Article Text

Statistics from Altmetric.com
Wei Qin, pulmonologist and pulmonary vascular interventional radiology specialist
A 72-year-old female patient was admitted because of dyspnoea and continuous cough lasting 5 months. She denied fever, chest pain and gastrointestinal symptom. She had undergone successful coronary stent implantation and percutaneous closure of the atrial septal defect 8 years ago. There was no history of venous thromboembolism, cancer, gastro-oesophageal reflux disease, asthma, allergic rhinitis or other allergies.At presentation, the patient’s temperature was 36.7 ℃ with a heart rate of 74 bpm, blood pressure of 110/60 mm Hg, respiratory rate of 21 bpm and oxygen saturation of 89% on room air. Chest auscultation revealed no abnormal findings, no wheezes and no moist rales. Cardiac examination revealed regular rhythm without murmur; there was no oedema and varicosities in both lower extremities.
Ziyang Zhu, pulmonologist and pulmonary vascular interventional radiology specialist
D-dimer levels were normal on admission. Thrombophilia-related indicators, including antinuclear antibodies, lupus anticoagulant, protein C and protein S, were within normal limits. Ultrasound of the lower extremity showed no intravenous thrombosis. Cardiac ultrasound showed normal-sized atria and ventricles, no visible masses and only a small amount of tricuspid regurgitation. Pulmonary artery CT angiography (CTPA) demonstrated multiple filling defects in bilateral pulmonary arteries (figure 1A) and the plugging device (figure 1B). In the absence of a mass on cardiac ultrasound, the right atrial shadow, attached to the occlusion device, was thought to be caused by turbulent blood flow (figure 1B, white arrow). A small amount of mucus-like material and a small piece of greyish tissue were aspirated by using a catheter to aspirate the lesion in the pulmonary artery (figure 1C, video 1).
