Article Text

Abstract
Background Obstructive sleep apnoea (OSA) and obesity are interdependent chronic diseases sharing reduced exercise tolerance and high cardiovascular risk.
Intervention A 3-month intervention with innovative training modalities would further improve functional capacity and cardiovascular health than usual cycle exercise training in already continuous positive airway pressure (CPAP)-treated obese patients with OSA.
Methods Fifty three patients (35<body mass index (BMI) <45 kg/m2) were randomly allocated to exercise training on a cycle ergometer, either alone (ERGO) or with respiratory muscle training (ERGO+RMT) or non-invasive ventilation (ERGO+NIV). Changes in 6 min walking distance (primary outcome), aerobic capacity (VO2peak), cardiovascular parameters, body composition and sleep quality were evaluated.
Measurements and main results All training modalities increased 6 min walking distance without differences between groups (P=0.97). ERGO+NIV and ERGO+RMT led to significantly higher improvement in VO2peak compared with ERGO (3.1 (95% CI 1.6 to 4.6) vs 2.3 (0.8 to 3.7) vs 0.5(−1.0 to 1.9) mL/min/kg, respectively, P=0.04) and ERGO+NIV significantly reduced self-measured blood pressure compared with ERGO+RMT and ERGO (systolic: −9.5 (95% CI −14.1 to −4.9) vs −13 (−5.8 to 3.1) vs −0.7 (−5.1 to 3.8) mm Hg, respectively, P=0.01). Waist and neck circumferences were reduced after ERGO+NIV compared with ERGO+RMT and ERGO (P=0.01).
Conclusions Combining RMT or NIV with cycling exercise training failed to provide further improvement in functional capacity as compared with cycling exercise training alone. However, the combination of NIV and exercise training demonstrated superiority for improving cardiometabolic risk factors in obese CPAP-treated patients with OAS.
TRIAL REGISTRATION NUMBER Results, NCT01155271.
- sleep apnoea
- pulmonary rehabilitation
- respiratory muscles
Statistics from Altmetric.com
Key messages
What is the key question?
How can we optimise exercise training in obese CPAP-treated patients with obstructive sleep apnoea (OSA) to further improve functional capacity and cardiovascular outcomes?
What is the bottom line?
The addition of non-invasive ventilation or respiratory muscle training failed to further improve functional capacity (6 min walking distance) at 3 months in already CPAP-treated obese patients with OSA but these innovative training modalities were superior to improve aerobic capacity and self-measured blood pressure in these patients.
Why read on?
New training modalities must be considered for personalising training programmes in obese patients with OSA when targeting exercise tolerance and cardiovascular risk.
Introduction
Obesity and obstructive sleep apnoea (OSA) are highly prevalent and interdependent chronic diseases, both predisposing patients to metabolic and cardiovascular complications.1 2 In obese patients with OSA, spontaneous physical activity levels2 3 are reduced and the deleterious combination of OSA, obesity and inactivity constitutes a strong risk factor for type 2 diabetes and cardiovascular diseases.4
Continuous positive airway pressure (CPAP), the first-line therapy for OSA, suppresses abnormal respiratory events during sleep and drastically improves daytime sleepiness, neurocognitive function and quality of life.2 However, CPAP has a limited impact on OSA cardiovascular consequences particularly in secondary prevention (Sleep Apnoea Cardiovascular Endpoints (SAVE) study).5 In well-conducted randomised trials looking at circulatory markers of cardiometabolic risk, CPAP did not change glycaemic control, lipid profile or inflammatory status (for review see Jullian-Desayes et al 6). Also, although it improves alertness, fatigue and quality of life, CPAP has no significant effect on spontaneous physical activity.7 8 There is a need for multidimensional care modalities to reduce cardiometabolic risk and change lifestyle behaviours, particularly towards physical activity in patients with OSA who are often at high risk of cardiovascular complications.1 9
Exercise intolerance in obese patients with OSA can be explained not only by a combination of factors including impairment in respiratory mechanics and respiratory drive10 but also metabolic, cardiovascular and muscular factors that impact on aerobic capacity.11 Besides conventional ergocycle training, innovative and respiratory-centred rehabilitation programmes targeting specific disabilities common in obese patients with OSA have been proposed. Non-invasive ventilation (NIV) during exercise training reduces the work of breathing, enhancing exercise tolerance in patients with obstructive and restrictive pulmonary diseases including obesity.12 Also, a previous study in our laboratory demonstrated that respiratory muscle training (RMT) (isocapnic hyperpnoea) in addition to usual rehabilitation further improves walking distance in the obese individuals by increasing respiratory muscle endurance.13
The OBEX study was a randomised controlled trial designed to compare the effects of cycling exercise training alone (ERGO) or combined with NIV (ERGO+NIV) or RMT (ERGO+RMT) on exercise capacity and cardiometabolic parameters, in obese patients with OSA already treated with CPAP.
