important issues included in those Guidelines remain unchanged and are equally valid today. The Coordinating Committee envisage that the next revision will be needed in 1997/8 when the Guidelines will be completely rewritten and, wherever possible, remain evidence based.
Note on terminology
Throughout this paper use of the word “infant” implies someone aged less than 12 months, “preschool” someone less than five years of age, and “schoolchildren” refers to children aged five years and over. For most of this position statement and revision, schoolchildren and adults are considered to require a similar therapeutic approach.
Participants
Professor JG Ayres,† Professor PJ Barnes,† D Bellamy, CE Bucknall,† PS Burge, F Carswell, RA Clark, R Clifford, JB Clough,† GM Cochrane,† JM Couriel, GK Crompton, SR Durham,† P Ebden, MW Elliott,† JAR Friend,† R Green,‡ BDW Harrison,* † JPR Hartley, DP Heaf,† BG Higgins, AM Hilton,* Professor ST Holgate,† WF Holmes, PW Ind,† KP Jones, D Keeley, H Kurz,‡ DJ Lane,† ML Levy, BW Lloyd, D Luyt,‡ UM MacFadyen, SA McKenzie,† E Neville, RG Neville,† CLP O’Callaghan,† RL Page, MR Partridge,* MG Pearson, JC Pounsford,† Professor NB Pride, RN Rivington,‡ M Rudolf,* NR Ruggins, G Russell,† DP Ryan, Professor M Silverman,* Professor AE Tattersfield,† AH Thomson, JGB Thurston, MJ Ward,† Professor JO Warner,† JV West, AJ Williams, N Wilson,† E Wooler.
Before the meeting all participants provided a listing of sources of funding from pharmaceutical or other relevant commercial interests.
*Member of Coordinating Committee; †prepared background paper; ‡observer.
Asthma in adults and schoolchildren
Diagnosis and differential diagnosis
The description of asthma given in the 1993 Guidelines3 remains valid Correct diagnosis of the condition is essential. If the variable nature of airway narrowing which is characteristic of asthma cannot be demonstrated by any other means, then in adults and older children a trial of high dose oral steroids with peak flow monitoring for a minimum of two weeks is essential. If patients who do not have asthma are treated according to the asthma guidelines and fail to improve, there is a danger that they may be treated with progressively higher doses of drugs such as systemic steroids with increased risk and little benefit. Whilst there is overlap between asthma and chronic obstructive pulmonary disease (COPD) related to smoking, they are different diseases with differing aetiologies, pathologies, natural histories, and responses to treatment. The British Thoracic Society is preparing separate guidelines for the management of COPD. Diagnostic confusion or failure to respond to treatment are indications for referral to a specialist.
In every clinical presentation with wheezing, breathlessness, or airway obstruction the health professional should consider:
(1) is this localised obstruction of the airways (e.g. cancer, foreign body, post tracheostomy stenosis, vocal cord dysfunction with wheeze), orgeneralised airway obstruction?
(2) if generalised, is it asthma (predominantly reversible) or chronic obstructive pulmonary disease (predominantly irreversible), or a combination of the two, or one of the more unusual causes such as bronchiectasis, obliterative bronchiolitis, or cystic fibrosis?
Asthma in the elderly
Asthma is frequently underdiagnosed in the elderly because of a wider differential diagnosis, difficulty with measurement of lung function, and under-reporting of symptoms.5 The latter may occur because of reduced expectations or because of an age related reduction in perception of breathlessness.6 A similar age related difference in the physical signs associated with severe asthma may lead to underestimation of severity and undertreatment.7 Simple tests of mental functioning may be necessary to ensure that elderly people with asthma are capable of acquiring the necessary skills for treating and monitoring their condition.8 Anticholinergic bronchodilator therapy may have a slightly greater role in this age group than in younger patients.9
Therapeutic issues
USE OF SHORT ACTING β2 AGONISTS
As bronchodilators are primarily intended to provide symptom relief and because of a possible link between asthma deaths and high doses of β2 agonists, there seems to be no reason to change the current recommendations. Patients should be encouraged to use the minimum dose of β2agonist to control their symptoms on an as required basis.
INDICATIONS FOR LONG ACTING INHALED β2 AGONISTS
At the present time, step 3 of the guidelines recommends the use of high dose inhaled steroids for those whose asthma is not controlled on low doses. However, they do include the possibility of the use of long acting inhaled β2 agonists plus low dose inhaled steroids for those who have problems with high dose inhaled steroids, or for those who have persistent night time symptoms despite otherwise good control. The use of long acting inhaled β2 agonists is currently limited to step 4. However, in the light of recent studies10 it is now recommended that low dose inhaled steroids plus salmeterol be regarded as an alternative to the use of high dose inhaled steroids as step 3 treatments. If the long acting bronchodilator option is chosen, it should only be continued if there is demonstrable evidence of benefit. More study is required on the relative merits of these two step 3 options.
ANTIMUSCARINIC AGENTS
No change is made to the recommendation in the current guidelines that inhaled anti- muscarinic drugs (ipratropium bromide or oxitropium bromide) may be used as regular maintenance bronchodilator therapy in step 4 patients who already require high dose inhaled steroids.
INHALED STEROIDS
The majority of patients taking inhaled steroids are on low doses at which side effects of any sort are unlikely. In all children height should be carefully measured on a regular basis. Impaired growth is one of the signs of uncontrolled asthma as well as being a potential side effect of steroid therapy. In those on higher doses of inhaled steroids, studies of side effects are often confounded by previous or concomitant use of oral steroids. In those with more severe asthma the risk versus benefit of high dose inhaled steroids is clearly more favourable than oral steroids. There is evidence that all of the inhaled steroids are absorbed to some extent from the lung11 ,12 and hence will have some systemic activity. Although this is small compared with oral prednisolone, the precise long term effect on conditions such as osteoporosis is uncertain. It is prudent therefore, as with all treatment, to give the lowest dose of inhaled steroid compatible with asthma control.
There is no indication at the present time for routine investigation of, or prophylactic treatment for, osteoporosis in patients on low dose inhaled corticosteroids. In patients receiving high dose therapy (⩾1000 μg beclomethasone or budesonide/day or ⩾500 μg fluticasone/day) general measures to counteract osteoporosis (such as regular exercise, hormone replacement therapy, smoking cessation, adequate dietary calcium) should be considered. More long term follow up data are needed for patients on long term high dose inhaled steroids.
