Article Text

Statistics from Altmetric.com
The British Thoracic Society (BTS) first produced a guideline on asthma and its management in 1990. The first collaborative guideline with the Scottish Intercollegiate Guideline Network (SIGN) using evidence-based medicine methodology was published in 2003.1 It has since become a mainstay of asthma management across the UK and beyond with updates published regularly every 18–24 months. The latest BTS/SIGN guideline for the management of asthma was published in 2016.2 Both BTS and SIGN are committed to continuing updates with the next update planned for publication in 2019.
Following publication of National Institute for Health and Care Excellence (NICE) guidelines for diagnosis and monitoring, and for management of chronic asthma,3–5 there are now two if not three national guidelines, for England at least, with some (apparently) striking differences. This statement considers the similarities and differences to assist clinical colleagues in the care of people with asthma.
The evidence base considered by the BTS/SIGN and NICE guideline development groups is broadly the same for each guideline, but the methodology used to produce recommendations is significantly different:
SIGN methodology is a multidisciplinary clinically led process which employs robust critical appraisal of the literature, coupled with consideration of pragmatic studies to ensure that guidelines provide clinically relevant recommendations.
NICE methodology overlays critical appraisal of the literature with health economic modelling, with interpretation supported by advice from a multidisciplinary guideline development group.
These different processes have resulted in some discrepancies in recommendations made by BTS/SIGN and NICE. This article seeks to provide some context to these differences in key areas:
Diagnosis
Pharmacological management:
Treatment at diagnosis.
The introduction of leukotriene receptor antagonists (LTRA) after low-dose inhaled corticosteroids (ICS).
Maintenance and reliever therapy (MART).
Treatment beyond combined inhaler therapy.
Some other issues in managing asthma in children.
The BTS/SIGN guideline also provides recommendations for important aspects of asthma management that are not addressed within NICE guidelines. These include guidance on inhaler devices, the management of acute asthma attacks in both adults and children, the management of difficult asthma, guidance on asthma in adolescents, in pregnant women and on occupational factors.
Diagnosis
A series of recent reports have raised concerns about both over-diagnosis and under-diagnosis of asthma6–8; a key objective of both guidelines was to clarify the evidence and suggest approaches to improve clinical practice.
There are many similarities between the NICE and BTS/SIGN recommendations for achieving an accurate diagnosis of asthma. Both agree that no one symptom, sign or test is diagnostic, and the predictive value of diagnostic tests is influenced by the context, the reference test used and the thresholds applied. Both guidelines recommend that in the absence of unequivocal evidence of asthma, a diagnosis should be ‘suspected’ and that initiation of treatment (typically inhaled steroids) should be monitored carefully and the diagnosis reviewed if there is no objective benefit. Once a diagnosis is made, both BTS/SIGN and NICE guidelines emphasise the importance of recording the basis on which the diagnosis was made.
NICE and BTS/SIGN offer algorithms, both of which are derived from evidence, but neither of which have prospective evidence to support them. In the case of NICE, this was derived from health economic modelling of the diagnostic test data. NICE reports that, in its pilot study in seven practices, its algorithm could be completed in 55% of patients with suspected asthma; a diagnosis of asthma was confirmed in 25% of cases; with 20% reaching no diagnosis despite completing the algorithm.9
BTS/SIGN used the same diagnostic test evidence, but also explicitly searched for pragmatic studies reporting evaluation of diagnostic programmes and, in discussion with the clinical guideline development group members, derived a ‘good practice’ algorithm. The key difference between the approaches is that BTS/SIGN has adopted the terminology of probabilities as resonating with clinical practice.10
This allows for the possibility that there will be people at high probability of asthma in whom a ‘monitored initiation of treatment’ is appropriate without necessarily awaiting further investigation. An example of a ‘high probability’ scenario is the patient presenting with typical symptoms who has had a documented acute attack (with symptoms, chest signs and peak flow confirmation of the attack). This is not recognised as a strategy for making a diagnosis by NICE, but it is reflected in the assumption underpinning the NICE economic modelling that ’a patient with a false negative diagnosis after working through the algorithm will be correctly re-diagnosed after an exacerbation’.10
The diagnostic approach outlined in the BTS/SIGN ‘intermediate probability of asthma’ includes the same diagnostic tests as the NICE algorithm, but (in the absence of pragmatic evidence) is not prescriptive about the best order in which to perform them.