Methods
Study design and participants
In this parallel, three-arm, single-blind, randomised controlled trial, patients referred to sleep clinics by general practitioners and hospital specialists to two tertiary teaching hospital centres (Grenoble, France) and Quebec City, Canada) were assessed for eligibility. The trial was registered (ClinicalTrials.gov NCT01155271). Sixty patients fulfilling the following criteria were consecutively included: (1) adult patients diagnosed with OSA (apnoea hypopnoea index (AHI) >30/hour assessed by poly(somno)graphy); (2) already treated by CPAP for more than 1 month with compliance above 4 hour per night and (3) obesity (35< body mass index (BMI) <45 kg/m2). Patients having an unstable cardiovascular or respiratory disorder diagnosed within 3 months of screening or orthopaedic/neurological disease that might reduce spontaneous physical activity and limit the impact of a rehabilitation programme were not included. All patients provided written informed consent. A full trial protocol is available on request to the authors.
Randomisation and masking
After the run-in period, participants were randomly assigned (1:1:1) by a blinded statistician using a computer-generated allocation sequence to one of the following interventions: ERGO, ERGO+NIV, or ERGO+RMT. Randomisation was stratified by BMI (greater than or less than 40 kg/m2) and dyspnoea (greater than or less than 6/10) in blocks of 15 participants. The trial coordinator was informed of trial entry but not group allocation. Patients and physiotherapists/exercise specialist conducting the training programmes were informed of group allocation but investigators conducting clinical evaluation at month 3 were blinded to the patient’s study arm.
Procedures/interventions
All patients had a 6-week run-in period on CPAP alone and after randomisation attended 36 exercise training sessions, three sessions per week over 3 months. In France, one session per week was performed at home under the supervision by a physiotherapist. The three interventions were performed by the patients in sessions of 2–4 patients in the same time, allowing for the physiotherapist to take care of each patient separately. Exercise training session started with 30 min of cycling that was progressively increased to 45 min, according to the participant’s tolerance. Training intensity started at 60% of peak capacity (determined during the baseline incremental test). Sessions were supervised by a physiotherapist. In addition to exercise training, the ERGO+RMT group performed RMT after the cycling exercise sessions using a commercially available device (Spirotiger, Idiag AG, Fehraltorf, Switzerland). Briefly, the patient breathed in and out via a mouthpiece in this device which is connected to a rebreathing bag (50% vital capacity). A partial CO2 rebreathing assured an isocapnic hyperpnoea throughout the training session. The first target ventilation was set at 50% maximum voluntary ventilation capacity. Patients were requested to breath at a rate of 20 to 45–48 breaths/min and a tidal volume corresponding to half of their FVC. The device provides breath-by-breath visual feedback of tidal volume and breathing frequency allowing quality control of the training. RMT session length was increased progressively from 2×5 min to 2×15 min and supervised by a physiotherapist/exercise specialist.
The ERGO+NIV group received bilevel positive airway pressure ventilation via a full-face mask while performing ergocycle training (Trilogy 100, Phillips Respironics, Murrysville, USA). Mask and settings were adapted by a respiratory therapist and a pulmonologist to provide maximum support according to the patient’s comfort and tolerance. The ventilator was set on spontaneous mode. Initial settings (inspiratory/expiratory pressures) were set at 12 cm H2O/4 cm H2O. NIV parameters were adjusted based on the subjective sensation of each patient (dyspnoea, pressure level) and synchronisation with the device. Parameters were first suggested by the respiratory therapist before being checked by a pulmonologist. NIV settings used during cycling sessions were as follows: mean inspiratory positive airway pressure=19 (4) cm H2O, mean expiratory positive airway pressure=4 (1) cm H2O) and mean pressure support=14 (4) cm H2O. All patients were equipped with full-face mask.
Outcomes
Patients were evaluated on three occasions: at visit #1 (V1) at study entry, at visit #2 (V2) at the end of the run-in period and at visit 3 (V3), at the end of the 3-month intervention. The three visits were identical and included a 6 min walking test (6MWT), a cardiopulmonary exercise test, muscle testing, clinical measures and biomarkers of cardiometabolic risk, quality of life and daytime sleepiness questionnaires and physical activity measurements.
Primary outcome: six-minute walking distance (6MWD)
The primary outcome was the change in the 6MWD and end-of-test dyspnoea. The 6MWT was performed in an enclosed corridor on a 30m-long course, following the American Thoracic society guidelines.14 Distance walked during the 6MWT was recorded and the end-of-test dyspnoea and leg fatigue were assessed using visual analogue scales (VAS, range 0–10).