Inhaled fluticasone propionate has become available in the UK since the last revision of the BTS guidelines. Its clinical efficacy and safety have been extensively documented. Fluticasone is as effective as beclomethasone dipropionate and budesonide at half the dose when given by equivalent delivery systems.13-16 At equipotent doses fluticasone may have the potential for producing similar systemic effects to those of beclomethasone and budesonide. Fluticasone should be included in the guidelines as an alternative inhaled steroid at half the doses recommended for beclomethasone and budesonide when given by metered dose inhaler (MDI).
In addition to differences in oral bioavailability, all currently available inhaled steroids are also absorbed systemically from the lungs11 ,12 and there is increasing evidence that the delivery system is an important determinant of the systemic effect of inhaled steroids. The detection of systemic effects depends on the sensitivity of the indices used to detect them.
Systemic effects may be reduced by the use of a large volume spacer with an MDI or with mouth washing without swallowing, or with a dry powder inhaler. The Turbohaler delivers approximately twice as much inhaled steroid to the lung17 and doses should probably be halved when this device is used but, as in all cases, dosage should be titrated against control of asthma and treatment reduced when control is achieved.
Although local and systemic side effects show a relationship with increasing dose, it has often proved difficult to demonstrate clear dose responses to the therapeutic (anti-asthma) effects of inhaled steroids in controlled clinical trials. However, in clinical practice improved asthma control can often be achieved by increasing the dose.
Current guidelines recommend that patients should double the dose of inhaled steroids temporarily if their asthma deteriorates or at the first sign of an upper respiratory tract infection. There are no published trials which have specifically addressed this question, but the recommendation should be retained though controlled studies are needed.
There are no published controlled trials of the effectiveness of nebulised budesonide in adults.
(See also section on “Gaining control and the stepwise approach to management” below.)
CROMOGLYCATE AND NEDOCROMIL
It is recommended that the current guidelines for the use of cromoglycate and nedocromil in adults and schoolchildren should remain unchanged.
THEOPHYLLINE
Current guidelines recommend theophylline in addition to high dose inhaled steroids at step 4, and as an option for a minority of patients at step 3. The additional possibility of using low dose theophylline for its anti-inflammatory action as a step 2 treatment needs further study before it can be recommended.
ANTILEUKOTRIENES
Leukotriene receptor antagonists and synthesis inhibitors have been shown to have a range of potentially beneficial pharmacological properties,18-23 but more studies are needed to provide comparative data against established therapies before any positioning recommendation can be made.
INHALED COMBINATION THERAPY
The use of formulations which combine fixed doses of anti-inflammatory agents and short acting β2 agonists is not generally consistent with the recommendations for minimising use of reliever inhalers laid down in the guidelines.
There is surprisingly little information on the relative benefits of bronchodilator combination inhalers and their individual constituents or other treatments, and there are few data on compliance, patient preference, or pharmaco- economics. Definitive pronouncements regarding the positioning of combination inhalers are therefore not possible.
INHALATION DEVICES
(i) New propellants
Whilst granted temporary “essential use” exemption from the Montreal Protocol, chloro- fluorocarbon (CFC) propellants will be phased out of use in metered dose inhalers within the next few years. Replacement propellants will be formulated with most of the existing medicines over the same time period. In changing patients from old to new inhalers it is important that the patients understand that the CFCs in the old inhalers were environmentally damaging and not harmful to the individual. Patients need to be forewarned that their new inhaler may have a different appearance, feel, and weight compared with their old inhaler and, when activated, the spray may have a different taste and impact differently on the oropharynx. However, they should be reassured that trials have shown the new CFC-free inhalers to be safe and effective. No dosage adjustment is necessary for salbutamol reformulated with the new propellants, but this may not apply when inhaled steroids and other drugs are reformulated.
(ii) New devices
A number of new inhalation devices are now available and limited data on lung deposition are available for some of them. Patient preference and cost should be taken into account when choosing an individual device.
(iii) Metered dose inhalers versus dry powder inhalers
Patient preference is of major importance in choice of device. Many patients are unable to use MDIs correctly and, even with good inhaler technique, only 10–15% of the dose is delivered to the lungs. This can be improved by the addition of a spacer device which will reduce coordination problems, but the amount of drug delivered from such devices may vary greatly.
Some patients prefer dry powder inhalers but there are variations in deposition ranging from 10% to 30%. Inspiratory flow rates also cause variation with the same device.
All children and adults on high doses of inhaled steroids from a metered dose inhaler (beclomethasone or budesonide ⩾1000 μg/day or fluticasone ⩾500 μg daily) should take them through large volume spacer attachments which increase lung deposition and reduce oropharyngeal deposition.
(iv) Correct use of large volume spacer devices
Inhalation from a spacer device should take place as soon as possible after actuation since the half life of drug aerosol within the spacer is often less than 10 seconds. Single dose actuation is recommended. The device should be washed, rinsed, and dried in air once a week and not wiped dry as this increases the electrostatic charging of spacers and reduces drug delivery. Spacer devices need to be replaced every 6–12 months.
(v) Nebulisers
Advances in other drug delivery systems, especially the use of MDIs with a large volume spacer (with or without face mask attachment), may obviate the use of nebulisers in many clinical situations.
Nebulisers vary greatly in the droplet size they produce, their nebulisation time, and drug output and this may have a significant effect on the therapeutic response. Different drugs nebulised within the same nebuliser, under identical conditions, will not necessarily have identical output characteristics. All nebuliser and compressor combinations and all ultrasonic nebulisers should have their output characteristics determined for all drugs used.
Whilst small variations in delivery of bronchodilator may not be critical, it is essential that information is available on the large differences in dosages that patients are likely to receive from some nebulisers. For example, changing from a conventional continuous emission nebuliser to one which delivers nebulised drugs only during inspiration may more than double the amount of drug reaching the lungs.
