Article Text

Abstract
Introduction A gap exists in the literature regarding dose–response associations of objectively assessed housing quality measures, particularly dampness and mould, with hospitalisation for acute respiratory infection (ARI) among children.
Methods A prospective, unmatched case–control study was conducted in two paediatric wards and five general practice clinics in Wellington, New Zealand, over winter/spring 2011–2013. Children aged <2 years who were hospitalised for ARI (cases), and either seen in general practice with ARI not requiring admission or for routine immunisation (controls) were included in the study. Objective housing quality was assessed by independent building assessors, with the assessors blinded to outcome status, using the Respiratory Hazard Index (RHI), a 13-item scale of household quality factors, including an 8-item damp–mould subscale. The main outcome was case–control status. Adjusted ORs (aORs) of the association of housing quality measures with case–control status were estimated, along with the population attributable risk of eliminating dampness–mould on hospitalisation for ARI among New Zealand children.
Results 188 cases and 454 controls were studied. Higher levels of RHI were associated with elevated odds of hospitalisation (OR 1.11/unit increase (95% CI 1.01 to 1.21)), which weakened after adjustment for season, housing tenure, socioeconomic status and crowding (aOR 1.04/unit increase (95% CI 0.94 to 1.15)). The damp–mould index had a significant, adjusted dose–response relationship with ARI admission (aOR 1.15/unit increase (95% CI 1.02 to 1.30)). By addressing these harmful housing exposures, the rate of admission for ARI would be reduced by 19% or 1700 fewer admissions annually.
Conclusions A dose–response relationship exists between housing quality measures, particularly dampness–mould, and young children’s ARI hospitalisation rates. Initiatives to improve housing quality and to reduce dampness–mould would have a large impact on ARI hospitalisation.
- acute respiratory infections
- housing quality
- dampness
- mould
- public health policy
- child health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is the key question?
We hypothesised that objective assessments of poor housing quality would be associated in a dose–response manner with increased risk of hospitalisation with acute respiratory infection (ARI).
What is the bottom line?
A dose–response relationship exists between housing quality measures consisting of items relating to damp and mould from a 13-item Respiratory Hazard Index, and rates of hospitalisation for young children with ARI.
Why read on?
This paper presents the largest ever case–control study of the dose–response association between objectively measured housing quality and hospital admission for young children with ARI and estimates that if all housing were free from damp and mould, almost 20% of ARI admissions for children less than 2 years old could be prevented.
Introduction
In New Zealand, as with many other Organisation for Economic Co-operation and Development countries, acute respiratory infections (ARIs) are a major cause of early childhood morbidity.1 2 ARIs are a leading cause of avoidable hospitalisation and account for 50% of general practitioner (GP) consultations in preschool-aged children.3 Upper respiratory tract infections (URTI) are the most common, accounting for 21% of all GP consultations in New Zealand,4 but ARI also includes important lower respiratory tract infections (LRTIs), including bronchiolitis, bronchitis and bronchopneumonia. In 2015, in the Wellington region of New Zealand, there were 9003 children under 2 years old hospitalised for ARI out of an estimated population of 118 580, a rate per population of 7.6%.