Secondary outcomes
Secondary outcomes included changes in aerobic capacity, cardiovascular parameters, body composition (fat-free mass index (FFMI)), sleep parameters, quality of life and physical activity. Furthermore, dietary intake was assessed in a subgroup of patients from the Grenoble’s centre (n=20).
Aerobic capacity
Aerobic capacity was assessed during a symptom-limited cardiopulmonary exercise, with breath by breath measurement of expired gases and ventilatory parameters (oxygen uptake (VO2), carbon dioxide excretion (VCO2) and minute ventilation (VE)) (Sensor Medics, Vmax Legacy, USA or Ergocard, Medisoft, Dinant, Belgium).
Quadriceps muscle strength and endurance
Quadriceps muscle strength and endurance (60% of the maximal voluntary contraction until exhaustion) were evaluated using a semirecumbent chair equipped with a strain gauge (Hewlett-Packard, Palo Alto, California, USA) with knee and hip angles of approximately 90° and 120°, respectively.
Cardiovascular outcomes
Cardiovascular parameters were blood pressure, pulse wave velocity (PWV) and endothelial function. Self-monitored blood pressure was measured at home, in sitting position on three consecutive days, with three measurements obtained 1 min apart on each occasion, according to European guidelines on hypertension,15 using a validated fully automated electronic device the Omron 705CP (Omron, Tokyo, Japan). Arterial stiffness was assessed by carotid-femoral PWV as measured with a Complior device (Artech Medical; Pantin, France).16 Endothelial function was assessed by reactive hyperaemia using finger plethysmography with an Endo-PAT device (Itamar Medical Ltd, Caesarea, Israel).17 Body composition was estimated using bioelectrical impedance (Bodystat 1500, Isle of Man, UK, in the French centre and InBody 570, Biospace, Seoul, Korea, in the Canadian centre).
Metabolic and inflammatory biomarkers
A panel of metabolic and inflammatory biomarkers was assessed. Plasma glucose and serum lipid concentrations were both measured using a Dimension Vista device by enzymatic methods (Siemens healthineers). Serum insulin was measured using an immunoradiometric assay (Bis-Insulin IRMA, CIS-Bio, France), and serum high-sensitivity C-reactive protein (hsCRP) was measured using automated immunonephelometry (Optilite analyser, The Binding site group, Birmingham, UK). The concentration of low density lipid (LDL) cholesterol was calculated using the Friedewald equation and the Homeostasis Model Assessment (HOMA) index with the formula HOMA=insulinaemia (mU/L)×glycaemia (mmol/L)/22.5.
CPAP measurements
Nocturnal oxygen saturation was measured by oximetry and mean daily CPAP usage and residual AHI were downloaded from the built-in software of the CPAP devices.
Quality of life questionnaire