Both guidelines highlight the importance of a good history but the ‘structured clinical assessment’ of BTS/SIGN is broader than the ‘initial clinical assessment’ of NICE incorporating background information from the clinical record such as confirmed wheeze or a peak flow reading from a previous consultation, or risk factors for an alternative diagnosis. BTS/SIGN suggest that existing evidence of atopic status (blood eosinophils, skin prick testing, IgE) may influence the probablity of asthma, but agree with NICE that they should not be considered as ’diagnostic tests'; their key value may prove to be in establishing phenotypes of asthma or identifying triggers that may inform management.11
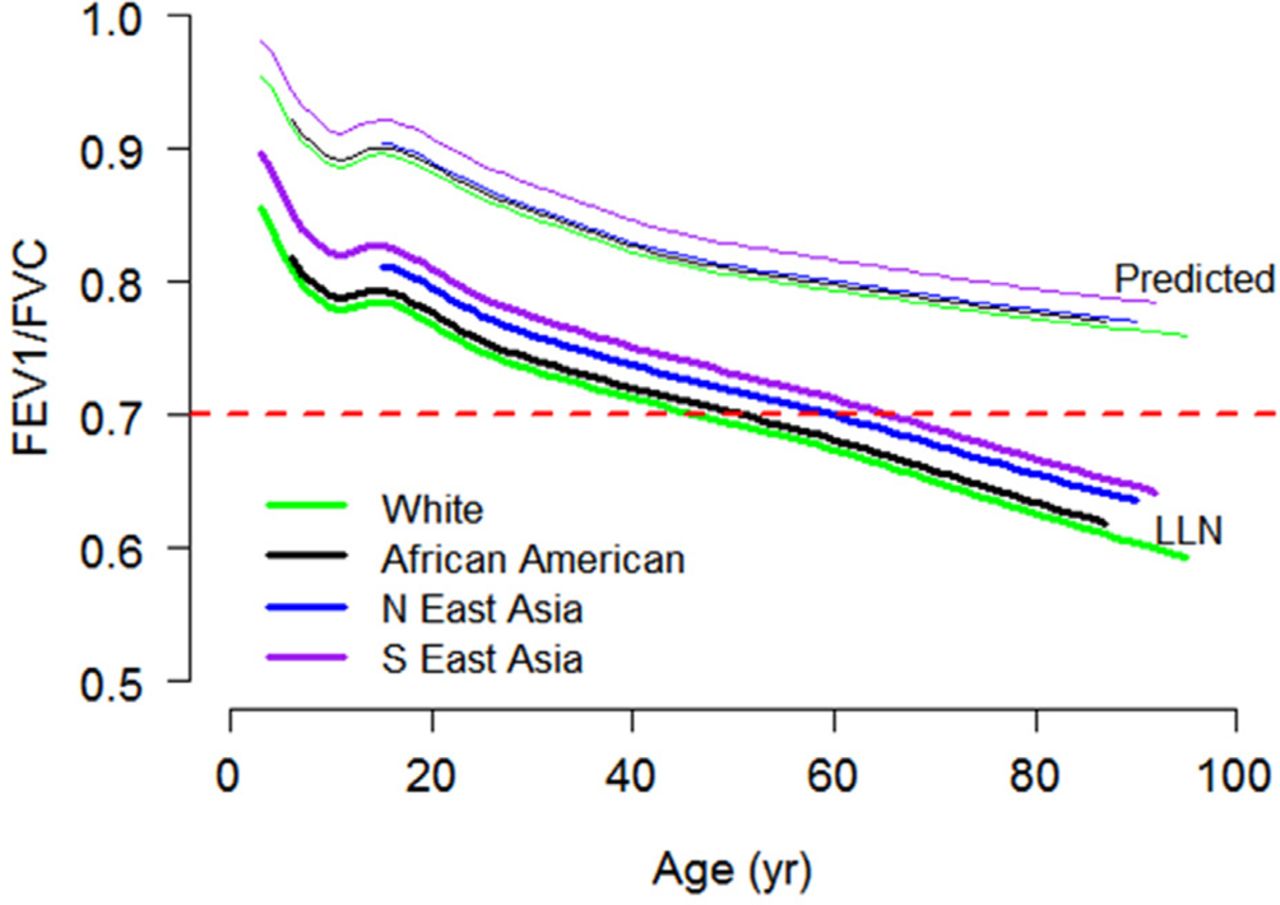
Spirometry is positioned as pivotal by both guidelines, but both caution that it is not useful for ruling out asthma because the sensitivity is low, especially in primary care populations (only 27% of people diagnosed as having asthma in the NICE feasibility work had obstructive spirometry which is similar to the estimate in BTS/SIGN of ‘a quarter having obstructive spirometry’). Both guidelines acknowledge that the forced expiratory volume in one second/forced vital capacity (FEV1/FVC) ratio changes with age. BTS/SIGN therefore recommends use of lower limit of normal (LLN) for FEV1/FVC ratio to avoid under-diagnosis in children and over-diagnosis in the elderly. NICE acknowledges the advantages of using LLN (especially in children) and suggests it should be used ‘if the value is available’ though specifically uses the fixed ratio of 70% as the threshold for proceeding to bronchodilator reversibility.3 Figure 1 illustrates the significant limitations of the fixed ratio cut-off of 70% in children and hence emphasises the importance of using the LLN for defining airways obstruction.12 This is well illustrated in a recent report by Murray et al. They found a mean FEV1/FVC ratio of 84% in children with current asthma with only 2 children <70%. 13

{kind=link}
Predicted FEV1/FVC ratio and lower limit of normal in healthy females of different ethnicity GLI. Reproduced with permission from Quanjer PH, Stanojevic S, Stocks J, et al, All-age multi-ethnic reference values for spirometry, 2012, www.ers-education.org/lrmedia/2012/pdf/266696.pdf (figure 16) under CC BY-NC 2.0.