Current ultrasonic nebulisers do not nebulisedrug suspensions such as budesonide effectively and until newer models are evaluated they should be avoided for this task. British Thoracic Society guidelines on current best practice for nebuliser treatment are currently in preparation and will provide further information. Advice regarding selection of patients for nebulised therapy is given in the 1990 and 1993 guidelines.1-3
(vi) Generic substitution/bioequivalence
The general assumption is that generic preparations have bioequivalence with branded products. There is little published evidence to support or refute this. The way in which equivalence is demonstrated is an issue to be taken up by the regulatory authorities and a consensus statement on determining equivalence of inhaled medications has recently been published.24
ALLERGIC AND ENVIRONMENTAL ISSUES: NON-PHARMACOLOGICAL TREATMENTS
There is clear evidence that passive smoking exacerbates childhood asthma and that removal from exposure leads to improved outcomes. Maternal smoking during pregnancy and during the infant’s early life is clearly associated with an increased prevalence of wheezy illnesses in the young.25 Other reasons for the increasing prevalence of asthma are not known. Increased early life exposure to indoor aeroallergens,26 reduced exposure to infections,27 and changes in diet28 are all possible factors. The role of outdoor pollution is controversial but it is unlikely to be a major factor in the increased prevalence of asthma,29 although high levels of pollution may worsen symptoms in those with asthma. In those with established asthma avoidance of house dust mite allergen by means of bed covers has proven efficacy in the short term.30-32 Other measures such as acaricides remain unproven.33 Careful allergy histories should be taken from all those with asthma, and skin prick testing with relevant allergens can be helpful in defining atopy and in support of the removal of domestic pets, especially cats,33 or the introduction of bed covers. Support for house dust mite avoidance measures reflects a change to the 1993 guidelines but further research into methodology and duration of action of these measures is needed.
Occupational asthma is an important cause of adult asthma, accounting for 1–2% of cases. An occupational history must be taken from all those with asthma. Symptoms which improve on days away from work or on holiday suggest occupational asthma and indicate the need for further investigation with objective measurement and specialist referral. If the link is proven then early removal from exposure to an occupational sensitiser is associated with a better long term outcome. Patients with suspected occupational asthma should not be advised to cease work until the diagnosis is proven and until all methods of reducing exposure at the work place have been explored. Specialist respiratory physicians, occupational physicians, and employers will all need to be involved in this process.
Gaining control and the stepwise approach to management
The importance of gaining control of asthma is re-emphasised, abolishing symptoms as soon as possible and optimising peak flow by starting treatment at a level likely to achieve this. This approach is most likely to gain and maintain the patient’s confidence in the treatment and the health professional, and enhance compliance with treatment and outcome. Current understanding of the mode of action of steroids would support a strategy of starting with oral steroids or moderately high dose inhaled steroids.34-36 Once control is achieved the dose of steroid can be reduced. It is therefore recommended that many patients who need anti-inflammatory therapy should be started on inhaled steroids in a dose of 400–500 μg twice daily for beclomethasone or budesonide, or 250 μg twice daily for fluticasone (half these doses for younger schoolchildren). Once control is achieved, treatment should be reduced in a stepwise manner. When control is not achieved, diagnosis and treatment should be reviewed.
Stepping down the dose of inhaled steroids once asthma is controlled has been emphasised in current guidelines but is often not implemented, with the result that many well controlled patients are overtreated with inhaled steroids. The reduction in inhaled steroids should be slow as patients deteriorate at different rates when steroids are withdrawn. Reduction in dose should be monitored by symptoms and peak flows, including frequency and severity of exacerbations, and β2agonist use. It is recommended that reductions should take place every 1–3 months by decreasing the dose of inhaled steroid by approximately 25–50% at each step. Some patients may come off inhaled steroids completely. When stepping down treatment in patients on inhaled budesonide there is some evidence to suggest that once daily treatment may be effective.
Patients, partnership and psychosocial issues
PATIENT EDUCATION AND GUIDED SELF MANAGEMENT PLANS
Giving information alone does not alter behaviour, but written and audiovisual reinforcement of spoken messages aids patient confidence. All patients should be given information about features which indicate when their asthma is worsening, and what to do under those circumstances. Giving those with asthma written self management plans so that they may adjust treatment to keep themselves well reduces morbidity and health costs.37 ,38
These recommendations represent a change from the 1993 revision in that there is now definite evidence of benefit from patient education and the issuing of self management plans, but exactly who needs them and what form they should take (number of action levels, thresholds for intervention) remain an area for further research.
In young schoolchildren such plans are based on symptoms; the results of peak flow monitoring should be interpreted with caution and can miss clinically meaningful falls in lung function.39 In older children and in adults peak flow monitoring as part of their management plan is recommended for those who are poor perceivers of symptoms, those with brittle or life threatening asthma, and to monitor the effects of changes in treatment and to determine the significance of changes in symptoms. Such plans should also be given to all who have been admitted to hospital because of severe asthma and to those on step 3 and above of the treatment guidelines.
There is a need in the UK for standardisation of peak flow meters.40
PSYCHOSOCIAL ISSUES
Despite improvements in medication and the beneficial effects of guidelines, potentially preventable asthma morbidity continues and some psychosocial factors have been identified which may be important.
Depression, anxiety and denial of disease are associated strongly with asthma deaths,41-43 near deaths,44 and acute asthma requiring attendance at the Accident and Emergency department. These associations may not necessarily be causal.45 Other associations include life crises, family conflict, and social isolation.43 Factors that may reduce compliance with medical advice remain largely unknown but seem to include those factors associated with asthma deaths with, in addition, shame, anger, and high risk life styles such as smoking and alcohol abuse.46Their association with poor compliance is weak, and many of these different factors may have to interact for true association with poor compliance to be determined. Failure to attend asthma education programmes is again associated with anxiety, depression, and denial and also with low socioeconomic group, minority ethnic groups, illiteracy, and occupational asthma.47
When asthma proves difficult to control on usually effective therapy it is important to find out about any family, psychological, or social problems which may be interfering with effective management. In schoolchildren and young people poor supervision of treatment by parents may be associated with unnecessary morbidity. School examinations, parties or outings may also need anticipatory increases in treatment.