The SF-36 questionnaire was used for quality of life assessment, and the Epworth scale was used to assess daytime sleepiness.
Physical activity and sleep quality
Lastly, sleep quality and duration, as well as spontaneous physical activity were recorded by accelerometer (SenseWear Pro2 armband; Bodymedia, Pittsburgh, Pennsylvania, USA). For the physical activity level, metabolic equivalent values have been corrected for obesity as previously reported in Vivodtzev et al.18
Statistical analysis
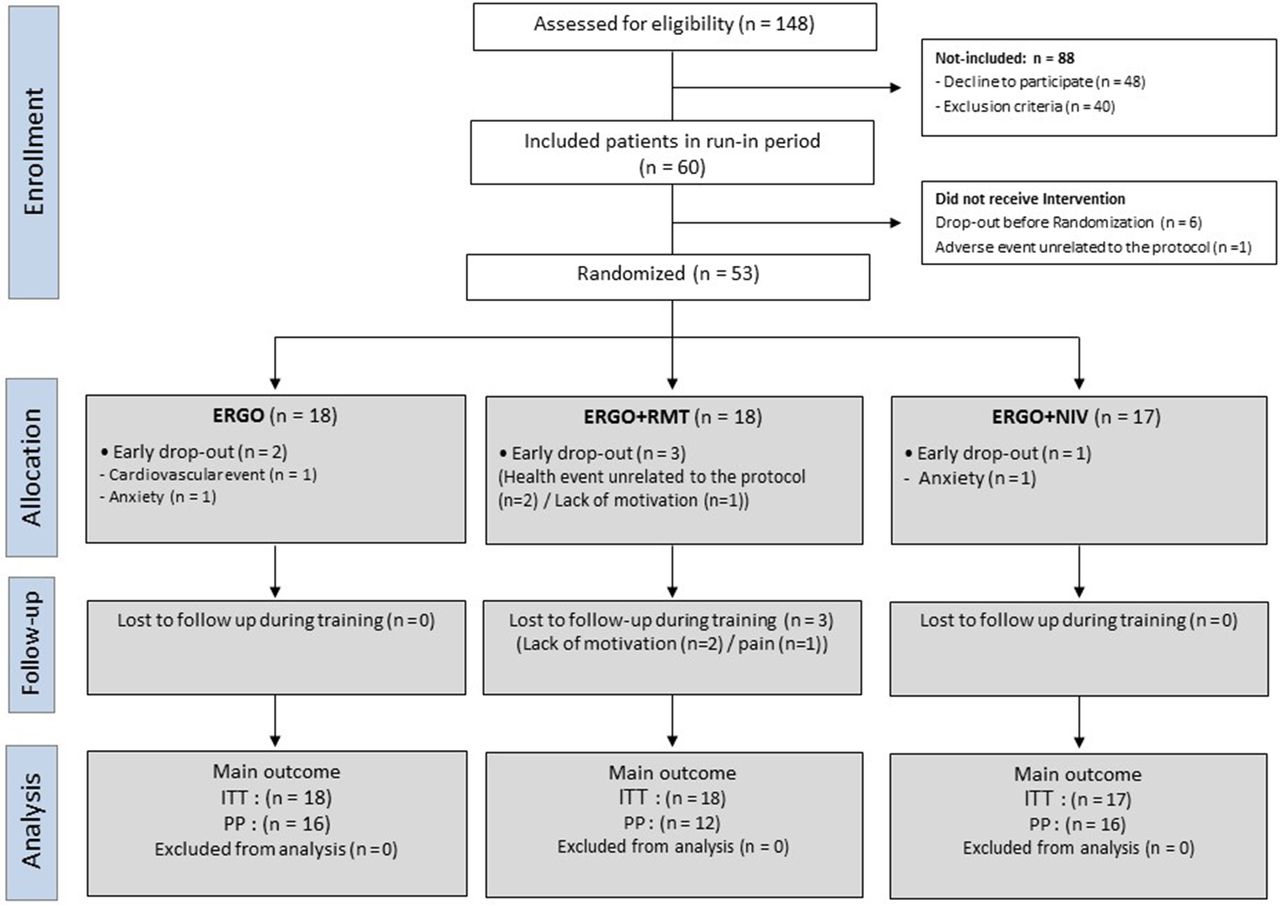
A previous study from our laboratory on morbidly obese patients showed that RMT performed in addition to an exercise training programme led to a greater improvement in 6MWD than exercise training.13 In the present study, we hypothesised that the combined training modalities (ERGO+RMT or ERGO+NIV) would increase 6MWD more than exercise training alone (expected difference: 50 m (±35)). The estimated sample size was 14 patients per group, based on a statistical significance threshold of 0.05 and power of 80%. Considering a 33% rate of non-compliance during training programmes for obese patients, the sample size was set at 20 patients per group, that is, a total of 60 patients. Data were initially analysed in intention to treat (ITT) including all subjects who completed the two pretraining visits and were randomised. Then, a per-protocol analysis was done on the subjects who completed the post-training visit (figure 1). Continuous data are presented as mean (95% CI) (text) or median and IQR (tables) and categorical data as frequency and percentage. Normality was assessed using Skewness and Kurtosis tests and equality of variance by Levene’s test. For all tests, a significance threshold of 0.05 was used. Missing values were replaced by the median for each group. For each study parameters, the baseline value corresponded to the average of the values obtained at V1 and V2, before the study intervention. A linear mixed effects model, with random effect by centre, was used to analyse (1) period (before and after training) and (2) group (ERGO, ERGO+RMT and ERGO+NIV) effect and the interaction (period*group) for all outcomes when the conditions of use of the analysis of variance were respected, otherwise a Kruskal-Wallis test was performed. Post hoc tests with Bonferroni correction were realised for the significant interactions (group*period). Correlations were assessed by Pearson’s coefficient. If assumptions for parametric tests were not evidenced, non-parametric alternatives were employed (Spearman’s coefficient). All statistical analyses were performed using SAS V.9.4 software.

Study flowchart. ERGO, ergocycle training; ITT, intention-to-treat; NIV, non-invasive ventilation; PP, per-protocol analysis; RMT, respiratory muscle training.
