Article Text

Abstract
Rationale Breastfeeding protects from respiratory infections in early life but its relationship to recurrent cough and other respiratory outcomes in adult life is not well established.
Methods Infant feeding practices were assessed prospectively in the Tucson Children’s Respiratory Study, a non-selected birth cohort and categorised into formula from birth or introduced <1 month, formula introduced ≥1 to <4 months and exclusive breastfeeding for ≥4 months. Infant feeding was assessed as an ordinal variable representing an increasing dose of breastmilk across the three categories. Recurrent cough was defined at 22, 26 and 32 years as ≥2 episodes of cough without a cold lasting 1 week during the past year. Covariates included participant sex, race/ethnicity and smoking as well as parental smoking, education, age and asthma. Covariates were evaluated as potential confounders for the relation between infant feeding and adult outcomes.
Results Of the 786 participants, 19% breastfed <1 month, 50% breastfed ≥1 to <4 months and 31% breastfed ≥4 months. The prevalence of recurrent cough at 22, 26 and 32 years was 17%, 15% and 16%, respectively. Each ordinal increase in breastfeeding duration was associated with a decreased risk of recurrent cough in adult life: adjusted OR=0.71, (95% CI: 0.56 to 0.89), p=0.004. Additional adjustment for concurrent adult asthma, wheeze, smoking and lung volume did not change these results.
Conclusion Longer duration of breastfeeding reduces the risk of recurrent cough in adult life, regardless of smoking and other respiratory symptoms, suggesting long-term protective effects on respiratory health.
- asthma
- cough/mechanisms/pharmacology
Statistics from Altmetric.com
Key messages
What is the key question?
Does breastfeeding protect from respiratory symptoms in adult life?
What is the bottom line?
Longer duration of breastfeeding reduces the risk of recurrent cough in adult life, regardless of smoking and other respiratory symptoms, suggesting long-term protective effects on respiratory health.
Why read on?
To discover how infant feeding choices can have an impact on respiratory health in adult life.
Introduction
There is a large body of literature which considers the relation of infant feeding and respiratory symptoms in infancy, with most studies indicating that breastfeeding has a protective effect. Multiple studies have shown that longer duration of breastfeeding is associated with reduced prevalence of wheeze in infancy.1 2 A Dutch study3 showed that breastfeeding was associated in a dose relation with decreased risk of dry cough in the first 4 months of life, as well as wheezing, shortness of breath and persistent phlegm. Others2 have shown that the severity of lower respiratory illnesses (LRIs) in infancy was reduced with exclusive breastfeeding, and LRIs that occurred among breastfed infants were of shorter duration. A large meta-analysis of infant feeding and health outcomes4 showed lower ORs for cough and wheeze associated with breastfeeding in a dose–response pattern.
Whether breastfeeding provides similar protection against respiratory symptoms in later life is less well established. Despite showing a dose–response relation of breastfeeding to wheeze in the first 3 years of life, Elliott et al 5 found no significant association by age 7–8 in the large Avon Longitudinal Study of Parents and Children (ALSPAC) cohort. In a longitudinal follow-up of children aged 9–26 years, Sears6 found no evidence that breastfeeding protected against asthma. Similarly, in following a birth cohort of 1314 newborns up to age 20 in five German cities, Grabenhenrich et al 7 showed no association between breastfeeding and asthma. However, given that both wheeze and cough in early life are associated with later respiratory symptoms,8 it is possible that infant feeding practices may be associated with respiratory symptoms in adult life in the absence of a diagnosis of asthma.
Our aim was to determine if infant feeding patterns are associated with respiratory outcomes in adult life using data from the Tucson Children’s Respiratory Study, a large non-selected birth cohort in which infant feeding practices and adult health outcomes were ascertained prospectively. The population has been followed longitudinally to age 32, with questionnaires regarding cough, wheeze and asthma completed multiple times in adult life. We hypothesise that a longer duration of breastfeeding has a protective effect against respiratory symptoms in adult life.
Methods
Study design
Healthy infants were enrolled at birth in the Tucson Children’s Respiratory Study between 1980 and 1984 (n=1246).9 At enrolment, parents completed a questionnaire describing their race and ethnicity, history of physician-diagnosed asthma, years of education, current age and current smoking habits. Participant race and ethnicity were determined from this parental information and categorised as ‘non-Hispanic White’ (both parents), ‘Hispanic White’ (one or both parents) and all other race/ethnic groups combined into ‘Other’ (African American, Asian American, Native American and other). Parental education was defined as ≤12 years of education compared with >12 years of education, parental asthma as a report of physician-diagnosed asthma, parental smoking as actively smoking at the time of the child’s birth and parental age as ≤28 years old compared with >28 years old.