Both NICE and BTS/SIGN guidelines agree that Fractional Exhaled Nitric Oxide (FeNO) can be used as a surrogate marker of eosinophilic airway inflammation with variable sensitivity/specificity for predicting asthma.14–16 On this basis, NICE positions FeNO prominently in the algorithm in all adults and most children over 5 years with suspected asthma. In the absence of evidence to inform its position within diagnostic algorithms, BTS/SIGN lists FeNO as a potentially useful test, specifically highlighting its role in the investigation of people with an intermediate probability of asthma and without spirometric evidence of obstruction or reversibility.
Both guidelines suggest considering the development of diagnostic hubs (for NICE this is to ‘achieve economies of scale’).4 The pragmatic ‘implementation’ evidence gathered by BTS/SIGN suggested that this was a model used in some countries which might be appropriate in some contexts to ‘streamline pathways for tests not available or inappropriate in primary care’.
Both NICE and BTS/SIGN recommend further research on diagnostic accuracy of objective tests; BTS/SIGN also highlights the need for prospective evidence on the implementation of diagnostic algorithms encompassing clinical assessment as well as objective tests.
Pharmacological management
Treatment at diagnosis for adults (≥17 years) and children 5-16 years
The 2016 BTS/SIGN guideline recommends initiation of treatment with low-dose ICS, making it explicit that patients should not be given short-acting beta-agonists (SABA) alone (except in the few with very occasional short-lived wheeze). This was a major revision from the previously recognised steps 1–5 model of the earlier BTS/SIGN guidelines, which had been in place for years.
The motive for the change came following the National Review of Asthma Deaths17 which demonstrated that a proportion of these deaths occurred in patients only treated with SABA and highlighted this as an important preventable factor.
This change underlines the fundamental importance of a preventer strategy and has been widely welcomed. It has also brought the UK into line with Scandinavian guidance and practice, which has resulted in reduced mortality through early and focused preventer strategies.18
The NICE guideline for the management of asthma has not followed this lead, still advocating the use of SABA alone in its algorithm, though it is noteworthy that the detailed commentary reports this should only be prescribed for a small minority of patients.5 For many, however, this will seem a retrograde step and has the potential to encourage continued over-reliance on SABA.
LTRA after low-dose ICS
The introduction of LTRA after ICS is potentially the most contentious and problematic of the differences between the two guidelines. BTS/SIGN continues the long-held view that low-dose ICS should be followed by addition of long-acting beta-agonists (LABA) in line with international guidelines such as the Global Initiative for Asthma (GINA).19
Head-to-head comparisons of ICS/LABA compared with ICS/LTRA have favoured ICS/LABA for effectiveness in adults (inconclusive in children).20 However, the cost differential is substantial between generic LTRA and LABA so when NICE used a cost-effectiveness model, the results favour LTRA, even though (as NICE acknowledges) LABA is the more effective treatment.
On a practical level, an increase in therapy from ICS alone to ICS/LABA, in most cases, only requires the name of the inhaler to be changed; the patient just continues using one inhaler as their preventer. Indeed, in the case of single maintenance and reliever therapy (MART), a single inhaler may be all that is required. Patients given LTRA have to adapt to an oral therapy, taken only at night, potentially affecting adherence to the inhaled preventer therapy. Preferences (including cultural) for tablets or inhalers and the immediate clinical benefit experienced by the LABA may also influence adherence, as may additional prescription costs for the patient.