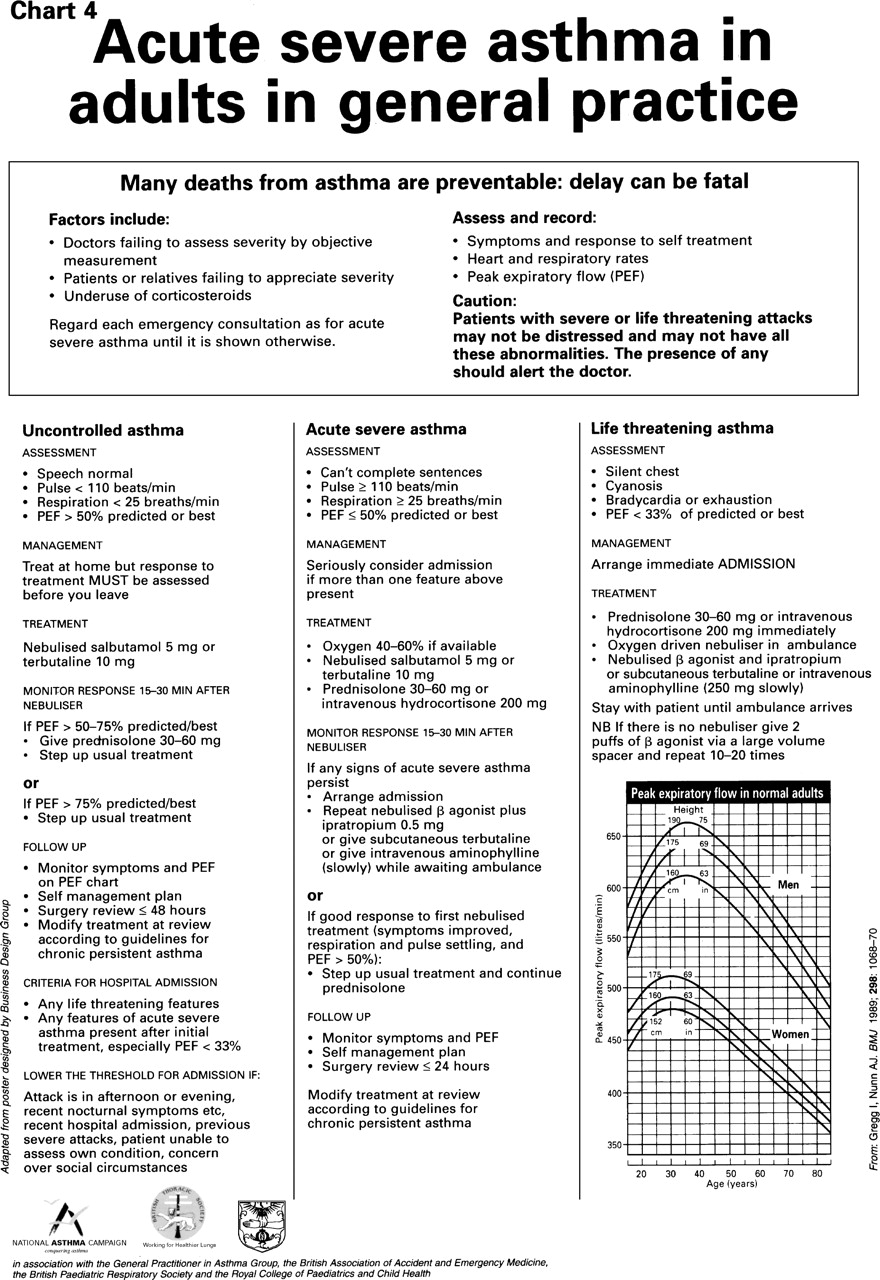
Acute severe asthma
PEAK FLOW CRITERIA FOR ADMISSION AND DISCHARGE
Peak expiratory flow (PEF) measurements must be interpreted in the light of other features of severity and the patient’s past history, particularly previous admissions to hospital, attendance at Accident and Emergency departments and current treatment, especially corticosteroids.
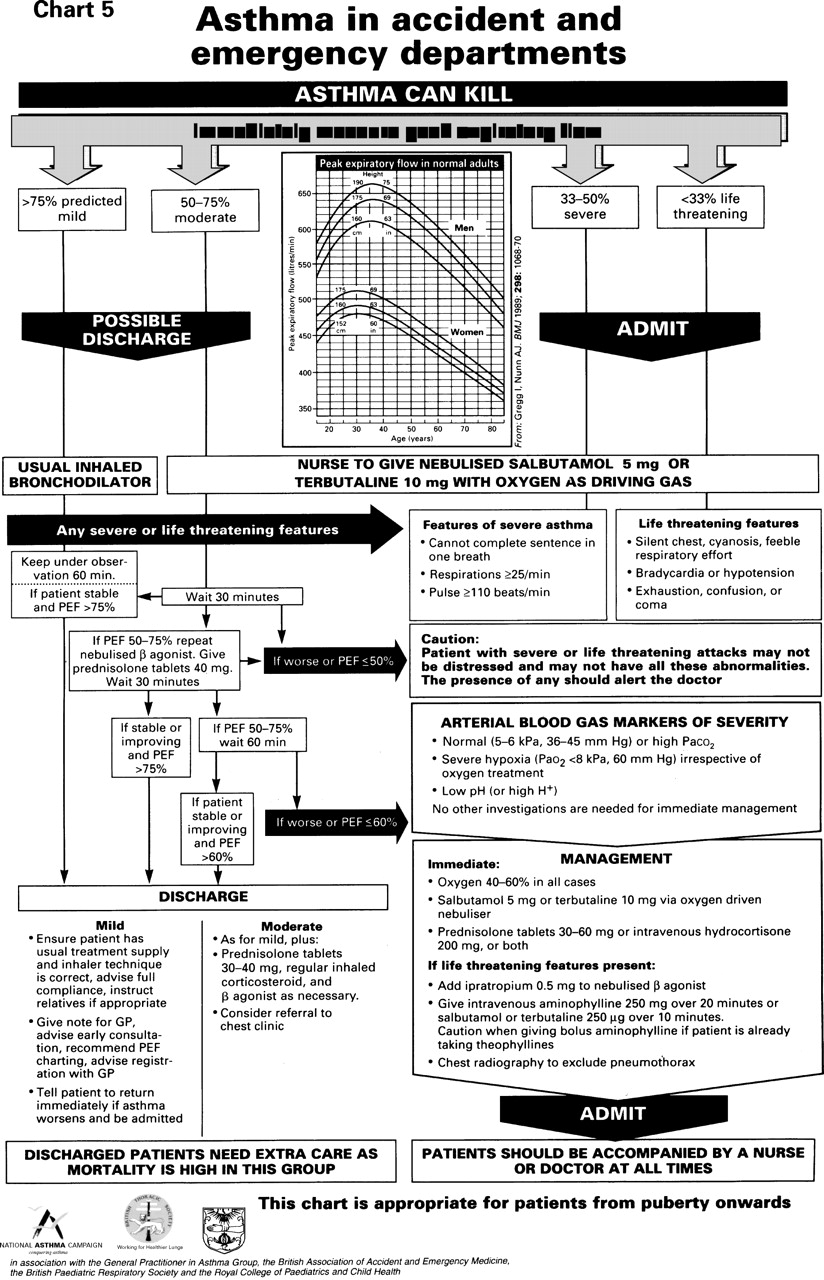
There are no new data to suggest that the previously agreed PEF guidelines on when to admit should be changed. The 33% figure is based upon published evidence.48 The 50% figure is arbitrary but widely accepted49 and supported empirically by the BTS audit.50 The guidelines do not take into account the patient’s previous history but previous hospital admissions or attendance at Accident and Emergency departments are important risk factors for readmissions51-53 and death.54Similarly, there is a difference between a patient with a PEF of 50% who has been on prednisolone for a week and a patient who has a short history and has not yet started oral steroids.