Housing and its effects on respiratory health
Many studies now attest to the deleterious effects of damp and cold homes.5 Buildings are subjected to continuously fluctuating moisture and temperature conditions, which can cause damage to building materials and increase indoor humidity,6 promoting mould and bacterial growth, leading in turn to higher rates of respiratory disorders.6 7 Shorter et al 8 found that indoor visible mould and mould odour were associated with new-onset childhood wheeze in a dose-dependent manner. Recent systematic reviews have shown that indoor visible mould and mould odour were associated in a causal way with the development and exacerbations of children’s asthma.9 Dose–response relationships between respiratory illness and indices of mould and damp have also been found in several previous studies.10 11
Efficient heating and insulation have been shown to benefit respiratory health in randomised controlled trials. Retrofitted insulation increased indoor temperatures, reduced relative humidity and improved respiratory symptoms for occupants.12 A subsequent randomised controlled trial of effective home heating showed that asthmatic children’s respiratory health improved significantly and they had fewer days off school in winter.13
Housing in New Zealand
Internationally, mould has been reported in 5%–10% of homes in colder climates, but higher in temperate or warm climates (10%–30%).14 New Zealand is a temperate high-income country with relatively large, inadequately insulated, poorly heated, stand-alone wooden houses. This leads to various problems with cold, damp and mouldy conditions, compounded by the increasing cost of residential electricity, which has led to a growing proportion of fuel poor households who cannot afford to effectively heat their homes.15
Census data for 2013 show that New Zealand’s indigenous people, Māori, constituted 15% of the population and Pacific people constituted 7%. Both groups suffer various degrees of socioeconomic disadvantage.16 Recent analysis showed that ethnic and income inequalities in infectious diseases are large and increasing: Māori and Pacific peoples are more than twice as likely as the European population to be hospitalised with a serious infectious disease.17
A Respiratory Hazard Index (RHI) has been developed and tested to quantify the impact of housing exposures on respiratory health.18 The RHI used in the current study incorporates most of the measures of mould and damp incorporated in the studies by Engvall et al 11 and Kishi et al 10 but differs from these studies by using an independent assessment made by trained observers, and with some additional measures, as described below. There are several case–control studies internationally that have examined associations between ARIs and household environmental conditions, but these have relied on self-report by participants.19–26 As self-reports of dampness or mould have been found to correlate poorly with objective assessments,27 28 there was a need for analysis of consistent, objective measures to orientate and justify potentially costly interventions.
The objective of this study was to examine the distribution of housing-related risk factors for children with severe ARI to form an effective basis for policy and practice to reduce inequalities and prevalence of this disease. We hypothesised that poorer housing quality would be associated with increased risk of hospitalisation with ARI.
Methods
Study design
This was a case–control study of children aged less than 2 years old, embedded as a substudy within the Whiti Te Rā Case–Control Study (a case–control study of the broader risk factors for ARI hospitalisation), using a kaupapa Māori (Māori-based) research framework. This involved partnership with Māori at all levels of the research to ensure that the research objectives, methods and conduct were Māori-led and consistent with tikanga (Māori cultural protocols).29
Setting
The study was conducted in an urban area comprising the catchments of two district health boards (DHBs): Capital & Coast DHB (population 300 000) and Hutt Valley DHB (population 145 310) in the Greater Wellington Region of New Zealand, over winter/spring (April–November) of 2011–2013.
Participants
Children were eligible if they were under the age of 2 years at the time of their index event, usually resident within the catchment and had a parent or legal guardian providing informed consent for participation in the study (which included a housing assessment). Participants outside a predefined period and those recruited after the required sample size was reached were excluded from participation (figure 1).

Recruitment flow diagram. HHI, Healthy Housing Index.
Cases with ARI were admitted to one of the two hospital paediatric wards in the region. Controls presented at one of five general practice clinics across the region with either ARI not requiring hospitalisation, or for routine immunisation, excluding those who had previously been admitted with ARI.
The diagnosis of ARI was made following assessment by the treating clinician. ARI diagnoses included any URTIs and LRTIs, including colds and other URTIs/LRTIs, influenza, pneumonia and bronchiolitis regardless of the diagnostic label. ARI did not include cystic fibrosis, bronchiectasis or chronic lung disease of infancy/bronchopulmonary dysplasia.
Controls were unmatched to cases but recruited in parallel at a ratio of 2:1. To minimise selection bias, all eligible clinic patients were approached.
Excluded were any potential case or control referred to the research group >3 days following the presentation with ARI at a general practice or emergency department, or admission (whichever was latest) or >7 days after their routine immunisation. Participants were not recruited more than once within the same study group. A participant could not be in both case and control groups as cases were defined as those admitted with ARI over the period studied, so a control who was later admitted with ARI was then defined as a case.
Study assessments
An assessment visit was undertaken either in the hospital or at the child’s home, including an interviewer-administered questionnaire that comprised basic demographic details and a comprehensive array of other factors potentially associated with hospitalisation for ARI, including body mass index30 and exposure to secondhand smoking.31
Independent, professional, building assessors subsequently visited each house to carry out a ‘well-house check’ using the Healthy Housing Index (HHI).18 The HHI records housing factors that indicate the ‘healthiness’ of a house or, conversely, provide a measure of how likely it is that occupants will suffer ill health or injury due to housing factors.32 The assessors were blinded to the status of the participants and had been trained in the use of both quantitative (eg, moisture measuring equipment) and subjective (eg, quantification of mould) measurement techniques.