The choice for clinicians will be prescribing LABA in a combination inhaler as the more effective first-line add-on therapy (BTS/SIGN) or adopting the NICE strategy of trying the cheaper option of a LTRA which will be cost-effective for those in whom it works. It could, however, be more expensive if ineffective LTRAs are not withdrawn before LABAs are prescribed. A pragmatic trial comparing add-on therapies found that a quarter of people commenced on LTRA switched to or were given additional LABA; none switched from the LABA strategy.21
Additionally, a failure to gain asthma control may ultimately lead to avoidable attacks and associated costs through emergency attendances and even hospital admissions.22
Another potential concern is losing the trust of the patient through the initial use of a cheap but often ineffective treatment in place of an effective simple regimen.
Beyond combination therapy
Both guidelines freely admit that evidence for optimal treatment of patients still uncontrolled after combination therapy is very limited. BTS/SIGN continues to document other treatment options (including specifically detailing effectiveness studies reporting the addition of long-acting muscarinic receptor antagonists (LAMA)). NICE does not offer any practical guidance on what practitioners should do when patients are still uncontrolled on high dose ICS, LABA, LTRA and theophyllines, other than to suggest seeking the help of an “asthma specialist”. The NICE guidance does not discuss advanced therapies such as anti IgE monoclonal antibody, anti IL-5 monoclonal antibody or bronchial thermoplasty, all approved by NICE and widely used in severe asthma services across the UK.
Maintenance and reliever therapy
Adults
Both guidelines state that there is evidence that a MART regime reduces the number of attacks in adults, but there is a discrepancy between the guidelines in the recommended target group.
NICE recommends a MART regimen for people with asthma ‘uncontrolled on a low dose of ICS/LABA, with or without an LTRA’ with the caveat that the maintenance ICS dose should continue to be ‘low’ (as highlighted by the economic evaluation).
BTS/SIGN advises considering a MART regimen for patients ‘who have a history of asthma attacks on medium dose ICS or ICS/LABA’.
In day-to-day practice, decisions on inhaler regimens depend upon consultation between the physician and the patient based on technique, compliance and convenience for the patient. The evidence reviewed in both sets of guidelines would suggest that a MART regimen is a viable option and discussion with the patient should inform which option to take.
Children
The NICE guideline recommends considering MART regimen in children and young people aged 5–16 on the basis of evidence from Bisgaard et al 22 that indicated fewer attacks in children using MART although it is acknowledged that no MART combination is licensed for use in children at the time of publication.
BTS/SIGN has not reviewed this evidence and in the absence of a licensed product, does not make a recommendation for use of MART in children.
Supported self management
Both guidelines agree on the importance of supported self-management including providing clear written advice on actions to take if asthma control deteriorates. Action plans should include advice on short-term increase (eg, short-term quadrupling of dose) of ICS, when to commence oral steroids, and when to seek emergency medical advice. Implementation is challenging. Based on a search of the implementation literature,23 BTS/SIGN recommends a whole systems approach; NICE recommends research on ‘delivering an asthma self-management package’.
Some other issues in asthma in children
Categorising inhaled corticosteroids dosing and potency in children
There are some discrepancies between the NICE and BTS/SIGN categorisation of inhaled steroid dosages for children. NICE have followed the GINA guidelines19 and define ICS doses for children as low, moderate and high dose (NICE Guideline Chronic asthma management, Table 3).5 BTS/SIGN uses very low, low and medium categories and specifically defines doses of commonly used ICS preparations (BTS/SIGN Guideline, Table 10).2 The age ranges used to define a child also differ. NICE defines children as under 16 years while for both BTS/SIGN and GINA children over 12 years are considered with adults (in line with the inclusion criteria of many adult pharmacological studies).