There is no evidence to support changing the PEF criteria for discharge. Despite a small study showing that most patients who were discharged without meeting BTS criteria suffered no ill effects provided that they had received education from a specialist chest liaison nurse and were discharged on oral and inhaled steroids,55 the very large BTS audit showed that patients with diurnal variation of >25% were at an increased risk of requiring early readmission.50
PULSUS PARADOXUS
Pulsus paradoxus need not be measured as it adds nothing to the assessment.56
PLACE OF PULSE OXIMETRY
Facilities for the monitoring of oxygen saturation should be available in all clinical areas that treat patients with acute asthma.
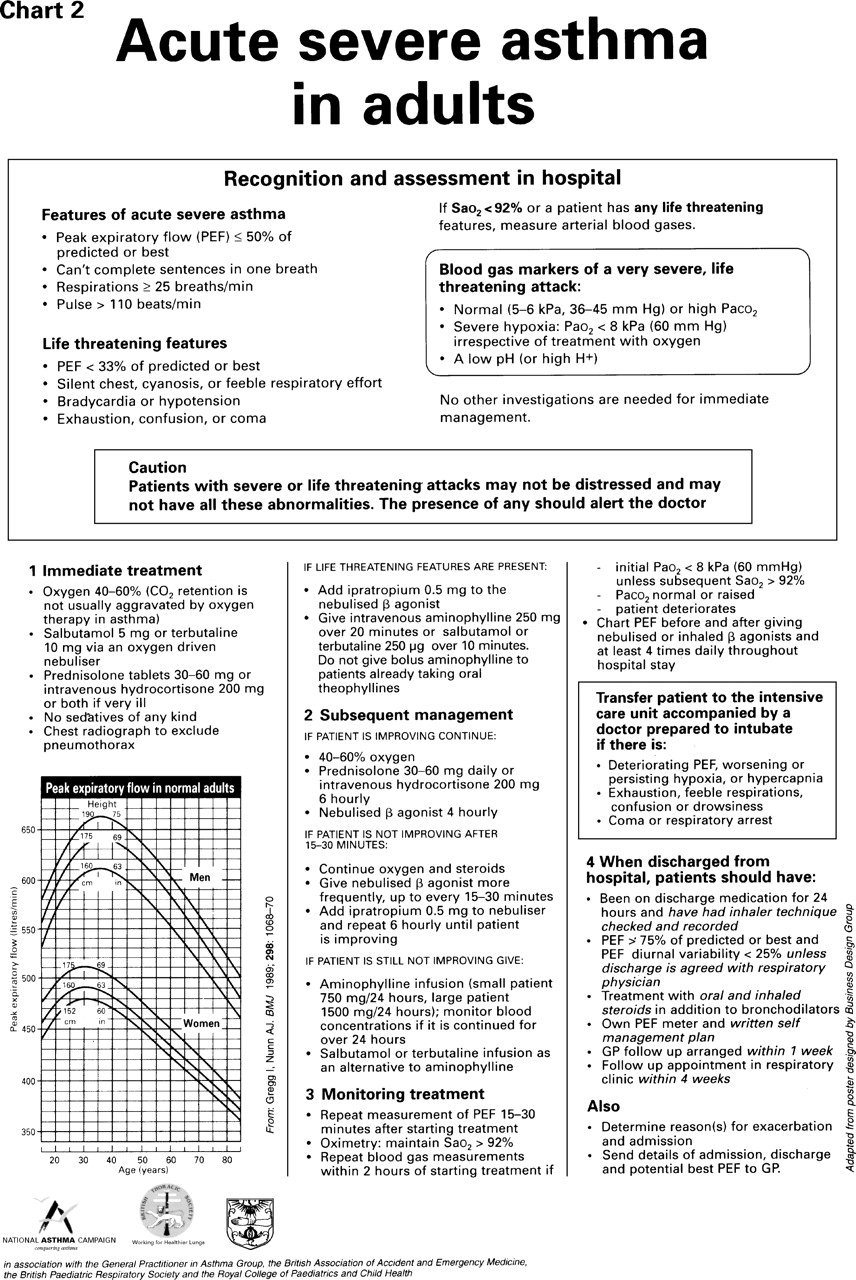
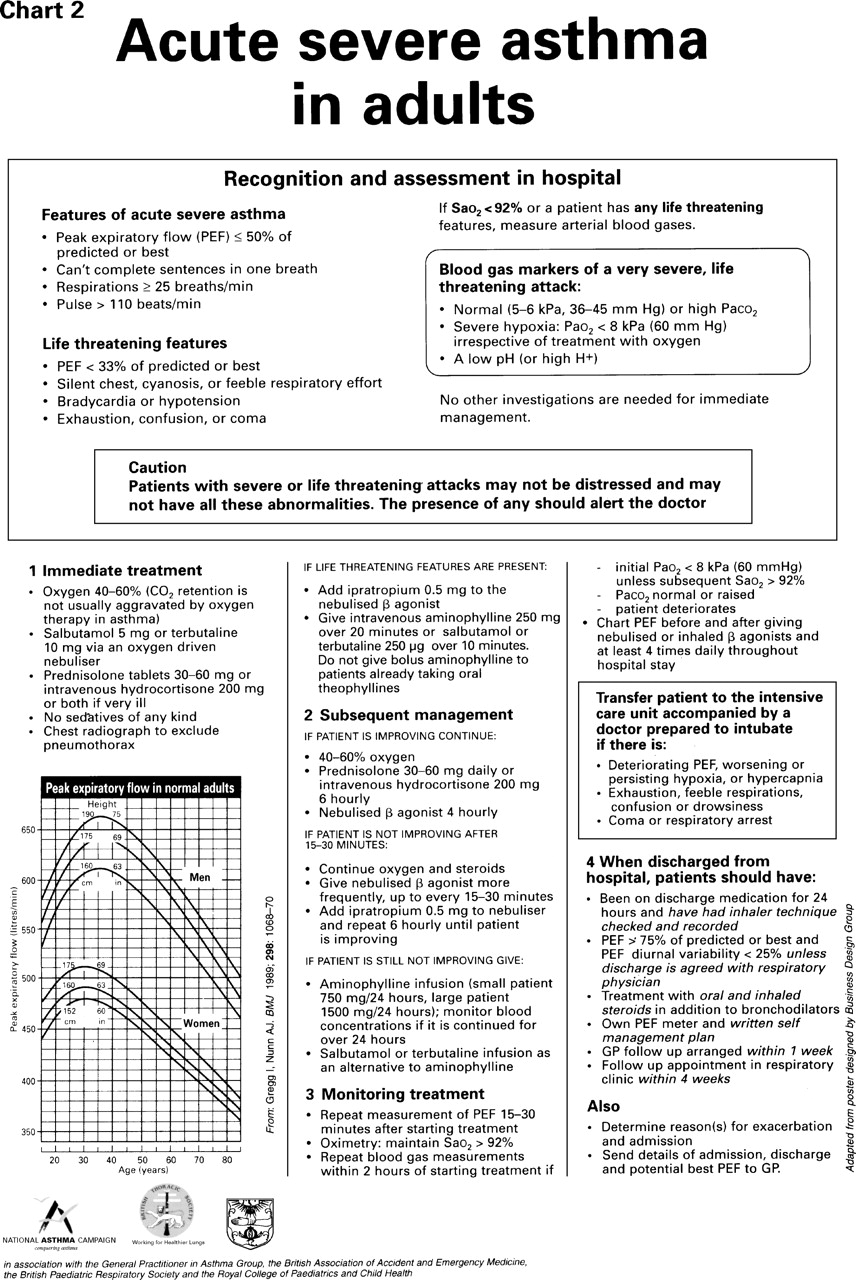
Interpretation of saturation in patients who are on, or who have recently been on, oxygen treatment is difficult, but in patients with an Sao2 of ⩾92% and no features of an imminently life threatening attack (PEF <33% predicted of best, silent chest, cyanosis, feeble respiratory effort, bradycardia or hypotension, exhaustion, confusion or coma), it is reasonable to defer arterial puncture.57 However, arterial blood gas tensions must be measured if there is any evidence of deterioration.