Components of the RHI scale
The RHI, a validated 13-item subscale derived from the HHI, includes household exposure factors with demonstrated a priori associations with respiratory health,18 listed in table 1. We did not assess absence of wall insulation that was a component of the RHI18 as the original manner of assessment, which involved removing the external plate from a power socket and inspecting the wall cavity, was considered potentially hazardous to the inspectors. The detection of a musty smell has been found to have consistent associations with respiratory tract symptoms.33 The ‘mould odour’ is thought to signal active mould growth (and associated microbial volatile organic compounds) that may or may not be visible to the inspector.34 Two components of the RHI relate to factors leading to cold housing: lack of insulation and house receiving little sun. The final element, the use of unflued gas heaters, assesses consequent exposure to indoor pollutants. This element relates more closely to occupant behaviour than the other elements of the scale, which focus on the building itself.18
Housing features measured during the home assessments included in the RHI or the DMI, with proportion of cases and controls found with each feature and corresponding ORs relative to no evidence
Housing quality indices: numbers of subjects (cases and controls) in the study; crude (unadjusted) ORs relative to a reference value; aORs controlling for season, housing tenure, socioeconomic status and household crowding
The first eight components of the RHI (table 2), which relate to damp and mould conditions of the house, are also presented as a subscale, the ‘Damp–Mould Index’ (DMI).
Statistics
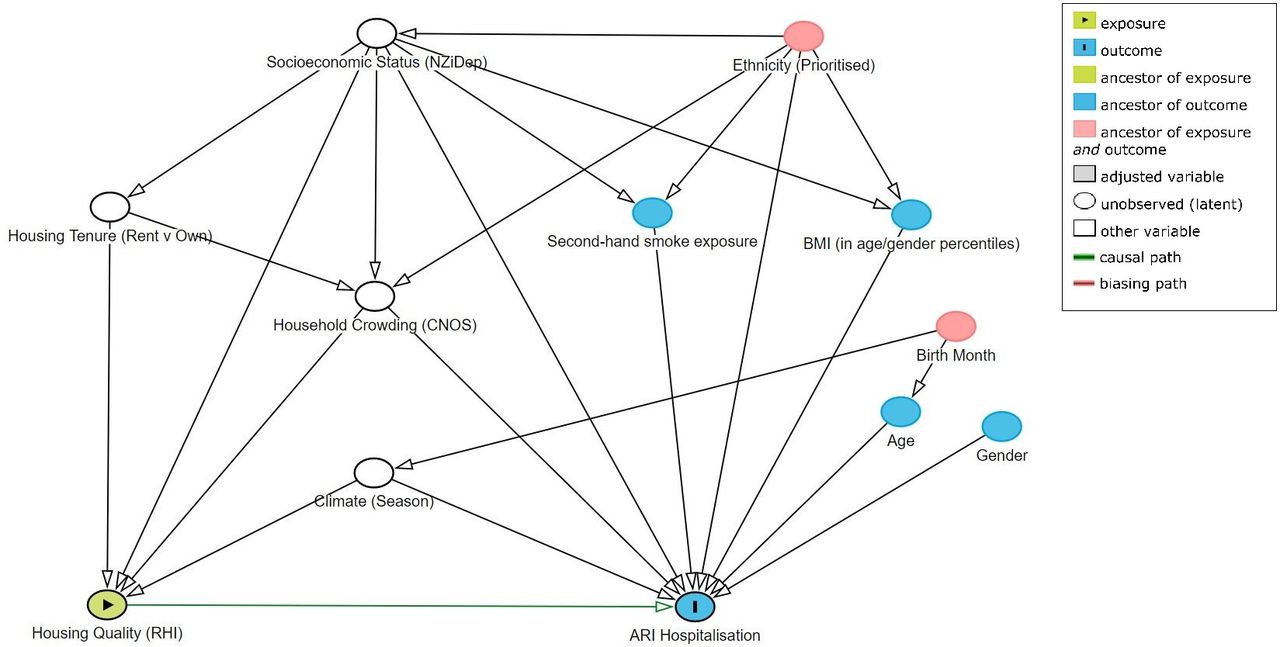
Statistical analyses were conducted using SAS V.9.4. Logistic models measured associations between housing quality (as denoted by RHI or DMI and ARI hospitalisation (case–control status), with the indices expressed as both categorical and continuous variables. In the latter case, the odds estimated were for an increase of one level in the index analysed. Groupings of the levels of factors were set in the following manner: a priori (in the case of age) and into minimally sufficient adjacent groups to enable odds to be estimated (each group requires non-zero counts of cases and controls) for the DMI and season). Relevant confounders were identified by constructing a directed acyclic graph using the software DAGitty V.2.3 to determine a minimal sufficient adjustment set.35 Housing tenure, household crowding (Canadian National Occupancy Standard),36 New Zealand Index of Individual Socioeconomic Deprivation (NZiDep)37 and season of enrolment, along with key demographic variables of age, gender and ethnicity (total response), were evaluated (figure 2). No data were imputed. There were no statistically significant differences in missing data between cases and controls (see online supplementary appendix).