Results
Study flow chart and population studied
A study flow chart is shown in figure 1. Patients we enrolled between 7 July 2010 and 7 January 2014. Table 1 shows the anthropometric characteristics, exercise capacity and physical activity of the study participants. Patients had a mean age of 54 (SD 10) and were morbidly obese (mean BMI of 38 kg/m2 (SD 3)) with a high prevalence of comorbidities; 31 patients (52%) were treated for hypertension and 20 participants (33%) for dyslipidaemia. Mean baseline 6MWD was 547 m (SD 90) (105% predicted value (SD 15)). Aerobic capacity was in the lower end of normal values with a mean peak VO2 of 20.9 mL/min/kg (5.2) that corresponded to 77.8% of predicted values (SD 1.5). Table 2 shows the baseline sleep and cardiometabolic parameters of the study participants. CPAP therapy was efficacious with participants having a mean residual AHI of 3.5 events per hour (SD 2.4) and good observance to CPAP (mean CPAP usage of 6.9 hour/night (SD 1.2). Unexpected events are reported in the online Supplementary table E1.
Supplementary file 2
Baseline anthropometric characteristics, exercise capacity and physical activity of the ITT population
Baseline sleep and cardiometabolic parameters of the ITT population
Primary outcome analysis
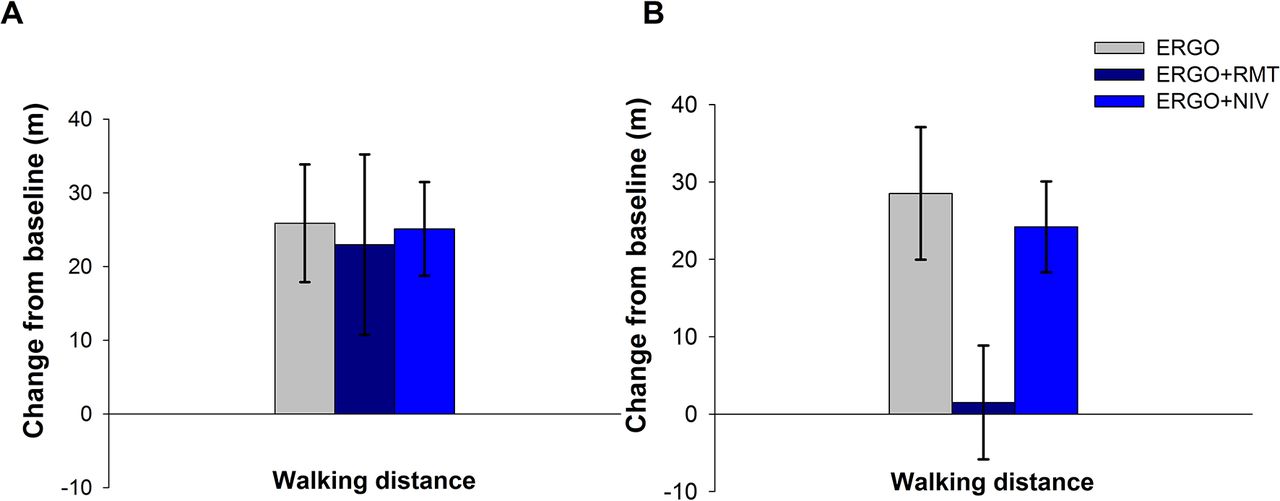
The ITT analysis revealed that the 6MWD and end-of-test dyspnoea improved in all three groups without significant difference between groups (figure 2A and table 3). In the per-protocol analysis, ERGO and ERGO+NIV training interventions led to a significant pre–post increase in 6MWD but not ERGO+RMT (figure 2B). Dyspnoea and leg discomfort also improved in all three groups without significant difference between groups (table 3).
Changes after training in 6MWD, aerobic capacity and muscle strength in the three intervention groups (ITT analysis)
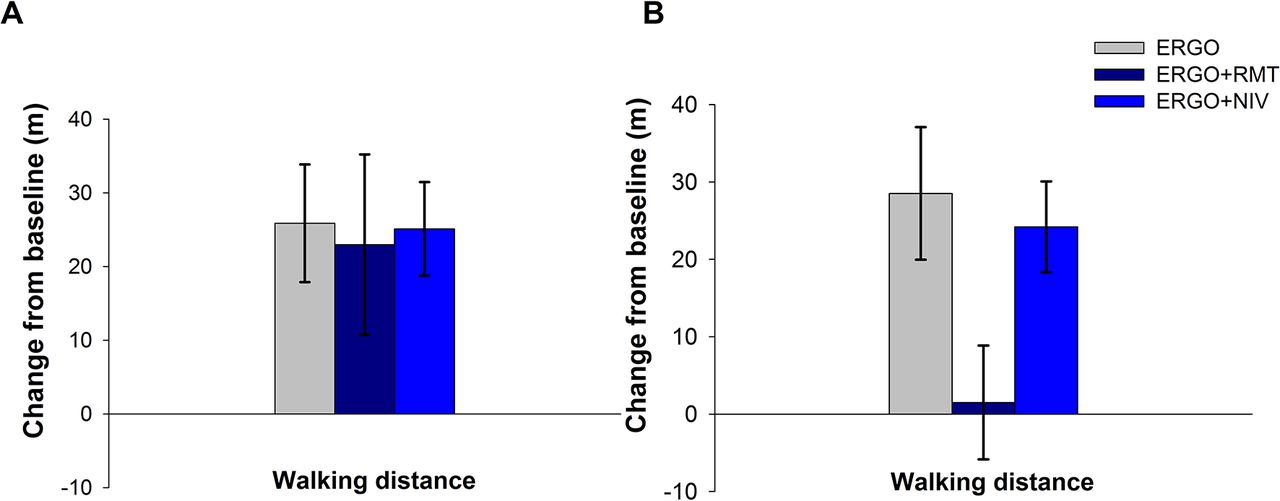
Postexercise training changes in the 6 min walking distance (6MWD) in the intention-to-treat population (Panel A) and in the per-protocol population (Panel B) in each of the three intervention groups. Bars represent SE. P values are for between-group differences in changes in walking distance. ERGO, ergocycle training; NIV, non-invasive ventilation; RMT, respiratory muscle training.