IPRATROPIUM BROMIDE IN ACUTE ASTHMA
Nebulised ipratropium bromide 0.5 mg should be added to other standard treatment for patients with life threatening asthma or those whose asthma fails to improve on standard therapy since most,58-62 but not all,63 ,64 short term studies have shown more rapid increases in PEF in patients given the combined treatment. Nebulised salbutamol and ipratropium can also be safely given by general practitioners and by ambulance crews to patients with life threatening asthma, but this should not defer or delay transfer to hospital. However, there are insufficient data from studies lasting more than a few hours65 to recommend the addition of ipratropium to other patients with acute severe asthma, and there are insufficient data to recommend the precise point at which ipratropium should be discontinued after anacute episode. More research, including data at 24 and 48 hours after admission and on length of hospital stay, is required.
DISCHARGE ARRANGEMENTS AND FOLLOW UP
No studies have been performed to determine when patients who do not require regular nebulised treatment at home should be changed from nebulised bronchodilators in hospital to bronchodilators delivered by their usual inhaler device.
The guidelines currently recommend that all patients discharged from hospital following an acute attack of asthma should be followed up by their general practitioner within one week and by a specialist respiratory physician within one month. This is a vulnerable time for patients but resources do not always permit these arrangements for follow up, and research is needed to determine whether specialist follow up (hospital or community) is associated with better outcomes or whether other alternatives are possible.
WHEN AND HOW TO STOP A COURSE OF ORAL STEROIDS AFTER AN EPISODE OF ACUTE SEVERE ASTHMA
Empirical observations suggest that:
-
A dose of 30–40 mg prednisolone daily should be continued until the patient’s acute severe asthma has completely resolved—as determined by no nocturnal disturbance, the ability to perform daytime activities normally, and peak flows which have returned to the patient’s best levels (within 80% of the patient’s highest value).
-
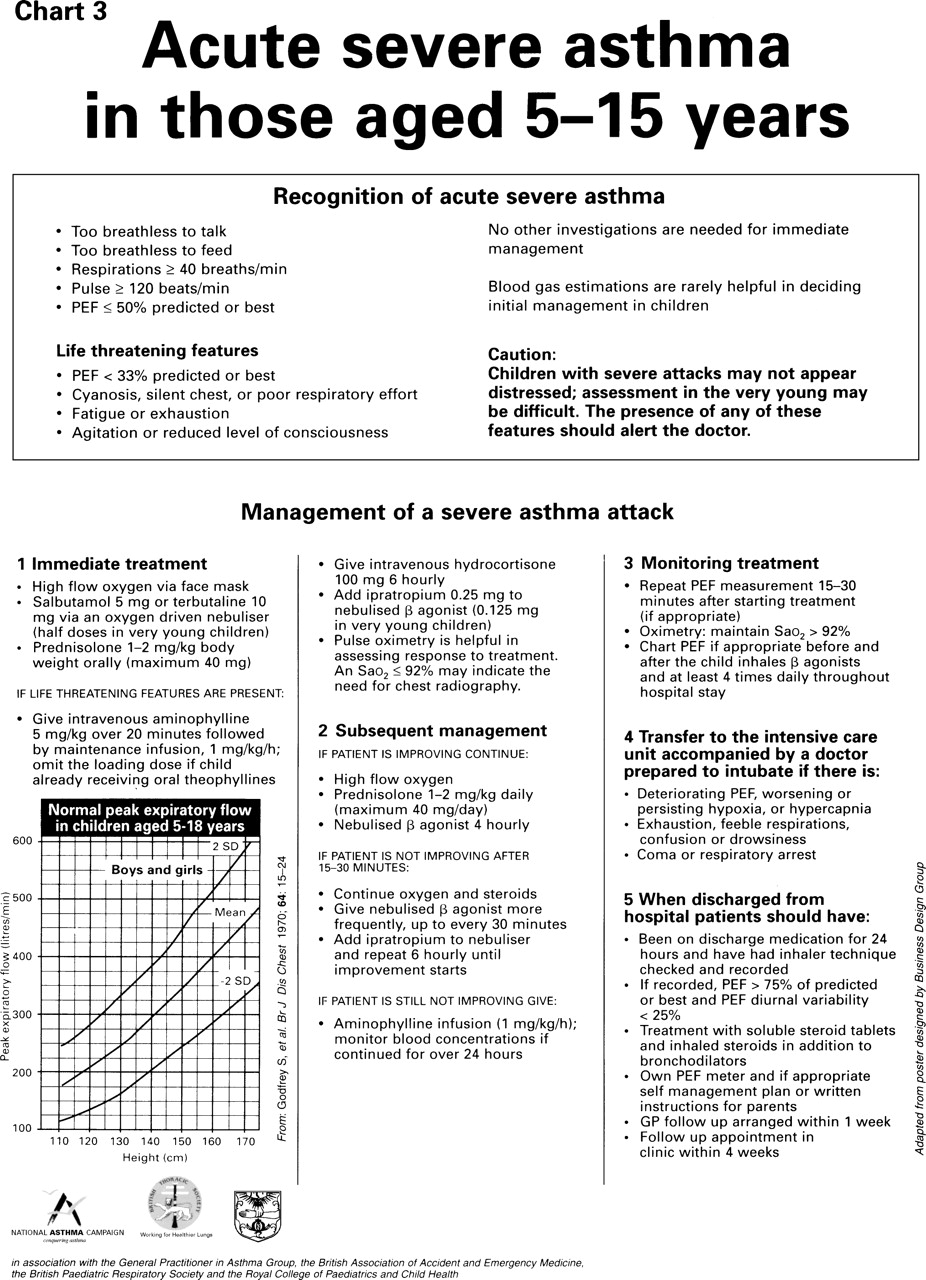
The rate of recovery is variable and steroid doses should be adjusted according to the severity. Doses of 30–40 mg/day in adults for up to three weeks are safe66 in most patients and treatment can be stopped either abruptly67 or tapered off if the patient is not on long term oral steroid therapy. Prednisolone should not be stopped (nor the dose tapered) if the patient’s asthma is deteriorating subjectively or objectively. In schoolchildren failure to respond to a four day course of steroids (prednisolone 30–40 mg daily) should lead to a review of the diagnosis.