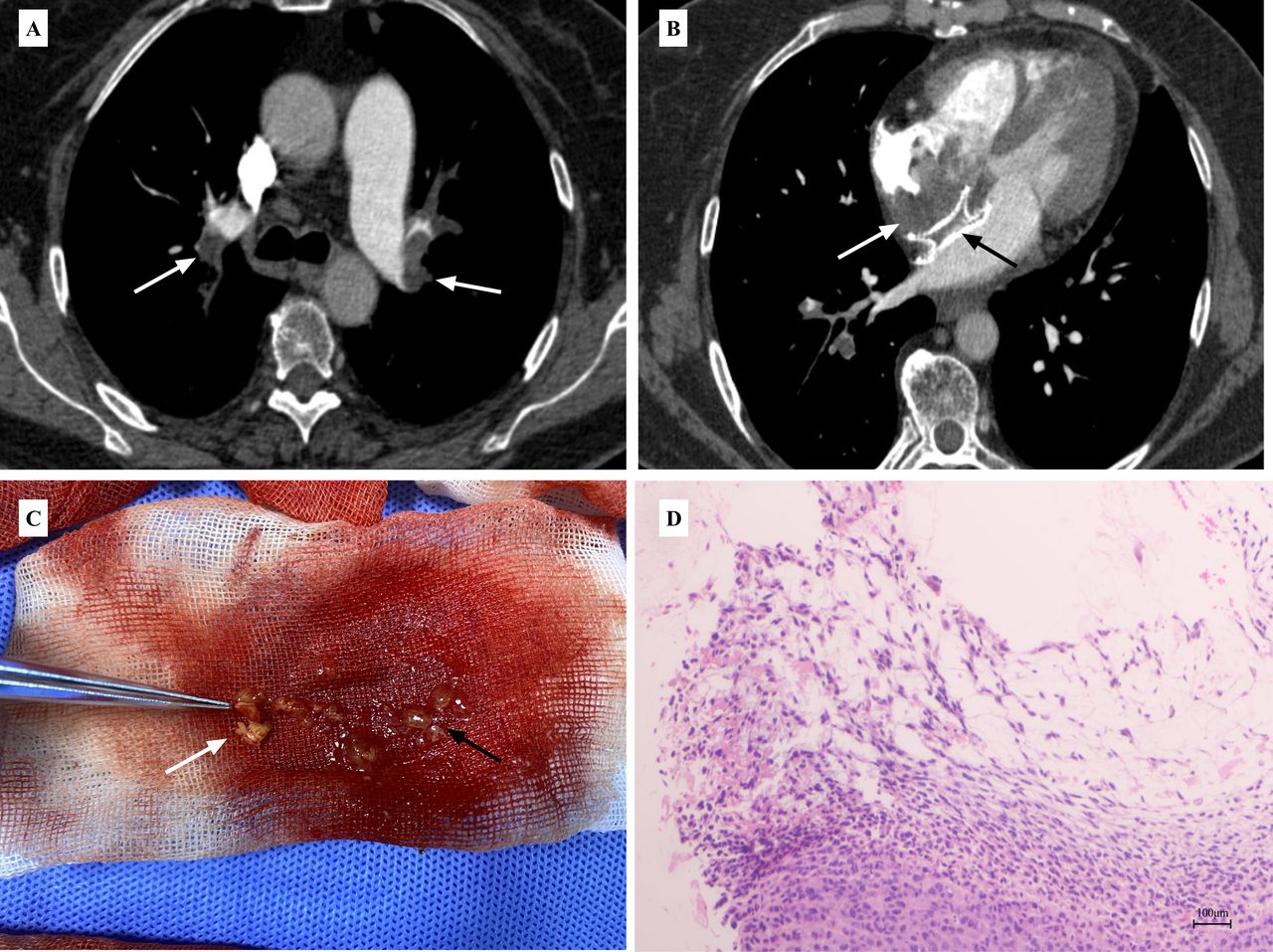
(A,B) Multiple filling defects in bilateral pulmonary arteries (white arrows); Suspicious low-density shadow (white arrow) on the right atrial side of the atrial septal blocker (black arrow). (C) Aspirations of mucus-like material (black arrow) and a small piece of greyish tissue (white arrow) in the pulmonary artery. (D) Tumour cells exhibited pleomorphism, mainly cylindrical and long spindle shapes (H&E, 100×).
Disclaimer: this video summarises a scientific article published by BMJ Publishing Group Limited (BMJ). The content of this video has not been peer-reviewed and does not constitute medical advice. Any opinions expressed are solely those of the contributors. Viewers should be aware that professionals in the field may have different opinions. BMJ does not endorse any opinions expressed or recommendations discussed. Viewers should not use the content of the video as the basis for any medical treatment. BMJ disclaims all liability and responsibility arising from any reliance placed on the content.
Qiong Liu, pathologist
Subsequent histopathological findings showed scattered tumour cells entangled in a large amount of myxoid stroma, which showed a diversity, that is, cylindrical and long spindle shapes. Immunohistochemical results showed positive for CD 31 and pan-cytokeratin, partially positive for S-100, CD 34 and a low calretinin positivity of 1%–2%, and on the contrary, negative for cytokeratin 5/6 (figure 1D, online supplemental figure S1 A-E).
Supplemental material
Shi Chen, pulmonologist
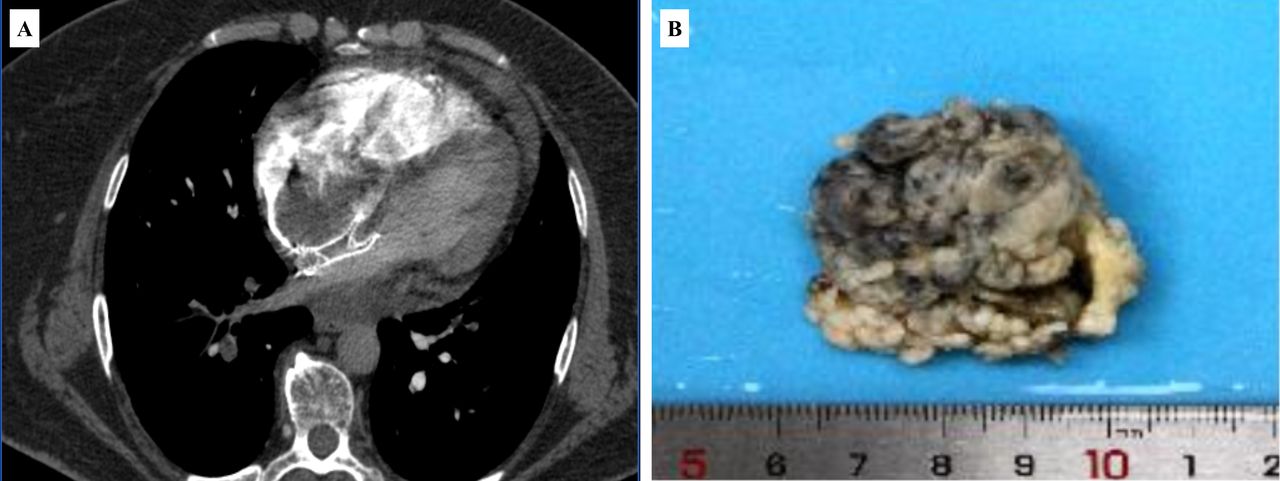
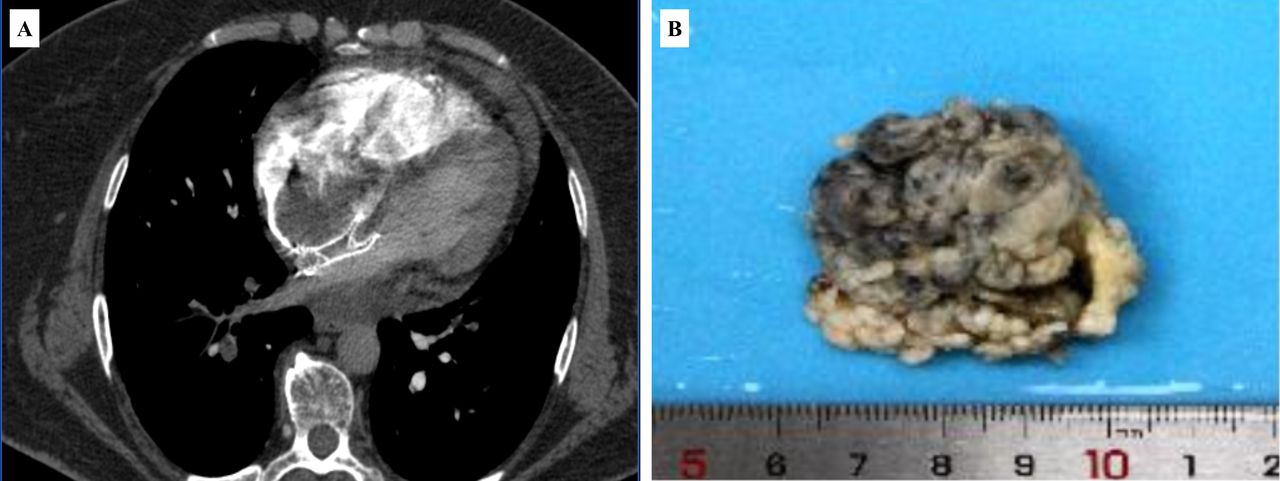
