Article Text

Abstract
Background Multiple serotypes of pneumococci have epidemiological and clinical implications, such as the emergence of non-vaccine serotypes and the acquisition of antimicrobial resistance. Prevalence of multiple serotypes of pneumococci in adults and their risk factors are not known.
Methods We enrolled adult patients from age ≥15 years with radiologically confirmed pneumonia in four hospitals across Japan. Pneumococcal pneumonia was defined with a pneumococcal bacterial density of ≥104/mL in sputum by lytA quantitative PCR, and serotypes were determined. Pneumonias with a single serotype were categorised as single-serotype pneumococcal pneumonia and with two or more serotypes as multiple-serotype pneumococcal pneumonia. Multivariable logistic regression was used to assess the risk factors.
Results 3470 patients (median age 77 years, IQR 65–85) were enrolled. Pneumococcal pneumonia was identified in 476 (18.3%, n=2605) patients. Multiple serotypes were detected in 42% of them. Risk of having multiple serotypes was low among patients who had received 23-valent pneumococcal polysaccharide vaccine (PPSV23) vaccines (adjusted OR 0.51 (95% CI 0.27 to 0.94)). Proportion of non-PCV7 PPSV23 serotypes in overall distribution of multiple serotypes was 67.4% (n=324/481) compared with 46.4% (n=128/276) in that of single serotypes (p=0.001). Serotypes 5, 9N/9L, 10A, 12/22/46, 17F and 35F were associated with multiple-serotype pneumonia, and serotypes 6A/6B, 23F, 11 and 6C/6D were associated with single-serotype pneumonia. Proportion of more invasive serotypes (serotypes 1, 5, 7F, 8) was significantly higher in multiple-serotype pneumonia (p=0.001).
Conclusions Multiple serotypes of pneumococci are common in sputum of adult patients with pneumonia. The risk of multiple-serotype pneumococcal pneumonia is lower than that of single-serotype pneumococcal pneumonia among PPSV23-vaccinated patients.
Trial registration number UMIN000006909.
- bacterial infection
- pneumonia
- respiratory infection
- clinical epidemiology
Data availability statement
Data are available on reasonable request. Data related to this study are available on reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on the topic?
More than one serotype of pneumococci can simultaneously colonise the nasopharynx in adults and can cause invasive diseases.
Prevalence of multiple serotypes of pneumococci among adult patients with pneumococcal pneumonia and their associated risk factors are unknown.
What this study adds?
How this study might affect research, practice or policy
Introduction
Streptococcus pneumoniae is a common cause of community-acquired pneumonia (CAP) worldwide. After introduction of pneumococcal conjugate vaccines, the diseases caused by vaccine serotypes have reduced remarkably; however, the incidence of pneumonia caused by non-vaccine serotypes has continuingly increased, particularly in adults.1–5 Pneumococcal pneumonia can be divided into invasive (bacteraemic) and non-invasive (non-bacteraemic), and majorities are non-invasive.6 7 Because of the nature of non-invasive infection, difficulty to get good quality sputum and a prior use of antibiotics, conventional culture methods are not efficient to diagnose non-invasive pneumococcal pneumonia.6 8 Real-time PCR has become an established method to diagnose pneumococcal pneumonia in sputum because of its increased sensitivity and decreased turnaround time.8–12
Pneumococcus has at least 98 serotypes that have potential to cause invasive (eg, meningitis, bacteraemia) and non-invasive (eg, pneumonia, sinusitis, otitis media) diseases.7 13 Although only single-serotype infection is generally reported, which is because of limitation of the conventional culture and identification methods, simultaneous infections with two serotypes have been reported. Serotype 9V and serotype 7 were isolated in the cerebrospinal fluid (CSF) in a man aged 60 years with meningitis.14 Similarly, in a 10-month-old infant, serotype 23B was isolated from the CSF, and serotype 23F was isolated from the blood.15 Pneumococci are highly recombinogenic transformable bacteria; when two or more than two serotypes are present, they can exchange genetic material that has implications for adaptation with host, drug resistance, biofilm formation and emergence of non-vaccine serotypes, which may lead to treatment failure and reduced effectiveness of vaccination.16–18
Besides these case reports, to our knowledge, only one epidemiological study about multiple-serotype infections that caused invasive pneumococcal diseases has been published.13 However, there is no published study that describes the epidemiological and clinical characteristics of multiple-serotype infections in adults with non-invasive pneumonia. We did a multicentre cross-sectional study of adult patients with pneumonia and applied an advanced PCR system that can identify more than one serotype of pneumococci simultaneously.19 Here, we describe the epidemiological and clinical characteristics of adult patients with multiple-serotype pneumococcal pneumonia by comparing with those with single-serotype pneumococcal pneumonia.
Methods
Study design
The Adult Pneumonia Study Group-Japan conducted this study as a part of the multicentre prospective cross-sectional study of adult pneumonia in four main islands in Japan.20 21 The study sites were: Ebetsu City Hospital in Hokkaido; Kameda Medical Centre in Chiba; Chikamori Hospital in Kochi and Juzenkai Hospital in Nagasaki. This study was a part of the surveillance study that was carried out from 28 September 2011 to 23 August 2014 and was registered in the University hospital Medical Information Clinical Trial Registry.