Secondary outcome analyses
Exercise tolerance
ERGO+NIV and ERGO+RMT training interventions led to significantly higher increases in peak oxygen consumption (VO2peak) compared with ERGO alone both in ITT analysis: 3.1 mL min−1 kg−1 (95% CI 1.6 to 4.6) versus 2.3 mL min−1 kg−1 (0.8 to 3.7) versus 0.5 mL min−1 kg−1 (−1.0 to 1.9), respectively, P=0.04 (figure 3A) and in per-protocol analysis (figure 3B). Significant differences between the three groups were also found in peak exercise VE and respiratory rate which were both significantly increased after ERGO+RMT only (table 3 and online Supplementary figure E1). Improvements in peak VO2 significantly correlated with those in peak VE (r=0.57, P<0.0001). No significant between-group differences were found for the changes in limb muscle strength and endurance after training or for respiratory muscle strength (table 3).
Supplementary file 1

Postexercise training changes in peak VO2 in the intention-to-treat population (Panel A) and in the per-protocol population (Panel B). Bars represent SE. P values are for between-group differences in changes in peak VO2. ERGO, ergocycle training; NIV, non-invasive ventilation; RMT, respiratory muscle training.
Cardiovascular and metabolic parameters
In ITT analysis, self-measured systolic blood pressure (SBP) and diastolic blood pressure (DBP) were significantly reduced after ERGO+NIV compared with ERGO+RMT and ERGO: SBP −9.5 mm Hg (95% CI −14.1 to −4.9) versus −1.3 mm Hg (−5.8 to 3.1) versus −0.7 mm Hg (−5.1 to 3.8), respectively (P=0.01) and DBP: −5.9 mm Hg (95% CI −9.8 to −2.1) versus 4.6 mm Hg (0.9 to 8.4) versus −1.7 mm Hg (−5.4 to 2.1), respectively (P=0.001) (figure 4A). This was confirmed in the per-protocol analysis (figure 4B).

Postexercise training changes in systolic (SBP)) and diastolic (DBP) self-measured blood pressure in the intention-to-treat population (Panel A), and in the per-protocol population (Panel B). Bars represent SE. P values are for between-group differences in changes in blood pressure. ERGO, ergocycle training; NIV, non-invasive ventilation; RMT, respiratory muscle training.
PWV was significantly reduced after training by an average of 0.5 m/s in the three groups but without significant difference between groups (table 3). No significant difference was found between groups in change in peripheral arterial tone.
No significant change was found in BMI after training in the three groups but waist and neck circumferences were significantly reduced after ERGO+NIV compared with ERGO and ERGO+RMT (waist: −5.3 (95% CI −8.2 to −2.4) vs −0.5 (−3.3 to 2.3) vs 0.7 (−2.2 to 3.5), respectively, and neck: −1.1 cm (95% CI −2.3 to 0) vs +1.0 cm (−0.1 to 2.1) vs +1.3 cm (0.2 to 2.4), respectively, P=0.01) (table 4 and figure 5). For the whole study population, after training there was a significant reduction (ITT analyses) in LDL to high density lipid cholesterol ratio (−0.02 (0.26), P=0.22), insulin blood level (−3.7 (12.4) µUI/mL, P=0.05) and HOMA index (−1.8 (5.9), P=0.03), compared with before training. hsCRP blood levels were also reduced after training in the whole study population in PP analysis (−1.4 (2.9) mg/L, P<0.001). There was no significant between-group difference for those parameters (table 4), but we found a significant correlation between changes in waist circumference and changes in the HOMA index (r=0.42, P=0.002).