In view of the therapeutic and management changes which have occurred since the 1993 guidelines were published, the modified summary charts for the management of asthma in adults and schoolchildren are reprinted on pages S11–15.
Organisational issues
THE ROLE OF GUIDELINES
There has been no detailed study of the effectiveness of asthma guidelines but studies in other fields suggest the likelihood of benefit. Development and publication alone are not sufficient and successful implementation is likely to involve ownership, active education of health professionals, incorporation into patient documentation, involvement of patients, and feedback to health professionals of how their behaviour compares with the recommendations in the guidelines. Local task forces or asthma planning teams are necessary to enhance implementation.
SPECIALIST VERSUS GENERALIST CARE
(i) Inpatients
Audit has shown that specialist care of adults admitted with asthma is associated with improved outcomes.68 ,69 In children there is evidence that improved outcomes can be associated with improved training and use of guidelines.
Other possible methods of providing care include:
-
Admission under a generalist onto a specialist respiratory medical ward and transfer to specialist care on the next day (this option is rarely available in paediatric departments).
-
Generalist care in line with guidelines agreed by the local respiratory physician or paediatrician with special responsibility for respiratory illness on either a general ward or a respiratory ward.
-
Generalist care plus a visit from a respiratory physician or specialist paediatrician.
-
Generalist care plus guidelines plus a visit from a respiratory nurse.
It is unknown whether these alternatives have similar high quality outcomes to specialist care; their relative costs are also unknown.
(ii) Outpatients
There is no evidence to justify altering the recommendations in the current guidelines that those with asthma who require hospital outpatient attendance should be seen in a respiratory medical specialist clinic or a paediatric asthma clinic.
SEVERITY, OUTCOME MEASURES, AND AUDIT
(i) Definitions of severity
-
Treated patients. The guidelines currently define severity in terms of the treatment step needed to control symptoms, maintain lung function, and allow normal life. Other guidelines have used ad hoc categorisations which have not been validated and, in the absence of new evidence, it is therefore recommended that the current operational definition of severity should be “the treatment step needed to maintain good, or best possible, control in terms of symptoms, lifestyle and lung function”.
-
Untreated patients. Untreated symptomatic patients are, by corollary, best regarded as poorly controlled and should be categorised by the treatment needed to maintain (not achieve) control, as above. Untreated asymptomatic patients with normal lung function should be categorised as being on step 0 treatment.
(ii) Severity measures
Severity scores, which might allow cate- gorisation on the basis of characteristics other than symptoms or treatment, are currently being evaluated. As a physiological outcome and severity measure, percentage of best function corrects for the degree of irreversible airflow obstruction and is independent of treatment step.70 It is valuable for individual patients by providing a realistic gold standard, and—providing best function is assessed in a standard manner after adequate treatment with anti-inflammatory and bronchodilator medication—it also allows results of groups of patients to be compared in a meaningful way. It is therefore recommended as a physiological measure which gives important information about severity and outcome.
(iii) Outcome measures
The outcomes currently recommended in the guidelines are described in terms of symptoms, degree to which normal life is disturbed, PEF and, for hospitals, readmission rates. As noted above, percentage of best function (where the best value is that predicted for many patients with the measure automatically taking account of this) is recommended as the standard physiological outcome measure. There is a need to validate a standard method of assessing symptoms which could then be recommended for widespread use, readily applicable to general practice, but the desired outcomes are clinically valid and there is no new evidence to support any change to them.
(iv) Audit
In hospital, audit should be of the process of asthma care in adult patients and in those of school age, since there is currently no outcome measure which reflects the quality of care. The BTS audit tool71 allows assessment of eight criteria.
-
PEF recorded on admission
-
Arterial blood gases measured in patients with Sao 2 <92%
-
Systemic steroids administered within one hour of attendance
-
PEF serially recorded so that variability can be calculated
-
Inhaled steroids prescribed on discharge
-
Oral steroids prescribed on discharge
-
Follow up appointment planned
-
Self management plan given
Readmission rates merit further investigation as an outcome of health care.50 In ambulatory care (hospital outpatient practice and primary care) there is a pressing need for the identification of auditable criteria for the management and control of asthma.
In general practice audit will include:
-
an asthma register
-
an ability to determine the frequency of attendance with asthma
-
information on the prescribing of both preventative and relieving medication
-
information on outpatient referral rates and admissions to hospital
-
agreed strategies for coping with patients at risk of developing severe attacks or showing features which are recognised associations with asthma deaths.
AMBULANCE SERVICES
Ambulance personnel should have specific training in the care of acute asthma. They need to be able to recognise asthma and to grade its severity. Protocols should include measurement and recording of PEF before and after nebulised treatment.
SCHOOLS
Each Health Authority should liaise with all education authorities and establishments to ensure that each school has an asthma policy and that the presence and implementation of this policy is checked by the Schools Inspectorate. The school health service can help children with asthma by ensuring that teachers, governors, parents, pupils, and doctors are agreed about the treatment of asthma, and the Children’s Charter emphasises that children with asthma can expect to have access to their inhalers at school. It is important for local Health Commissions and Education Authorities to work together to develop clear policies on how asthma should be managed in schools.