Study population
Patients who fulfilled these three criteria in the emergency and outpatient departments were enrolled: (1) age ≥15 years, (2) symptoms suggestive of pneumonia and (3) findings suggestive of pneumonia in chest X-ray or CT scan. Pneumonia cases were classified into CAP and healthcare-associated pneumonia (HCAP) following the American Thoracic Society/the Infectious Diseases Society of America guideline.22 23 Patients who developed pneumonia after 48 hours of admission in another inpatient facility were excluded. Pneumococcal pneumonia was defined by positive lytA real-time PCR with a pneumococcal bacterial density ≥104 copies/mL in sputum in patients with radiologically confirmed pneumonia.9 10 19
Data collection
Using a standardised data collection form, we collected demographic and clinical data from the patients and medical charts. Good quality sputum and blood specimens were collected at the time of admission. If the patients could not cough up sputum, it was induced by inhalation of hypertonic saline soon after admission, and the sputum was collected before giving antibiotics. Chest X-rays were taken within 24 hours of admission, and CT scans were done at the treating physicians’ discretion.
Laboratory methods
On average 250 μL of sputum was taken from each patient, and DNA was extracted using the QIA DNA Mini Kit (Qiagen). Identification of pneumococci by lytA and serotyping by the nanofluidic real-time PCR system were performed as described elsewhere.24 Respiratory viruses were tested by in-house multiplex PCR which was described elsewhere.25 Pneumococcal serotypes 1, 5, 7F and 8 were categorised as highly invasive serotypes, and remaining serotypes were grouped as less invasive serotypes.26 Urine samples were tested by BinaxNOW Pneumococcal Urinary Antigen Test (BinaxNow, Alere, USA).
Pneumococcal vaccination in Japan
PCV7 was available in Japan from February 2010, and it became widely available for children <5 years by the end of 2010. However, it was introduced to the routine immunisation in April 2013 and was replaced by PCV13 in November 2013. The estimated vaccine coverage rate was 80%–90% in 2012 and >90% in 2013.27 At the time of this study, 23-valent pneumococcal polysaccharide vaccine (PPSV23) was not recommended for adults of ≥65 years; however, it was introduced in the routine vaccination in October 2014, and PCV13 was also licensed for this age groups in June 2014. The PPSV23 coverage in 2013 was 25%.28 At present, all adults aged ≥65 years are eligible for PPSV23 vaccination.