Supplemental material

{kind=link}
{kind=link}
DAG demonstrating causal relationships and potential biasing pathways affecting the association between housing quality and ARI hospitalisation (produced using DAGitty V.2.3 software). In this conceptual diagram, each circle represents an individual exposure (‘node’) of theoretical relevance to this hypothesis; each node is interconnected by directional arrows (‘edges’) that represent theoretical associations based on the researchers’ assessment of a priori literature and determination of biological plausibility. Housing quality (RHI and/or Damp–Mould index as proxy) is the exposure of interest (green node with black border), with ARI hospitalisation (blue node with black border) as the outcome of interest. The association of interest, therefore, is the edge represented by the green arrow connecting the exposure and outcome. Age, gender, secondhand smoke exposure and BMI (blue nodes with blue borders) are theoretically causally associated with (ie, ancestors of) the outcome alone. In this instance, all the other exposures (‘nodes’) are theoretically causally associated with (ie, ancestors of) both the exposure and the outcome. To adjust for confounding in the association of interest, it is necessary to close all ‘backdoor pathways’ between the exposure and outcome (ie, any pathway (consisting of a series of one or more edges and nodes) that provides an alternate route between the exposure and outcome); this is accomplished by adjusting for at least one node on that path. The minimally sufficient adjustment set is the combination of the fewest nodes that, being ancestors of both the exposure and outcome, if selected, effectively block all backdoor pathways between the exposure and the outcome (white nodes with black borders). These ‘adjusted variables’ are then introduced into the multivariate modelling as potential confounders. No other ancestors (blue, red or green nodes) are necessary (or appropriate) to include in the model as potential confounders. ARI, acute respiratory infection; BMI, body mass index; CNOS, Canadian National Occupancy Standard; DAG, directed acyclic graph; NZiDep, New Zealand Index of Socioeconomic Deprivation; RHI, Respiratory Hazard Index.
There was an inevitable delay between recruitment and the independent building assessors’ follow-up home assessments. To account for potential changes to housing exposures over the period of this delay, respondents were asked, ‘Have you made any changes to heating or insulation of your home since our main questionnaire?’ They were then asked to specify what changes had been made and the approximate dates of the changes. A sensitivity analysis was conducted to examine the potential effects of such changes.
A previous study found that the homes of 30% of children suffering an asthma attack had poor scores in the RHI compared with only 16% of those not reporting an attack.18 We expected poor housing to have at least as much an effect on ARI as on asthma. Using this dichotomous variable, ‘exposure to poor quality housing’, and the proportions found in the previous study, the null hypothesis that the exposure rates for case and controls are equal would be rejected with probability (power) 0.805 with 113 cases and 226 controls (α=0.05).
Patient involvement
No patients were specifically involved in setting the research question or the outcome measures. An advisory group, including members of local healthcare organisations, Māori and Pacific community members, were involved in supporting the development of plans for recruitment, design and implementation of the study. No patients were asked to advise on interpretation or writing up of results.