Infant feeding practices
Feeding practices were assessed prospectively based on forms completed by the child’s paediatrician at well-child visits at ages 2, 4, 6 and 9 months. Infant feeding was categorised into three groups as described previously10: formula provided from birth or introduced <1 month (‘Breastfed <1 month’), formula and/or food introduced between ≥1 to <4 months (‘Breastfed ≥1 to <4 months’) and exclusive breastfeeding for four or more months (‘Exclusive breastfed ≥4 months’).
Adult assessments
Questionnaires were completed at 22, 26 and 32 years of age. Recurrent cough was defined as two or more episodes of cough without a cold that lasted 1 week during the past year as previously reported for participants in this cohort.11 12 For recurrent cough, one episode of cough without a cold during the past year was combined with no cough group. A summary measure of the prevalence of adult recurrent cough between 22 and 32 years of age (‘Recurrent cough 22–32’) was defined as any report of recurrent cough at any adult age.
Active wheeze was defined as one or more episodes during the past year and active physician-diagnosed asthma as a report of a physician diagnosis of asthma and reported symptoms (asthma episodes or attacks and/or wheeze) during the past year. Active smoking was defined as any smoking in the past year, heart burn (acid or gastro-oesophageal reflux) as at least one reported episode during the past year, sinus trouble as a report of a physician diagnosis of sinus trouble with one or more episodes during the past year11 and allergic rhinitis as hay fever or runny, stuffy nose that a doctor said was allergic in nature. Adult body mass index (BMI) was calculated from self-reported height and weight at each age.
Lung volumes
Because we had previously found that longer duration of breastfeeding was associated with better FVC in childhood,10 we considered lung volume as a potential confounder. The FVC was determined from pulmonary function tests obtained at each adult age as described previously.13
Early life factors
Multiple early life factors were considered for their relations to infant feeding and recurrent cough as potential confounders. Respiratory syncytial virus (RSV) LRIs were identified from viral cultures of nasopharyngeal swabs and throat specimens collected during the acute phase of the illness as previously described.14 Cold air bronchial hyper-responsiveness (BHR) was measured at age 6 as previously defined.15 Early wheezing phenotypes were previously described as persistent wheezing (wheeze during lower respiratory tract illness before 3 years and wheeze at 6 years), late-onset wheezing (wheeze only at 6 years), transient early wheezing (wheeze only during lower respiratory tract illness before 3 years) and never wheezing.16 Atopy was defined as a positive skin-prick test to at least one of seven local aeroallergens (Bermuda grass, Alternaria alternata, careless weed, house-dust mix and mesquite, mulberry and olive-tree pollens).17
Statistical analysis
Infant feeding was evaluated as an ordinal variable (0, 1, 2) and as a categorical variable with the breastfed <1 month group considered as the reference group using logistic regression. The ordinal variable had a lower Akaike’s information criteria compared with the categorical infant feeding variable, so the first was used in all models as representing increasing duration of breastfeeding. Relations between breastfeeding duration and covariates or adult respiratory outcomes were assessed using contingency tables and the Χ2 statistic. A Mantel-Haenszel test of trend was computed for the unadjusted age-specific relation between breastfeeding duration and respiratory outcomes (IBM SPSS Statistics 24). ORs for each respiratory outcome were determined after adjustment using logistic regression. The generalised estimating equation, using an exchangeable correlation structure, was used to longitudinally assess the relation between breastfeeding duration and adult recurrent cough, asthma and wheeze (STATA 14). Models were adjusted for sex, race/ethnicity and parental smoking, education, age and asthma as fixed covariates and participant active smoking as a time-dependent covariate. This research was approved by the Institutional Review Board of the University of Arizona and informed consent/assent was obtained from/for all participants.
Results
Of the 1246 participants enrolled at birth, those with information for infant feeding and who completed one or more adult questionnaire were included in the current analysis (n=786). Of these, 503 completed all three questionnaires, 163 completed two questionnaires and 120 completed one questionnaire. Included participants (n=786) were more likely to have non-smoking parents with more years of education and to be non-Hispanic White, compared with those excluded from the current analysis because of missing data (n=460; online supplementary Etable 1). Parental history of asthma was similar for both groups.