Statistical analysis
Details of the covariates are shown in the online supplemental file 6. Statistical analysis was done in Stata V.14. The χ2 test was used to compare the proportions, and Mann-Whitney U test was used to compare the medians. Unadjusted and adjusted ORs (aORs) were estimated by logistic regression models. Stratified analysis was done to examine the subgroups for effect modification. Variables with p value ≤0.05 in univariate analysis, and a priori variables (patient’s sex, age, age groups, vaccination status, present smoking, underlying diseases, prehospital antibiotic use, study site, study period, type of pneumonia, hypoxaemia and severity score (Confusion, blood Urea nitrogen, Respiratory rate, Blood pressure, 65 years of age and older (CURB-65)) were adjusted in the final multivariable logistic regression model.29 30
Supplemental material
Results
Characteristics of the study population
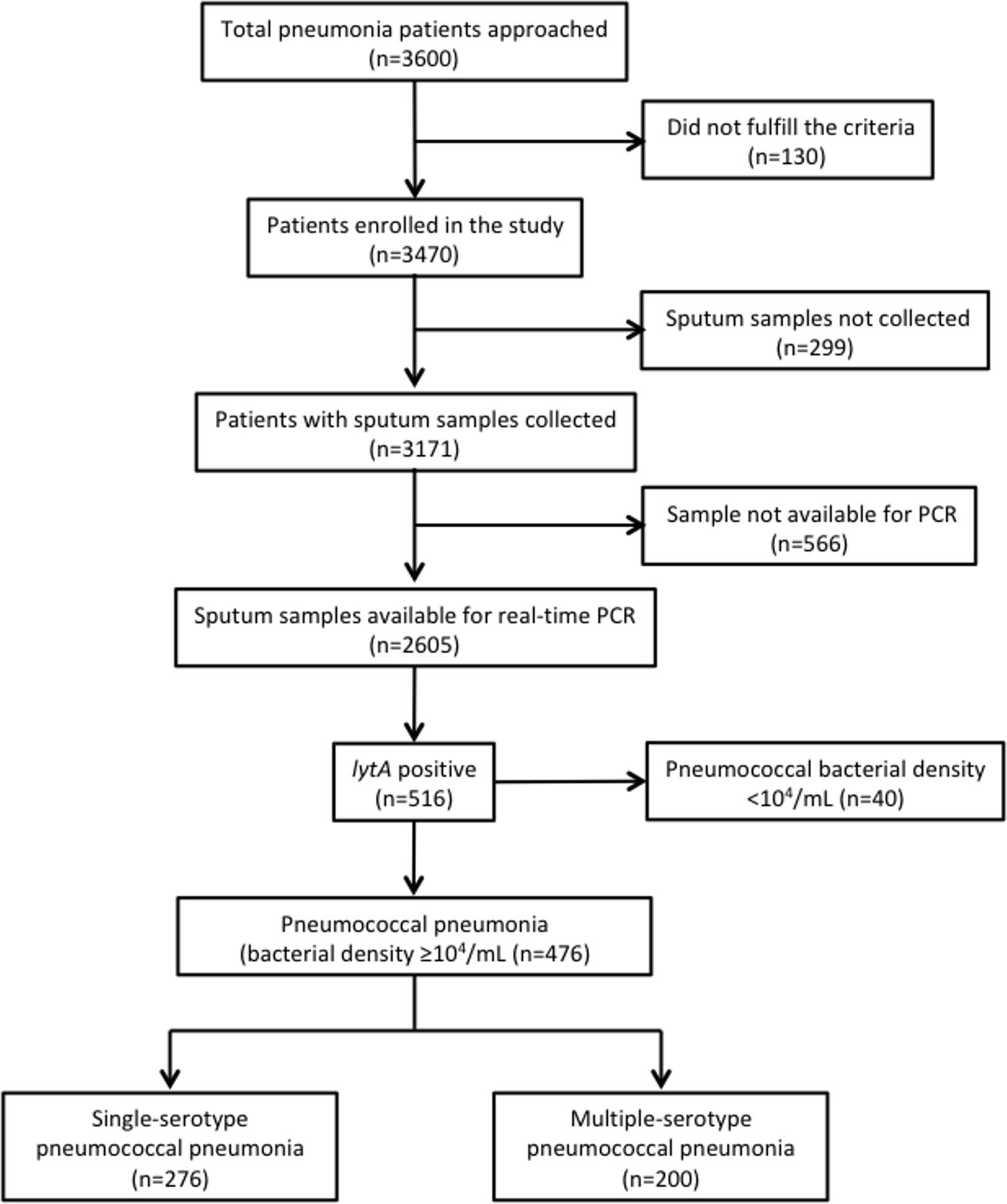
Overall, 3600 adult patients with pneumonia were approached. The total number of patients enrolled was 3470 (figure 1), the median age was 77 years (IQR 65–85), 75.5% were ≥65 years old and 59.5% were male. Some 30.4% of patients had PPSV23 vaccine in last 5 years (table 1). Distribution of patients in different age groups is shown in figure 2. Sputum was available for PCR in 2605 patients. Characteristics of patients with sputum samples available and those with ‘not available for PCR’ are shown in online supplemental file 1. Among the 2605 patients, pneumococcal pneumonia was identified in 476 (18.3%) patients.
Supplemental material
Demographic and clinical characteristics of adult patients with pneumonia enrolled in the study
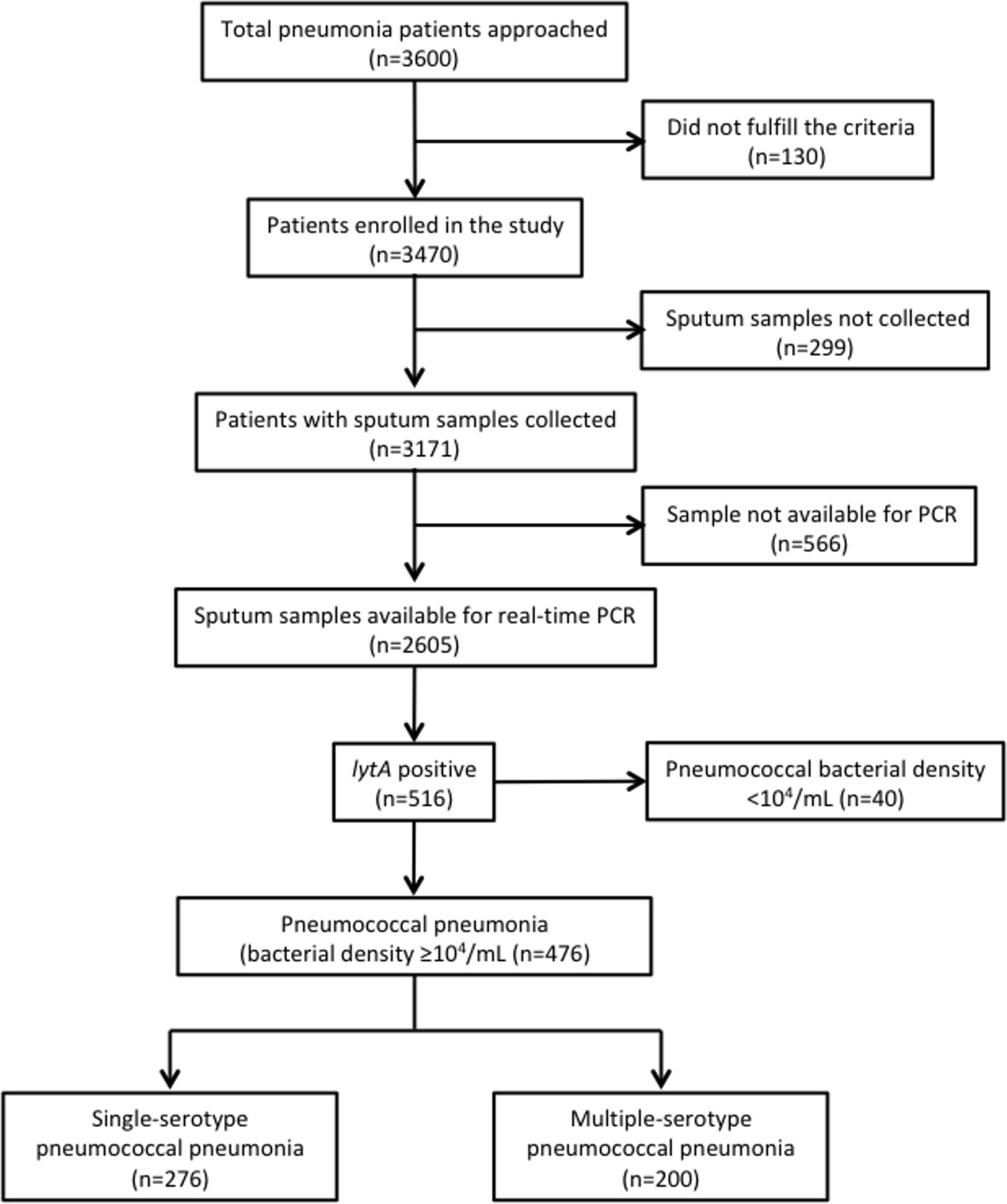
Patient enrolment and identification of pneumococcal pneumonia. Flow chart shows the number of adult patients (≥15 years) from the enrolment to the identification of patients with single-serotype and multiple-serotype pneumococcal pneumonias.