There is an important discrepancy in the summary tables categorising steroid potency (NICE Guideline Chronic asthma management, Table 35; BTS/SIGN Guideline, Table 102) with potential safety issues of which clinicians should be aware (see Table 1). Fluticasone is usually regarded as twice as potent as beclometasone. However, in their dose equivalency table (NICE Guideline Chronic asthma management, Table 3),5 NICE (and GINA) give the equivalent dose of the commonly used Fluticasone Propionate HFA as the same or higher than Beclometasone HFA; similarly, Budesonide DPI and Fluticasone DPI are categorised as being equipotent. The Summary of Product Characteristics in the Medical Compendium24 clearly advises that “Prescribers should be aware that fluticasone propionate is as effective as other inhaled steroids at approximately half the microgram daily dose”; in line with this BTS/SIGN advise that, to avoid over-dosage, the dose of fluticasone should be half that of beclometasone (see Table 1; BTS/SIGN Guideline, Table 10).2
One other important practical difference is that BTS/SIGN recommends that children on medium ICS dose ‘should’ be under the care of a specialist paediatrician for the duration of the treatment. NICE only recommends ‘considering’ seeking advice from a health care professional with expertise in asthma for children between 5 and 16 years who are on a moderate ICS dose with LABA and have uncontrolled asthma.
Inhaler devices
Choosing and using an inhaled device is a critical part of managing asthma, particularly for children. NICE acknowledges suboptimal inhaler technique as a possible reason for uncontrolled asthma and advises that inhaler technique should be observed and checked at every consultation. BTS/SIGN summarises the available evidence and gives good practice recommendations on device choice; NICE signpost a separate NICE document for further guidance.25
Another point BTS/SIGN highlights is that generic prescribing of inhalers should be avoided, for children and adults, as this might lead to people with asthma being given an unfamiliar inhaler device which they are unable to use properly.
Dose equivalency table: children. Comparing NICE, GINA and BTS/SIGN
Management in children under 5 years
Children under 5 years are a particular problem for asthma management guidelines because the evidence base is limited or absent.2
There are two particular problems at this age. First, there is a lack of good objective tests to guide either diagnosis or management in children under 5 years. Second the pattern of asthma in preschool children is heterogeneous and different from adults. Wheezing/asthma attacks are triggered by viral infections (‘colds’) and often there are no asthma symptoms between attacks. This is the most common pattern (‘phenotype’) up to 3 years of age after which interval symptoms typical of chronic asthma become more evident.
Both NICE and BTS/SIGN note that many children under 5 with recurrent episodes of viral-induced wheezing do not go on to have chronic asthma. Neither guideline addresses the issue of what to do with the child who is having frequent wheezing attacks treated with short courses of oral corticosteroids, but who has no interval asthma symptoms.9
First-line preventer treatment in children under 5 with probable asthma and poor symptom control
In young children with symptoms uncontrolled by intermittent reliever use in whom maintenance therapy is being considered, regular daily inhaled corticosteroid is the first-line preventer of choice although both BTS/SIGN and NICE acknowledge that the evidence base is limited.
NICE recommends an 8-week trial of a paediatric moderate dose of ICS (‘Trial of treatment’). At the end of the 8 weeks, NICE advises stopping the ICS treatment and assessing the response and subsequent progress. If symptoms resolve on steroids but recur within 4 weeks of stopping, maintenance low-dose ICS should be started. If symptoms recur after 4 weeks then a further repeat trial of 8-week moderate-dose ICS is suggested. NICE’s recommendation to start at a paediatric moderate dose was driven by a need to be confident whether or not the symptoms were responsive to ICS.
For BTS/SIGN, a trial of ICS treatment with careful objective evaluation of the response is an integral part of the diagnostic process at all ages, with a good response supporting a diagnosis of asthma. The recommended starting dose of ICS should be appropriate to the severity of the disease and should then be titrated to the lowest dose at which control is maintained (noting that this will result in a ‘trial of withdrawal’ in children whose symptoms do not recur). BTS/SIGN highlights that in many children who have symptoms only with colds ‘watchful waiting with review’ may be a useful strategy, at least initially.
If asthma in children under 5 is uncontrolled on first-line preventer, what next?
At this stage, both NICE and BTS/SIGN state that evidence is very limited. BTS/SIGN notes that long-acting bronchodilators are not licensed under 4 years and evidence comparing ICS+LABA versus ICS+LTRA at this age is absent. Both NICE and BTS/SIGN recommend an LTRA in combination with low-dose ICS as the next step. If that fails, NICE suggests stopping the LTRA and referring to a clinician with expertise in asthma.
Conclusion
In considering the areas where differences occur between the recommendations made in BTS/SIGN and NICE guidelines, it is clear that close scrutiny of the evidence base shows that there is often more in common between the guidelines than might appear at first glance. It is hoped that this examination of the differences highlighted in this article will assist clinicians in making decisions with their patients.
Our understanding of asthma is evolving and our assessment of treatments must evolve with it. Further research to clarify the areas where data are currently limited or absent is urgently required in order that further updates can offer the best evidence-based advice.
Footnotes
Contributors All authors drafted and approved the final article.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.