Supplemental material
Infant feeding
Formula was introduced at birth or <1 month for 19.2% of the participants (n=151) and between ≥1 to <4 months for 49.6% of the participants (n=390), while 31.3% were exclusively breastfed ≥4 months (n=245) (table 1). Non-Hispanic White, non-smoking parents with more years of education were more likely to exclusively breastfeed ≥4 months (table 1). However, there was no relation between parental asthma and infant feeding choice (table 1).
Demographic characteristics of the infant feeding groups
Adult respiratory outcomes
The prevalence of recurrent cough, that is, two or more episodes of cough without a cold lasting 1 week during the past year, was similar at the three adult ages: 16.7% at 22 years, 14.7% at 26 years and 16.0% at 32 years, and the overall prevalence of adult recurrent cough reported between ages 22 and 32 was 28.4% (223/786) (online supplementary Etable 2). Of the participants who completed all three adult questionnaires (n=503), 165 reported recurrent cough at one or more times: 9.7% (n=16) at all three ages, 23.6% (n=39) at two ages and 66.7% (n=110) at one age. Of the socioeconomic or parental factors tested for potential confounding, only paternal asthma was associated with an increased risk of recurrent cough at age 22, but not at ages 26 or 32 (online supplementary Etable 2). Early life risk factors for asthma, such RSV LRI14 and persistent wheeze,16 were unrelated to recurrent cough in adult life (online supplementary Etable 3). Further, factors commonly associated with asthma such as cold air BHR and atopy at age 6 showed no consistent relation to recurrent cough (online supplementary Etable 3).
In adult life, participants who reported either recurrent cough or active wheeze were more likely to smoke compared with those without such symptoms (table 2). In contrast, adult asthma was unrelated to concurrent smoking. Recurrent cough was associated with active wheeze and asthma at each age (online supplementary Etable 4). In addition, adults with recurrent cough reported rhinitis, sinus trouble and heart burn more often that those without recurrent cough (online supplementary Etable 4). There was no relation between recurrent cough and concurrent BMI at 22, 26 or 32 (data not shown).
Prevalence of active smoking at ages 22, 26 and 32 years by concurrent respiratory symptoms
Infant feeding and recurrent cough
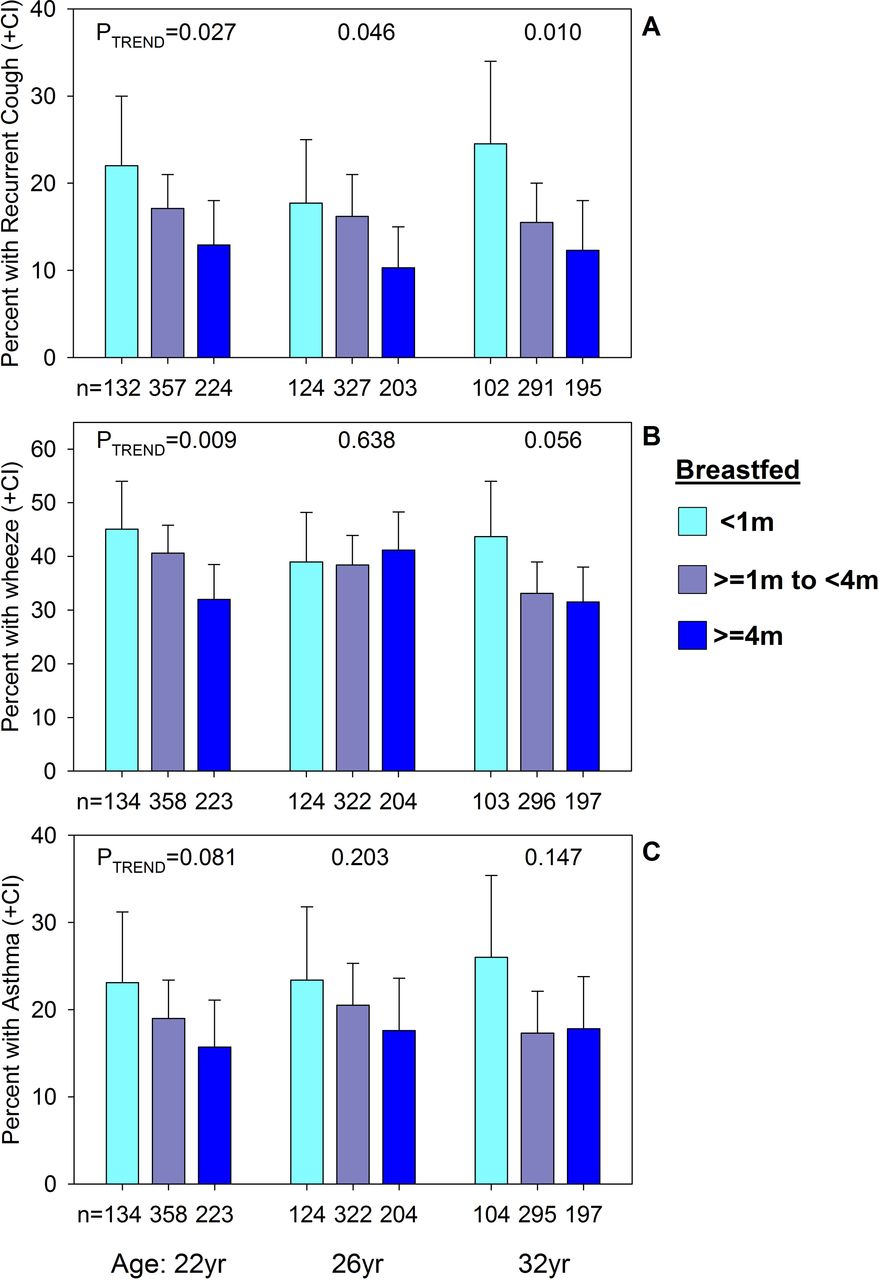