Distribution of pneumonia in adults by age in Japan. Bar diagram shows the distribution of radiologically confirmed adult patients with pneumonia (black bar), single-serotype pneumococcal pneumonia (blue bar) and multiple-serotype pneumococcal pneumonia (green bar) by age group.
Clinical characteristics of patients with pneumococcal pneumonia
The median age was 72 years (IQR 63–82.5), 70.4% of them were ≥65 years of age and 62.4% were male. Clinical features, such as fever, hypoxaemia, leukocytosis, raised CRP, lobar consolidation in chest X-ray and CAP were more prevalent in patients with pneumococcal pneumonia than non-pneumococcal pneumonia. Patients with pneumococcal pneumonia tended to be current smokers, and respiratory syncytial virus and rhinovirus co-infections were more prevalent in them than patients with non-pneumococcal pneumonia (table 2).
Comparison of characteristics of patients with pneumococcal pneumonia versus non-pneumococcal pneumonia, and single-serotype pneumococcal pneumonia versus multiple-serotype pneumococcal pneumonia
Clinical characteristics of patients with multiple-serotype pneumococcal pneumonia
Multiple serotypes were detected in 42% (n=200/476) of the patients with pneumococcal pneumonia. Demographical and clinical characteristics of patients with multiple serotypes and single serotypes are shown in table 2. The proportion of patients who received PPSV23 vaccines was lower in the multiple-serotype group than that in the single-serotype group (19.6% vs 33.0%, p=0.007). Among patients aged ≥65 years, the proportions of PPSV23 vaccinated were 24.7% in multiple-serotype pneumonia and 38.6% in single-serotype pneumonia (p=0.029). The history of vaccination is unknown in 32.5% in multiple-serotype and 24.4% in single-serotype pneumonias (p=0.106) in the ≥65 years age group.
The risk of multiple-serotype pneumonia was lower among the PPSV23-vaccinated than PPSV23-non-vaccinated patients (aOR 0.51 (95% CI 0.27 to 0.94)) (table 3). Characteristics of PPSV23-vaccinated and PPSV23-non-vaccinated patients were compared (online supplemental file 2), and characteristics of patients with known vaccination history and unknown were also compared (online supplemental file 3), and the characteristics with significant differences were adjusted for the multivariable analyses. The association of PPSV23 with the risk of multiple-serotype pneumonia was further examined in subgroups. We found the effect size of the risk of multiple-serotype pneumonia was much less among women (aOR 0.23 (95% CI 0.07 to 0.8)) than men (aOR 0.62 (95% CI 0.3 to 1.29)); the test for interaction was not significant due to a small sample size. Similar observations were made among patients with CAP (aOR 0.40 (95% CI 0.20 to 0.82)) and lobar pneumonia (aOR 0.37 (95% CI 0.17 to 0.79)) (table 4).