{kind=link}
{kind=link}
![[SP1.jpg]](https://thorax.bmj.com/content/thoraxjnl/73/7/634/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
Postexercise training changes in waist and neck circumferences in the intention-to-treat population (Panel A) and in the per-protocol population (Panel B). Bars represent SE. P values are for between-group differences in changes in waist or neck circumferences. ERGO, ergocycle training; NIV, non-invasive ventilation; RMT, respiratory muscle training.
Changes after exercise training in body composition, physical activity, sleep and cardiometabolic parameters in the three intervention groups (ITT analysis)
FFMI and basal metabolism were improved after ERGO+RMT compared with ERGO and ERGO+NIV but only in the ITT analysis (table 4). This difference was lost in per-protocol analysis. In addition, no significant changes were found over the course in the training period in the dietary intake of the patients (data shown in the online Supplementary table E2).
No significant between-group differences were found between groups in sleep duration or number of steps per day after training. However, ERGO+NIV tended to reduce the time spent in a supine position by about 40 min/day compared with ERGO and ERGO+RMT in both ITT analysis (P=0.10) and per-protocol analysis (P=0.11) (table 4). Daytime somnolence and quality of life (SF-36) were improved after all three training programmes but without any significant differences between them.
Discussion
In obese patients with OSA, adjuncts to exercise training such as non-invasive ventilation or respiratory muscle training failed to demonstrate further improvement in the 6MWD as compared with cycle exercise training alone, after 3 months of training. However, non-invasive ventilation and respiratory muscle training in addition to ergocycle both led to greater improvements in peak aerobic capacity than ergocycle alone. Furthermore, non-invasive ventilation had the greatest impact on cardiometabolic risk with a dramatic reduction in blood pressure associated to a significant reduction waist and neck circumferences and a trend to significant decrease in time spent lying down. Our trial provides a rationale for personalising exercise training modalities in obese patients with OSA especially when cardiometabolic risk needs to be addressed.
Impact of the different training modalities on exercise tolerance
A recent meta-analysis reported benefits of training programmes for reducing OSA severity and improving sleep quality.19 Here we targeted obese patients with OSA already treated with CPAP. No significant additional effect of RMT or NIV added to exercise training was found in terms of our primary endpoint 6MWD in this population. RMT has been previously shown to provide greater improvement in 6MWD than usual exercise training alone in a rehabilitation centre, but in a more severely obese population (mean BMI: 45 kg/m2).13 In fact, it is likely that our group of patients were unexpectedly fit and that a subgroup of patients with higher cardiometabolic impairments compared with patients with OSA such as patients with obesity hypoventilation syndrome (OHS) may have been a more sensitive to the training effect on the 6MWD.20 The willingness to participate in rehabilitation programmes seems also to be different between OHS and classical OSA groups. It would be interesting to further investigate the cardiometabolic benefit of such interventions in patients with OHS.21
The improvement in aerobic capacity as assessed by VO2peak was significantly greater in with ERGO+RMT and ERGO+NIV compared with ERGO alone. Increases in aerobic capacities after RMT reported in patients with chronic obstructive pulmonary disease22 have been attributed to improvements in respiratory muscle endurance.22 In our study, we observed an increase in peak VE correlating with changes in peak VO2 suggesting that a greater respiratory muscle capacity was responsible for improved ability to perform exercise in these patients. One study has investigated the effect of proportional assisted ventilation during a single ergocycle session in patients with obesity.12 In this study, improvement in exercise tolerance with NIV was attributed to a reduced work of breathing, as also suggested by other investigators,23 to lesser diaphragm fatigue or reduced dyspnoea.24 Consistent with these observations, we observed a trend towards a significantly higher reduction in the end-of test dyspnoea score during the training programme in the ERGO+NIV group compared with the two other groups (P=0.06, table 2).