Results
RECRUITMENT
A recruitment flow diagram is included (figure 1) in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement.38 A total of 188 cases and 454 controls were studied. Although cooperation rates were high, cases and controls differed with respect to not being approached for consent (8.7% vs 3.9%, respectively; p=0.0013) and not being able to have a housing assessment completed (14.3% vs 9.6%, p=0.0022). There were no other statistically significant differences in recruitment processes.
Demographic characteristics
Table 1 shows the demographic profile and key housing characteristics of the subjects. Forty-four per cent of cases and 45% of controls were aged under 6 months. ‘Total ethnicity’ shown in the table reports all ethnicities that participants nominated, so individuals were counted more than once in the table if they reported multiple ethnicities. Such reporting is standard in New Zealand to facilitate the measurement and monitoring of Māori health and inequalities.39 Māori and Pacific ethnicities were strongly represented within both case and control groups. Participants reporting Pacific ethnicity had a higher odds of being a case (ARI hospitalisation) (OR 3.11, 95% CI 2.09 to 4.62), while those reporting European ethnicity had a significantly lower odds of hospitalisation (OR 0.39, 95% CI 0.27 to 0.58). Cases were significantly more likely to live in rented accommodation, have higher levels of individual socioeconomic deprivation and experience crowding.
Key demographic and housing characteristics of the study population (ie, enrolled participants with completed housing assessments), along with crude ORs for all characteristics and aORs for factors included in the logistic model along with the RHI
Housing features assessed
Table 2 shows the proportion of cases and controls exposed to components of the RHI and the DMI. Percentages are calculated as a proportion of the total, excluding missing values. No individual item had more than 5% missing measurements apart from no floor insulation and any mould on joists (see online supplementary appendix). These two items, which required access to (sometimes inaccessible) underfloor areas of houses, were not obtained for 30% (n=56) of cases and 30% (n=136) of controls (for floor insulation) and for 30% (n=57) of cases and 31% (n=139) of controls (mould on joists). When the indices were calculated, only items with measured evidence of each hazard were included; so missing values for a given item contributed an effective value of 0 to the index, potentially attenuating the indices’ ability to discriminate between degrees of harmful exposure. Such attenuation is likely to have been small in the case of floor insulation (see table 2: proportions exposed were almost identical for cases and controls) but may have been greater for mould on joists (exposure rates were twice as high for cases). The unadjusted (crude) ORs in table 2 show a generally stronger relationship between the presence of the housing exposures and case status for the exposures more directly related to damp and mould than for the other exposures.
Two logistic models were fitted to look at associations between housing quality and ARI hospitalisation, controlling for relevant factors.
Table 3 shows the results of the multivariate analyses. The first half of the table shows the associations between the RHI and case–control status, adjusted for housing tenure (rent vs own), household crowding (bedroom deficit), socioeconomic status (NZiDep) and season. The lower portion of the table shows a second analysis in which the RHI was replaced by the DMI subscale in an otherwise identical model.
The estimated coefficients for the above factors were generally similar in this second model. Associations between the DMI and hospitalisation showed generally consistent odds with increasing levels of the index. Levels of the DMI were jointly statistically significant in the model (p=0.042). The higher levels of the RHI were associated with elevated odds relative to the zero level, but the coefficients in the model representing levels of the RHI were jointly not statistically significant in the model (p=0.38).
Table 3 also shows estimated odds from two separate models in which the RHI and then the DMI were fitted as continuous variables, both as the sole factor predicting case–control status (the crude ORs) and adjusted for potential confounders. These provide some evidence of dose–response relationships for both indices but stronger evidence for the DMI, for which the odds of being a case were associated with an average 15% increase for each unit increase of the index. The increases in the RHI were associated with statistically significant increases in the crude ORs but not in the adjusted ORs.
There was an inevitable delay between recruitment and the independent building assessors’ follow-up home assessments. The difference in the median delay overall was 11 days (cases=49 days and controls=38 days). A total of 31 respondents had made changes, 7.4% of the cases and 3.7% of the controls (data not shown), a difference that was statistically significant (χ2 statistic 3.97, p=0.046). As a subanalysis, the RHI was adjusted for changes in insulation, but the odds reported in table 3 changed little (data not shown). There was similarly little change in the odds estimated from another subanalysis conducted on a reduced data set that excluded those who reported changes.