Supplemental material
Supplemental material
Comparing associated characteristics of multiple-serotype pneumococcal pneumonia with single-serotype pneumococcal pneumonia
Stratified analysis of the association between 23-valent pneumococcal polysaccharide vaccine (PPSV23) and multiple-serotype pneumococcal pneumonia
Serotype distribution in single-serotype and multiple-serotype pneumococcal pneumonias
The serotype distribution is shown in figure 3. In total, 28 different serotypes/serogroups were identified. Serotype 3, 6A/6B, 10A, 11, 19F, 6C/6D and 35B were common in single-serotype pneumonia. Serotype 3, 10A, 19A, 15B/15C, 6A/6B and 35B were common first dominant serotypes in multiple-serotype pneumonia; serotype 10A, 5, 9N/9L, 4 and 17F were common second dominant serotypes and serotype 10A, 17F, 4, 12/44/46 and 18 were common third dominant serotypes. When overall serotype distributions were compared between these two groups of pneumonias, serotype 6A/6B, 23F, 11 and 6C/6D were associated with single-serotype pneumonia, whereas serotype 5, 9N/9L, 10A, 12/22/46, 17F and 35F were associated with multiple-serotype pneumonia (table 5). The proportions of PCV13 serotypes in single-serotype and multiple-serotype pneumonias were 46% (127/276) and 44.1% (212/481), respectively (p=0.605), whereas, non-PCV7 PPSV23 serotypes were 46.4% (128/276) in single-serotype pneumonia and 67.4% (324/481) in multiple-serotype pneumonia (p=0.001); similarly, non-PCV13 PPSV23 serotypes were 25.4% (70/276) in single-serotype pneumonia and 43% (207/481) in multiple-serotype pneumonia (p=0.001). The proportions of PPSV23 serotypes in single-serotype pneumonia and multiple-serotype pneumonia were 71.4% (197/276) and 87.1% (419/481), respectively (p=0.001). Similarly, the proportions of more invasive serotypes (serotype 1, 5, 7F and 8) were 0.72% (2/276) in single-serotype pneumonia and 7.7% (37/481) in multiple-serotype pneumonia (p=0.001).
Overall serotype distribution in multiple-serotype pneumococcal pneumonia and single-serotype pneumococcal pneumonia

Distribution of pneumococcal serotypes. Bar diagram showing the distribution of pneumococcal serotype/serogroups in single-serotype pneumococcal pneumonia (number of serotypes=276) and multiple-serotype pneumococcal pneumonia (number of serotypes=481). Blue bar represents serotype distribution in single-serotype pneumonia, whereas orange, green and purple bars represent serotype distributions of first, second and third dominant serotypes in multiple-serotype pneumonia. PPSV23, 23-valent pneumococcal polysaccharide vaccine.
Correlations of PCR results with urinary antigen test and blood culture
Among 1990 patients whose urine antigen were tested, 290 were positive (14.6%) for pneumococci. Out of these 1990 patients, the PCR result was available for 1662 patients. Both the PCR and the urinary antigen test were positive in 169, and both were negative in 1249; the proportion of concordant results was (169+1249)/1662, that is, 85.3%. Similarly, we had blood culture results of 2041 patients; among them, S. pneumoniae was isolated in 21 patients (1.0%). Among the 2041 patients, PCR result was available for 1591 patients. Identification by PCR and isolation of pneumococci in blood culture were matched in 19 patients, and both tests were negative in 1304 patients; the proportion of concordant results was (19+1304)/1591, that is, 83.2%. Combinations of positive results of various tests are shown in a Venn diagram (online supplemental file 5). Among the 19 patients with matched PCR and blood culture results, serotyping results of blood isolates were available for 14 patients; 13 of them were matched. One unmatched sample was 6B in blood isolate and 6C/6D in PCR. Out of the corresponding 14 sputum samples, 6 had multiple serotypes and all the dominant serotypes matched with serotypes identified in blood culture isolates. We did not observe any highly invasive serotypes among these matched serotypes.
Supplemental material
Pneumococcal bacterial density
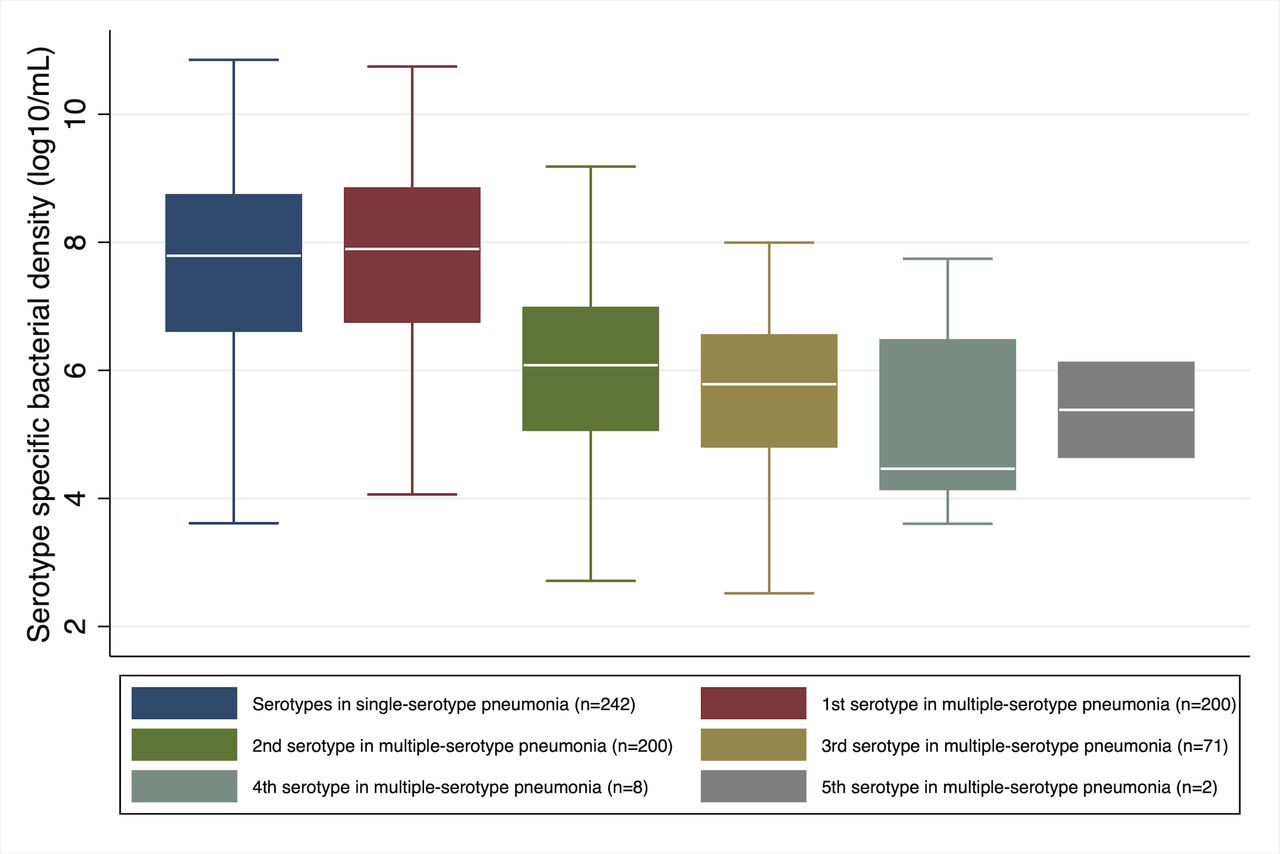