ACCIDENT AND EMERGENCY DEPARTMENTS
These require clearly written management protocols along the lines of the BTS recommendations. Patients with acute asthma must be treated in the most urgent manner.
GENERAL PRACTICE SERVICES
In addition to following the recommendations in the BTS Guidelines, nurses and doctors involved in asthma clinics need appropriate training with regular updates. Asthma clinic nurses should have been on a recognised asthma training course and District Health Authorities should set a target for this with a recommendation that all of the nurses involved in asthma care should have been on a formal evaluable training course. A system for regular meetings and liaison, perhaps led by a local respiratory nurse specialist, should be in place, as determined by the local Asthma Task Force.
HOSPITAL SERVICES
Adults and children who require hospital outpatient care, including those recently discharged from hospital following a severe attack of asthma, should all be seen by doctors and nurses with appropriate special interest and training. In addition to following the good practice recommended in the guidelines, such services will provide facilities for educating patients and their families about asthma and contact with at least one respiratory nurse with special responsibilities for asthma (including nurses in general practice and school nurses). Regular joint meetings between these groups are encouraged.
CONTRACTING WITH PURCHASERS: WHAT CONSTITUTES A GOOD ASTHMA SERVICE?
Providers of asthma care should contract to:
-
Prevent asthma attacks
-
Reduce asthma morbidity
-
Reduce asthma mortality
To achieve this the delivery of care must include primary care, hospital respiratory specialists (both adult and paediatric), and Departments of Public Health and local Education Authorities. There must be good communication between the specialist centre and the other groups involved, with the specialist centre often acting as a resource for knowledge and training as well as providing direct patient care.
Good practice as recommended in the BTS Guidelines should be followed.
Asthma in children under five years of age
Diagnostic issues
The pathophysiological term “chronic inflammatory condition” to describe asthma may be inappropriate in very young children. There are a number of patterns of lower airway disease and it might be more appropriate to consider the management of early childhood asthma in relation to the two predominant clinical patterns—acute wheezy episodes and recurrent day to day symptoms—which may occur separately or together in any child. There is evidence that acute viral wheezy episodes in the very young72-74 represent a type of airway disease clinically distinct from atopic asthma. There are major difficulties in the use of the term “asthma” in infants (under one year of age) and it is acceptable to refer to “wheezing illness” or “infantile asthma” in order to avoid entering a major area of disagreement, namely the definition of asthma in very young children.
There is also evidence that the individual clinical patterns may require different therapeutic approaches in young children.75-77 Lumping acute episodes with recurrent day to day symptoms is inappropriate in defining the severity or control of asthma. When the diagnosis of asthma is in doubt—for instance, when the major or only symptom is chronic cough—a positive response to a therapeutic trial of β2 agonist and/or inhaled corticosteroid therapy may help to identify the disease as stated in the 1993 guidelines. There is, however, no evidence that early diagnosis or treatment affects the long term prognosis of asthma in children under the age of five. Both diagnosis and treatment should be kept under regular review.
A number of research questions remain to be resolved. It is possible that separate terminology describing wheezing disorders of infants and young children may be required to differentiate them from atopic asthma. Further research on clinical and laboratory markers may help to identify these disorders in individual patients—something which is not possible at present. There are few valid short or long term outcome measures for use in this age group. The criteria for defining asthma in the presence of chronic or recurrent cough have not been adequately defined.
Management plan
DRUGS
Preventative treatment with sodium cromoglycate or low dose inhaled corticosteroids for troublesome asthma in early childhood is safe and effective, and the short term benefits certainly exceed any possible side effects in almost all children. Sodium cromoglycate is rarely effective for wheezing in infants under the age of one year, with the exception of those born prematurely,78 and it is not effective for very young children with acute episodes. The precise place of inhaled corticosteroids has yet to be clarified in children with intermittent wheezing episodes alone, but this group of drugs is effective in children with chronic or daily wheezing. The long term side effects of treatment in early childhood are as yet unknown. There is, however, concern that by treating very mild cases with inhaled steroids, the balance of risk/benefit may be adverse.79 For such children, sodium cromoglycate should be considered as first choice preventative treatment. The relative merits of newly introduced inhaled corticosteroids compared with those of long standing remain to be demonstrated.
There are no clinical trials of long acting β2 agonists in the management of preschool children. It seems reasonable, however, to introduce this treatment at step 3, rather than using high dose corticosteroids in the first instance.
MANAGEMENT OF CHRONIC ASTHMA
The recommendations are given in Chart 6 on pp S16–17. There is disagreement among paediatricians as to whether or not sodium cromoglycate should be introduced as a separate step, prior to low dose corticosteroids, and the issue has yet to be addressed by a good controlled study. It is also not known whether in this age group two or three doses daily are as effective as four doses per day.
When inhaled steroid therapy is introduced (new step 2) it is important to gain control quickly, but there is no evidence to favour either a stepwise increase in steroid dose (say, at 10–14 day intervals) or a high starting dose followed by a stepwise decrease when control is achieved. The choice is optional but the point of entry into Chart 6 (that is, step 2 or 3) should be determined by the severity of symptoms at the time.
A number of therapeutic questions remain
to be resolved including the role of long acting
β2 agonists, the efficacy of doubling preventative agents, the role of long acting theophylline in view of its reported anti-inflammatory actions, and the dose-response effect of inhaled corticosteroids (which has a bearing on the decision to step up or down with the introduction of inhaled steroids). No data are available on the dose of inhaled agents which reaches the lungs. There are few reliable measures for evaluating outcome in individual children.80 The effects of inhaled steroids on lung growth in infants should be investigated.
MANAGEMENT OF ACUTE EXACERBATIONS
For the child who has mild or moderate acute symptoms in a community setting (wheeze and cough with chest tightness and mild dyspnoea, but without distress, speech or feeding difficulty or cyanosis) a management protocol is given in Chart 7. The role of prednisolone in infancy has not been established. If there is progressive deterioration or if signs of severe airway obstruction develop (Chart 8), referral to secondary care is indicated.
DRUG ADMINISTRATION
The move away from a nebuliser to an MDI with spacer (with face mask for the very young or ill coordinated child) is reflected in Table1 and Chart 7. There is no evidence that small volume spacers are more effective than those of large volume; the choice depends mainly on convenience, compliance and parental choice. Doses and dose intervals are extremely variable; because of the inefficiency of small volume spacer devices, adult doses are often used in infancy (Table2).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Choice of inhaler devices for young children
Recommended starting doses and dose intervals for children under 5 (maximum doses and minimum dose intervals for domiciliary use in brackets)
References
Linked Articles
- Editorial