Population attributable risk
By making informed assumptions about the prevalence of damp and mould in New Zealand housing (particularly the housing of children under two), we estimated the benefits in terms of reduced hospitalisations from improving the housing stock so that all had a zero rating using the DMI. Out of a population of 118 580 children,40 there were 9003 children who were hospitalised for ARI in 2015, with 12 701 admissions.41 The odds that a child was hospitalised at least once in 2015 was therefore 0.0822. The average DMI rating for the controls in our study was 1.61 and that for the cases was 2.11. If the nationwide housing quality for those admitted was represented by the average index for the cases and the remainder of housing (for under 2 years not admitted) was represented by that for the controls, the national average can be estimated to be 1.644. This equates to odds of ARI admission of 1.255 relative to houses with a 0 DMI (using the estimated increase in the odds shown in table 3). If housing for children under 2 years of age could be improved to a 0 DMI, our estimates suggest that the odds of admission for ARI would be reduced from 2015 levels of 0.0822 to 0.0655, which equates to around 1700 fewer children admitted, a reduction in the admission rate of 19%.
Discussion
This paper presents the largest ever case–control study of the association between housing quality and hospital admission for young children with ARI. Participants in this housing study comprised children under 2 years of age: 188 cases (children admitted to hospital with ARI) and 454 controls (children attending general practice either with ARI not requiring hospitalisation or for routine immunisation). Independently measured levels of damp, mould and crowding were statistically significantly associated with ARI hospitalisation among this sample of children after adjusting for potential confounders. For each additional housing feature assessed as indicating evidence of damp and mould, there was a 15% increase in the odds of ARI hospitalisation. The RHI did not predict case–control status in a statistically significant way after adjustment.
As mentioned above, several similar case–control studies in other settings have examined the associations between ARIs and household environmental conditions reported by respondents.19–26 Cardoso et al 20 did include a fieldworker visit to the home to assess basic housing characteristics (eg, type of house, water supply and number of rooms) and a basic assessment of indoor environmental conditions, such as ventilation and solar orientation, but no objective measurements of dampness or mould. One of the key strengths of this study is the analysis of independently assessed measures of housing quality. There is evidence from a number of studies that self-reports of dampness or mould correlate poorly with objective assessments.27 28 For example, Dales et al 28 found very poor association of parent-reported mould with fungal biomass: there was over-reporting of mould for children with chronic cough, asthma or allergies relative to asymptomatic children. Similarly, Brunekreef et al noted under-reporting of home dampness by parents of symptom-free children.27 28
As noted earlier, a limitation of this study was the delay between recruitment into the study and the housing inspection. Although some delay was inevitable, long delays from recruitment to inspection could mean that homes were inspected during warmer, drier conditions than were present at the time of the winter/spring recruitment. The higher median delay for the cases was likely due to the disruption of the hospitalisation to families’ household routines. The size of the difference was not particularly large (11 days), so it is unlikely to have had a material impact on the analysis conducted. If the delay did impose a difference in measured exposures, it is likely to be towards the null, reducing the strength of association between the housing exposures and case–control status.
We conducted an analysis of associations between case–control status and the RHI or DMI that specified both indices as continuous variables, with higher values theorised to represent higher levels of hazard to respiratory health presented by housing conditions. As any given element of these indices is unlikely to be equally important as every other element, the estimates from these models are likely to be very context-specific. The ORs represent an average proportional change in the odds of ARI admission averaged across each additional aspect of (harmful) housing conditions evaluated. Whether these continuous indices should be considered as linearly related to the log of the odds is arguable: the sample size of the current study is insufficient to support fitting any more complex functional form of the indices.