Median pneumococcal load density in the pneumococcal pneumonia was 7.48 log10/mL (IQR 6.07–8.29 log10/mL). The serotype-specific median bacterial density of the most dominant serotypes in multiple-serotype pneumonia was similar to that of single-serotype pneumonia (7.89 log10/mL vs 7.79 log10/mL); however, the bacterial density of other serotypes in multiple-serotype pneumonia was about 2 log10/mL lower than the dominant serotype (p=0.001) (figure 4). Pneumococcal load density was found to be positively correlated with CRP and CURB-65 scores, and negatively with SpO2 in single-serotype pneumonia, whereas in multiple-serotype pneumonia, the load density was positively correlated with body temperature, CRP and CURB-65 scores, and negatively correlated with SpO2 (figure 5; online supplemental file 4).
Supplemental material

Bacterial density in single-serotype pneumococcal pneumonia and multiple-serotype pneumococcal pneumonia. Box and whisker plot showing the distribution of bacterial density of serotypes in single-serotype pneumococcal pneumonia and multiple-serotype pneumococcal pneumonia in order of dominance. The total number of serotypes identified was 242 in single-serotype pneumonia and 481 in multiple-serotype pneumonia.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatter plot showing the relationship between pneumococcal bacterial density and C-reactive protein in single-serotype pneumococcal pneumonia and multiple-serotype pneumococcal pneumonia. Solid lines represent the linear regression fit across the patients. Spearman’s rank correlation coefficients were 0.205 (p=0.001) and 0.184 (p=0.009) for single-serotype pneumococcal pneumonia and multiple-serotype pneumococcal pneumonia, respectively.
Discussion
This multicentre study of adult pneumonia showed that multiple serotypes were prevalent in pneumococcal pneumonia. To best of our knowledge, this is the first study that describes the demographic and clinical characteristics of multiple-serotype pneumococcal pneumonia in adults. Compared with single-serotype pneumonia, the risk of multiple-serotype pneumonia was lower among patients who had taken PPSV23 vaccine in last 5 years, and the risk was much lower in female sex. Serotype distributions in single-serotype and multiple-serotype pneumonias were different, and the proportion of non-PCV7 PPSV23 serotypes was significantly higher in multiple-serotype pneumonia than single-serotype pneumonia.
Multiple-serotype pneumonia constituted 42% of pneumococcal pneumonia. This high prevalence was in concordance with a high prevalence (50%) of multiple serotypes detected as carriage in healthy adults in Japan.31 Pneumococcal pathogenesis starts with nasopharyngeal colonisation32; two or more than two serotypes can colonise at the same time, and studies in children have shown that the multiple-serotype colonisation is associated with pneumonia.33 Multiple-serotype colonisation, which we assume the precursor of multiple-serotype pneumonia, has implications for vaccine serotype replacement, pneumonia diagnosis and antimicrobial resistance.16 Therefore, it is important to explore the epidemiological and clinical characteristics of multiple-serotype pneumonia.
Most studies of pneumococcal invasive diseases show single serotypes. Conventionally, serotypes are determined by Quellung reaction on one or two colonies picked up from the culture plate. Molecular methods, such as real-time PCR show higher sensitivity to detect multiple serotypes than WHO-recommended culture method.34 35 When multiple serotypes are present in the culture plate, dominant serotype is generally picked up by the conventional method. In this study, 14 patients had serotyping results of blood culture isolates, 6 of them had multiple serotypes by PCR and the serotypes identified by the conventional method were all of the dominant ones identified by PCR. Our data also show that there is about 100 folds (2 log10) difference in bacterial loads between dominant and subdominant serotypes. Therefore, in sputum culture, to detect 2 serotypes, we probably need to serotype 100 colonies. However, this ratio of bacterial loads in invasive disease is unknown. Our colonisation study in healthy elderly in Japan shows that the median bacterial load is 3.98 log10/mL in saliva or nasopharyngeal samples (data not published), which is 100 times lower than that of second dominant serotype (6 log10/mL) in multiple-serotype pneumonia. Due to such a high bacterial load of second dominant serotypes, we think at least second dominant serotypes may have a pathological role in non-invasive pneumonia. However, it may be possible that the most dominant serotypes are the ones that often invade into the circulation.