She was then diagnosed with pulmonary artery myxoma embolisation but she refused to receive further treatment and was then given rivaroxaban 15 mg Q12H and switched to 20 mg every day after 3 weeks. Forty-five days after anticoagulation therapy outside the hospital, the patient experienced a sudden increase in dyspnoea with subcutaneous bleeding and massive haemoptysis. On admission, laboratory tests showed a platelet count of 10×109 /L. CTPA showed a mass attached to an atrial septal blocker in the right atrium (figure 2A). Cardiac ultrasound revealed a large mass in the right atrium extending past the tricuspid valve into the right ventricle and was beating with the blood flow, this was never observed in any previous cardiac ultrasound examinations (online suppelemental figure S2, video 2). Urgent vascular embolisation for haemoptysis (online supplemental figure S3, S4) was performed and the patient was then transferred to the Department of Cardiac Surgery for resection of the intra-atrial mass (figure 2B). Postoperative pathology confirmed the diagnosis of atrial myxoma (online supplemental figure S5). The patient was discharged from the hospital when she was recovered from the heart operation. She was given warfarin for follow-up anticoagulation therapy. Her haemoptysis is no longer present and her dyspnoea has improved significantly during the next 3 months of follow-up.
{kind=link}
{kind=link}
(A) CTPA demonstrated an enlarged mass in the right atrium compared with the initial CT images. (B) Excised right heart mass suggestive of atrial myxoma. CTPA, CT pulmonary angiography.
Disclaimer: this video summarises a scientific article published by BMJ Publishing Group Limited (BMJ). The content of this video has not been peer-reviewed and does not constitute medical advice. Any opinions expressed are solely those of the contributors. Viewers should be aware that professionals in the field may have different opinions. BMJ does not endorse any opinions expressed or recommendations discussed. Viewers should not use the content of the video as the basis for any medical treatment. BMJ disclaims all liability and responsibility arising from any reliance placed on the content.