The design of the study might have attenuated the associations found between levels of damp and mould and the odds of ARI admission. It is possible that the controls in the current study, which included children with mild ARI, may have elevated damp and mould levels in their home that contributed to their respiratory symptoms. However, we found no difference in levels of exposure to damp and mould for the two groups of controls. The mean DMI was 1.61 for the healthy control group and 1.60 for the mild ARI control group. Given both the high incidence of ARI in the general population and the high rate of attendance at primary care for such events (ie, almost 70% of children presenting to their GP with at least one respiratory condition in their first year of life), we considered the pooling of these two control groups to be valid.4 It should be noted that ARI accounts for around half of GP consultations in preschool-aged children,3 4 so the group of controls with mild ARI will not be too dissimilar from the general population. There is likely to have been some exposure to cold, damp and mould in settings outside the home for the infants studied, such as childcare facilities. However, such exposures are unlikely to be important in the associations adjusted for factors such as socioeconomic status, particularly as the New Zealand average amount of time spent at home is high (around 72%), and this proportion is higher for young children.42
Implications for policy
Given the findings of this study, we predict that 19% of ARI admissions for children under 2 years old would be prevented if all housing were free from damp and mould. This represents savings in costs solely due to hospitalisation (ignoring wider social costs) of just under $8 million NZD (£4.5 million GBP) per annum. Improving housing quality to prevent such hospitalisations is highly desirable also in terms of future costs. Poor housing quality in childhood has also been shown to be associated with adverse health outcomes in adulthood.43 Conversely, improvements in housing contribute to long-term improvements in the health of the occupants, for as long as such improvements remain effective.
The results of the study also highlight the importance that all healthcare professionals are made aware of housing as a risk factor for respiratory illness. This is of particular relevance to primary healthcare, given the high service use generated by childhood respiratory conditions. As an important aspect of the primary and secondary preventions of childhood ARI, we suggest that part of the routine clinical assessment of preschool children should include enquiry about the home environment, particularly regarding the presence of dampness and mould, with referral to appropriate remedial services.
Acknowledgments
We are very grateful to all the children, parents and whānau (families) of the Whiti Te Rā study who gave their time so generously. Our special thanks to the staff at WISE Better Homes, who supplied the building assessors who conducted the objective housing assessments. We also thank the staff at the Tu Kotahi Māori Asthma Trust for their advice and guidance, and Dr Lucy Telfar Barnard for extracting data on hospitalisations and associated costs. We also acknowledge the support and contribution of the following investigators to the design and conduct of the main Whiti Te Rā Study: Professor Carlos A. Camargo Jr, Massachusetts General Hospital, Harvard Medical School, USA; Dr Donna Cormack, Te Rōpū Rangahau Hauora o Eru Pōmare, University of Otago Wellington, New Zealand; Dr Joanna Kirman, Department of Microbiology and Immunology, University of Otago, New Zealand; and Professor Keith Grimwood, Royal Children’s Hospital, University of Queensland, Australia. The authors alone are responsible for the views expressed in this article, and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
References
Footnotes
Contributors TI, MK, BJ, CD, JC, HV, TVS and PHC developed the study design and secured all grant funding. TI, BJ, CD, JBD, LOB and PL undertook the data collection. TI, MK and DRA were responsible for data analysis. TI, MK, BJ, DRTA and PHC undertook the literature review and drafted the manuscript. TI, MK, BJ, JC, TD, CD, DRTA, HV, TVS, PL, ML and PH-C provided critical input in the interpretation of the results. All authors reviewed and contributed to the manuscript. All authors, external and internal, had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. TI is the guarantor.
Funding This study was supported by grants from the Health Research Council (HRC) of New Zealand (HRC Refs: 10/443 and 11/370). The funding organisation had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.
Competing interests All authors have completed the International Committee of Medical Journal Editors uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare the following: TI reports grants from the Health Research Council of New Zealand during the conduct of the study, grants from Janssen Research and Development, and others from AstraZeneca outside the submitted work. MK, CD, JC, HV and ML report grants from the Health Research Council of New Zealand during the conduct of the study. BJ, DRTA, JBD and LOB report grants from the Health Research Council of New Zealand during the conduct of the study and grants from Janssen Research and Development outside the submitted work. ACD, TVS and PI report that they have nothing to disclose. PH-C reports grants from the Health Research Council of New Zealand and the Ministry of Business, Innovation and Employment during the conduct of the study. The lead author affirms that this manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Patient consent for publication Not required.
Ethics approval This study was approved by the New Zealand Health and Disability Ethics Committee (Northern B) MEC/11/01/008.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.