Impact of the different training modalities on cardio-metabolic outcomes
One strength of our study was to evaluate the effects of exercise training alone or in conjunction with RMT or NIV both on respiratory and cardiovascular endpoints. Whereas quality of life and daily functioning are clearly improved by CPAP in patients with OSA,2 prognosis and mortality in OSA are mainly related to cardiometabolic comorbidities.25 A recent network meta-analysis demonstrated only a limited effect of CPAP on blood pressure reduction.26 Moreover, a recent systematic review concluded that CPAP alone did not change glucose control, lipid profile or the proportion of patients with metabolic syndrome.6 As recently confirmed by the SAVE study,5 CPAP alone is unlikely to provide clinically relevant decreases in cardiometabolic risk. One important finding of our study, albeit a secondary endpoint, is that the use of NIV during exercise training allowed a dramatic reduction in SBP (−9.5 (10.8) mm Hg) and DBP (−5.9 (7.9) mm Hg), suggesting a more protective effect on cardiovascular function of this combined intervention than exercise training alone (figure 4).5 In comparison, a 4-month restrictive diet (decrease of 500 kcal/day) plus exercise training programme reduced SBP from 136 mm Hg (SD 65) to 125 mm Hg (SD 63) in patients with OSA and metabolic syndrome.27 This reduction in blood pressure effect is presumably related to reductions in basal sympathetic activity, enhancement of vagal activity and restoration of baroreflex sensitivity that are seen with exercise training.28 By relieving the respiratory muscles during exercise, it is likely that NIV changes the autonomic nervous system response during exercise and potentially baroreflex sensitivity leading to substantial reductions of blood pressure during the days following exercise training sessions.29
The prevalence of metabolic syndrome is very high in patients with OSA and the association of the two conditions has synergistic deleterious effects on hypertension and vascular remodelling.30 In this study, ERGO+NIV was the only training modality associated with a reduction in waist circumference, the main marker of visceral adiposity, a cardinal feature of the metabolic syndrome. One plausible explanation for this beneficial effect of ERGO+NIV training is the repetition of training sessions performed with a lower dyspnoea and fatigue, and the decrease in time spent lying down reflecting an overall increase in physical activity. Hence, although it deserves to be confirmed, it is likely that the utilisation of NIV during exercise would be of great interest for patients and clinicians into clinical practice. Such a strategy would be initially implemented in a hospital-setting rehabilitation programme and then being pursued in a self-supervised manner at home with the regular intervention of a physiotherapist. Tele rehabilitation would also be a way to support such a strategy.31
One potential limitation of our study is the relatively small sample size. Any effects of this small sample size on the power to detect between group changes may have been mitigated by the fact that all included patients were compliant with CPAP treatment and with the study interventions, avoiding confounding factors such as persistent sympathetic over-activation related to insufficient nightly usage. Thus, the reported effects can be attributed to the exercise training modalities. Another potential limitation which cannot be ruled out is the possibility of increased type I errors due to multiple secondary outcomes. The novelty of these exploratory results needs to be confirmed in future studies.
Conclusion
Studies exploiting data sets from large patient cohorts have used cluster analysis to identify distinct sleep apnoea phenotypes. Subgroups have been identified that varied considerably in age, sex, symptoms, obesity, comorbidities and environmental risk factors. The principal significant differences between clusters were minimally symptomatic versus sleepy patients with OSA, lean versus obese and among obese patients different combinations of comorbidities and environmental risk factors.32 33 There is a clear need for combined treatment strategies to improve the prognosis of severely comorbid obese patients with OSA. A combination of a weight loss intervention and CPAP has demonstrated synergistic effect on blood pressure, CRP and lipid profile.9 Our results open new avenues for personalised exercise training strategies in the context of comprehensive risk factor management plans for OSA and cardiometabolic diseases.
Acknowledgments
The authors are grateful to Marion Perrin and Meriem Benmerad for statistical analyses. We thank Alison Foote, PhD (employed by Grenoble Alpes University Hospital) for critically editing the manuscript.
References
Footnotes
Contributors IV, J-LP, FM and J-CB were involved in the literature search, study design, data collection, data analysis and interpretation, preparation of figures and/or writing. MC, AG and CM were responsible for the study design and data collection. Data collection, data interpretation and critical revision of the manuscript were done by RT, BW, PL and FS.
Funding This work was funded by the endowment fund ‘Agir pour les maladies chroniques’, France, an unrestricted grant from Philips and was also supported by the French National Research Agency (ANR) in the framework of the ‘Investissements d’avenir’ program (ANR-15-IDEX-02).
Competing interests IV reports personal fees and other from Invacare and salaries from Agiradom, all outside the submitted work. RT reports grants from Resmed, Philips and other from Agiradom, all outside the submitted work. J-CB reports grants and personal fees from Resmed and Philips, salaries from Agiradom and other from Nomics, all outside the submitted work. FM reports grants from GlaxoSmithKline, Boehringer Ingelheim, Novartis and AstraZeneca; personal fees from Novartis, Griffols, Boehringer Ingelheim and Novartis, all outside the submitted work. J-LP reports grants and personal fees from Resmed, Philips, Sefam, Agiradom, Vitalaire; personal fees from Elevie grants from Fisher & Paykel, Astra Zenecaand Bohringer, all outside the submitted work. MC, AG, BW CM, FS and PL have nothing to disclose.
Patient consent Obtained.
Ethics approval CPP Sud Est V (09-PROR-1), France and CER Laval Hospital (#20649), IUCPQ, Quebec, Canada.
Provenance and peer review Not commissioned; externally peer reviewed.