Receiving PPSV23 vaccine within 5 years was associated with a lower risk of multiple-serotype pneumonia. The risk was much lower in female sex, patients with CAP and patients with lobar pneumonia (although not significantly due a small sample size). Studies have shown that the effectiveness of PPSV23 is higher among female patients than male patients.21 29 The reasons behind higher immune response among female patients are not fully known; however, humoral responses as well as type III hypersensitivity reactions are found to be stronger in female patients.36–38 Our observation of lower risk of multiple-serotype pneumonia in comparison with single-serotype in PPSV23-vaccinated female patients is in line with the implications of the previous studies; however, the mechanisms of protection by PPSV23 vaccine in this pneumonia group, needs to be elucidated. We observed the risk of multiple-serotype pneumonia was lower in PPSV23-vaccinated patients than not-vaccinated patients, and the proportion of multiple-serotype pneumonia was significantly higher in CAP than HCAP (45.5% vs 29.1%, p=0.004); that may lead to a much lower risk of CAP than HCAP among PPSV23-vaccinated patients. We did not find any protection of the vaccine against multiple-serotype pneumonia after 5 years of the vaccination; however, we think a larger study is needed.21 In this study, the sample size of the vaccinated for >5 years was small, six in multiple-serotype and seven in single-serotype pneumonias (data not shown).
We found that the proportion of non-PCV7 PPSV23 or non-PCV13 PPSV23 serotypes was significantly higher in multiple-serotype pneumonia than single-serotype pneumonia. Serotypes 5, 9N/9L, 10A, 12/44/46, 17F and 35F were found to be associated with multiple-serotype pneumonia, whereas serotypes 6A/6B, 23F, 11 and 6C/6D were associated with single-serotype pneumonia. Among these serotypes, from our previous study of serotype-specific vaccine effectiveness of PPSV23, we found the point estimates of the vaccine effectiveness for serotype 10A was 30.5%, and for serotype 6A/6B, it was −35.9%.21 Because of the small sample size, serotype-specific vaccine effectiveness could not be calculated for all these serotypes in that study; from our observation of the association of serotype 10A with multiple-serotype pneumonia and serotype 6A/6B with single-serotype pneumonia in this study, it is plausible that the vaccine effectiveness of the PPSV23 could be higher among the serotypes prevalent in multiple-serotype pneumonia, especially non-PCV7 PPSV23 or non-PCV13 PPSV23 serotypes than those prevalent in single-serotype pneumonia.
Our data show the proportions of serotype coverage by PCV13 and PPSV23 were 46% and 71.4%, respectively in single-serotype pneumonia; other studies show the proportion of PCV13 serotypes from 40.2% to 46.0% and PPSV23 serotypes from 63.1% to 66.0% among adults in Japan in the study period from 2013 to 2016.39 40 We found a higher proportion of PPSV23 serotypes in multiple-serotype pneumonia (87.1%) than single-serotype pneumonia (71.4%) (p=0.001); this was mostly because of a significantly higher proportion of non-PCV13 PPSV23 serotypes in multiple-serotype pneumonia as discussed above.
Routine serotype surveillance is important as non-PCV13 serotypes have emerged to cause pneumococcal diseases after introduction of the pneumococcal conjugate vaccines, and these replacement diseases most commonly occur in elderly.1 2 41 Comparing serotype distribution before and after introduction of PCV13 in Japan, a study has found that the proportions of the non-PCV13 serotypes, such as 11A, 35B and 33F have increased significantly, along with vaccine serotype 3 after introduction of PCV13 in Japan.42 In our study, non-vaccine serotypes (non-PCV13 serotypes) 9N/9L, 10A, 12/44/46, 17F and 35F were associated with multiple-serotype pneumonia, and serotype 11 and 6C/6D were associated with single-serotype pneumonia. As the proportion of non-vaccine serotypes (non-PCV13 PPSV23) was found to be significantly higher in multiple-serotype pneumonia than single-serotype pneumonia, we believe that the emergence of non-PCV13 vaccine serotypes would be more common in multiple-serotype pneumonia than single-serotype pneumonia after introduction of PCV13.