Fajiu Li, pulmonologist and pulmonary vascular interventional radiology specialist
Right atrial myxoma is a rare benign tumour of the heart with an incidence of 0.0017% in the general population.1 Meanwhile, this is the first report in the literature of an atrial myxoma with pulmonary artery myxoma embolisation after percutaneous atrial septal repair, in this case, 8 years later. Although rare, myxomas are the most common primary tumours of the heart, usually occurring in the atria and consisting of a stroma rich in acidic mucopolysaccharides with polygonal stromal cells scattered throughout the matrix. Clinical manifestations of myxoma, without specificity, may include intracardiac obstruction, thromboembolism including pulmonary embolism and cerebral infarction, constitutional symptoms such as fever, fatigue and laboratory changes, including anaemia, elevated D-dimer and erythrocyte sedimentation rate.
The diagnosis of pulmonary artery myxoma embolisation may be made based on histological and pathological findings. CTPA may reveal an intravascular low-density filling defect, which is often first considered as pulmonary thromboembolism. Intra-atrial myxoma found by cardiac ultrasound can be indirect evidence of myxoma embolisation. Besides, another circumstantial evidence of myxoma embolisation is the absence of venous thrombosis observed by lower extremity venous ultrasound. In patients with atrial masses, especially with a history of cardiac invasive procedure, benign primary cardiac tumours and other kinds of masses, such as thrombi and malignant lesions, may require a differential diagnosis. Many cases were reported in the literature of thrombus formation after percutaneous atrial septal repair as far as 10 years later.2 The case we presented was undergone percutaneous closure of the atrial septal defect 8 years ago, which led us to delude ourselves into thinking that the pulmonary embolism was caused by an atrial septal sealer before the acquired mucus-like items from the patient’s pulmonary artery.
Myxomas have a growth rate of about 0.1–2 mm/month. From the patient’s echocardiography and CT evidence, it is clear that the atrial myxoma has grown, but since the mass was not detected on the initial cardiac ultrasound, it was impossible to determine how fast it was growing. The initial failure to detect an intra-atrial mass on cardiac ultrasound may be related to the fact that bedside ultrasound was limited by the patient’s position, the size or spatial location of the mass, the degree of apposition of the mass to the myocardium and the effect of the atrial septal occluder on the ultrasound examination.
Qiong Liu, pathologist
The overwhelming opinion is that cardiac myxoma is a rare benign neoplasm of the heart consisting of spindled, ovoid or star-shaped cellular elements interspersed in a myxoid matrix. These tumours continue to be of interest due to their indeterminate histogenesis and different clinical presentations. The cell of origin remains a controversial topic.3 Ultrastructural examination suggests mucinous tumours derived from multipotent mesenchymal cells.4 In our presented case, immunohistochemical results, positive for pan-cytokeratin and negative for cytokeratin 5/6, demonstrated that the tumour cells originated from the high possibility of mesothelial cells.
Chenghong Li, pulmonary vascular specialist
The consequences of pulmonary artery obstruction due to the right atrial mucinous tumour can be divided into acute and chronic events. Obstruction of the pulmonary artery can be a mucus matrix, a thrombus or a mucinous tumour itself. Large clots or mucus dislodged into the pulmonary artery or/and systemic circulatory systems, such as the brain, the liver, the spleen, the kidneys or the coronary arteries, may lead to sudden death or target organ dysfunction.5 It is well documented that chronic pulmonary obstruction caused by myxoma emboli can lead to irreversible pulmonary hypertension. There are a few literature reports of pulmonary artery aneurysms due to embolization from right-sided cardiac myxoma.6
Once diagnosed, it needs to be treated as soon as possible. In atrial mucinous tumours combined with pulmonary embolism, surgical removal of the atrial mass and pulmonary emboli is considered to be the standard strategy with curative effect. The main factor attributed to tumour recurrence after surgical resection is incomplete excision of the tumour and subsequent enlargement.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but our Ethics Committee exempted this study. Participants gave informed consent to participate in the study before taking part.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
WQ, ZZ and QL contributed equally.
Contributors WQ, ZZ and QL conceived the report. QL reviewed the histology. WQ, ZZ, SC, FL and CL drafted the manuscript. All authors reviewed and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Airwaves