Very few colonisation studies have been conducted in adults and elderly in Japan.31 43 A study conducted in 2011 shows that serotype 3 (19.0%), 19F (14.3%), 11A (12.7%), 23F (9.5%), 6B (9.5%) and 15B (7.9%) were common.43 Our study showed that serotype 3 was dominant both in single-serotype pneumonia (15.9%) as well as multiple-serotype pneumonia (11.0%), 19F was fifth common (6.5%), 11 was fourth common (7.6%) and 6B was second common (8.3%) in single-serotype pneumonia. ‘Highly invasive serotypes’, such as serotype 1 (1.2%), 5 (5.2%), 7F (0.8%) and 8 (0.4%) were detected in our cohort of multiple-serotype pneumonia, but not in the colonisation study. The other study was conducted in 2018, and it showed that serotype 10A, 12 and 35F were common (sample size, n=22).31
We found bacterial density of one serotype was dominant to that of other serotypes in multiple-serotype pneumonia. This dominance of one serotype is similar to the findings when more than one serotypes are present in nasopharyngeal colonisation in healthy babies and children with acute respiratory tract infections.33 44 These similarities in density of serotypes in colonisation and in pneumonia may indicate that the multiple-serotype colonisation could be the precursor of multiple-serotype infections. This is also supported by the high prevalence of carriage of multiple serotypes in saliva of healthy adults.31
Our study has limitations. We defined pneumococcal pneumonia when PCR was positive with a bacterial density ≥104/mL; although it is a robust technique and is being used increasingly for the diagnosis, we might have included some cases of carriage in the sputum, as the PCR had sensitivity of 85.4% and specificity of 94.6% at that bacterial load cut-off.19 Another limitation is that the nanofluidic PCR system can only detect 50 serotypes; therefore, the characteristics of non-typeable serotypes could not be determined. Clinical and epidemiological characteristics of individual serotypes could not be explored because of low numbers of the serotypes. Similarly, we could not follow-up the patients to know some outcomes, such as 30-day mortality; therefore, their association with multiple-serotype pneumonia could not be examined.
Conclusion
We found a high prevalence of multiple serotypes of pneumococci in adult patients with pneumonia. The risk of multiple-serotype pneumonia was lower among those who were PPSV23 vaccinated. We observed a significantly higher proportion of non-PCV13 PPSV23 serotypes in multiple-serotype pneumonia than single-serotype pneumonia that may have implication for differential vaccine effectiveness of PPSV23 between these two groups of patients.
Data availability statement
Data are available on reasonable request. Data related to this study are available on reasonable request to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the review boards of Institute of Tropical Medicine (Nagasaki University) and the hospitals (reference number or ID: 11063070). We took a written informed consent from all conscious patients. Because the study was observational and there was no invasive intervention or any deviation from the current medical treatment, the necessity of taking an informed written consent was waived in few cases of unconscious patients by all the institutional review boards.
Acknowledgments
We would like to thank Kyoko Uchibori, Rina Shiramizu and Yumi Araki for their technical help.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators Adult Pneumonia Study Group-Japan (APSG-J) collaborators: Masahiko Abe (Ebetsu City Hospital, Hokkaido, Japan),Masayuki Chikamori (Chikamori Hospital, Kochi, Japan), Akitsugu Furumoto (Institute of Tropical Medicine, Nagasaki University, Nagasaki, Japan), Naohisa Hamashige (Chikamori Hospital), Naoto Hosokawa (Kameda Medical Centre, Chiba, Japan), Hiroyuki Ito (Institute of Tropical Medicine, Nagasaki University and Juzenkai Hospital, Nagasaki, Japan), Satoshi Kakiuchi (Institute of Tropical Medicine, Nagasaki University), Norihiro Kaneko (Kameda Medical Centre), Shungo Katoh (Ebetsu City Hospital and Institute of Tropical Medicine, Nagasaki University), Naoko Katsurada (Kameda Medical Centre), Emi Kitashoji (Institute of Tropical Medicine, Nagasaki University), Kei Matsuki (Juzenkai Hospital), Hiroshi Nakaoka (Chikamori Hospital and Institute of Tropical Medicine, Nagasaki University), Kei Nakashima (Kameda Medical Centre), Yoshihito Otsuka (Kameda Medical Centre), Eiichiro Sando (Kameda Medical Centre), Kaori Shibui (Kameda Medical Centre), Takaharu Shimazaki (Institute of Tropical Medicine, Nagasaki University), Daisuke Suzuki (Kameda Medical Centre), Masahiro Takaki (Institute of Tropical Medicine, Nagasaki University), Kenzo Tanaka (Kameda Medical Centre), Kentaro Tochitani (Kameda Medical Centre), Yoshiko Tsuchihashi (Juzenkai Hospital), Takao Wakabayashi (Ebetsu City Hospital), Kiwao Watanabe (Institute of Tropical Medicine, Nagasaki University), Lay-Myint Yoshida (Institute of Tropical Medicine, Nagasaki University).
Contributors BGD, MS, KA and KM (guarantor) proposed the study. MS, TI, MYae, NA, MI, SH, MA and KM trained clinicians and staffs on study protocols and supervised the study in the hospitals. BGD, TI and MYas did serotyping in Nagasaki. BGD and MS did the analysis. BGD, MS, KA and KM clarify the findings. BGD and MS drafted the first report. KM is the guarantor of the paper. All authors contributed to the final manuscript.
Funding This study was supported by Pfizer (grant numbers WI182481 and WS1874254) and Nagasaki University.
Disclaimer The funders did not have any role in study design, data collection and analysis, manuscript preparation and decision to publish.
Competing interests KA declares speaker fees from Eli Lilly, Takeda and Asahi Kasei Pharma. KM declares speaker fees from Pfizer and Kyorin Pharma. No other authors declare any competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.