In unadjusted age-specific analyses (figure 1), there was a significant protective effect for increasing duration of breastfeeding on recurrent cough at all three adult ages. The same effect was also evident for wheeze at age 22, but not at ages 26 or 32 years. No statistically significant association was observed between infant feeding considered as an ordinal variable representing an increasing breastfeeding duration and active adult asthma. At age 22, those in the early formula group were more likely to smoke compared with those with more breastfeeding (online supplementary Etable 5). However, by ages 26 and 32, infant feeding showed no relation to active adult smoking.

{kind=link}
Association of infant feeding and adult recurrent cough (A), wheeze (B) and asthma (C) at ages 22, 26 and 32 years; proportions compared across the ordinal infant feeding categories using a Mantel-Haenszel test of trend.
After adjusting for sex, race/ethnicity and current smoking as well as maternal and paternal smoking, education, age and asthma in age-specific models, a similar protective effect for increasing duration of breastfeeding on recurrent cough was present at all ages. For each ordinal increase in breastfeeding duration, there was a corresponding decreased risk of recurrent cough in adult life at age 22 (adjusted OR (aOR)=0.72, (95% CI: 0.52 to 1.00); p=0.049, n=668) and age 32 (aOR=0.65, (95% CI: 0.44 to 0.94); p=0.021, n=549). At age 26, there was a similar trend, though it was not statistically significant (aOR=0.75, (95% CI: 0.53 to 1.06); p=0.108, n=611) (full models shown in online supplementary Etable 6).
Longitudinal models were used to assess the relation of breastfeeding duration to recurrent cough over the 22–32 age span. There was a significant protective relation between breastfeeding duration and recurrent cough between ages 22 and 32 (aOR=0.71, (95% CI: 0.56 to 0.89); p=0.004, 735 subjects, 1828 observations) after adjusting for sex, race/ethnicity, active current smoking as well as parental smoking, education, age and asthma (online supplementary Etable 6). Additional adjustment of this basic model for the relation between breastfeeding duration and recurrent cough with concurrent adult asthma, wheeze and lung volume (FVC) did not appreciably change the results (aOR=0.69, (95% CI: 0.50 to 0.94); p=0.019, 560 subjects, 1122 observations). Further adjustment of this basic model with concurrent BMI did not change the results (aOR=0.68, (95% CI: 0.54 to 0.86); p=0.002, 732 subjects, 1769 observations). There was no statistically significant relation between breastfeeding duration considered as an ordinal variable and adult wheeze (aOR=0.89, (95% CI: 0.73 to 1.07); p=0.203) or asthma (aOR=0.86, (95% CI: 0.66 to 1.12); p=0.267) between ages 22 and 32 years in adjusted longitudinal models.
There were no significant interactions between breastfeeding duration and the main covariates: sex, race/ethnicity, active current smoking and parental smoking, education, age and asthma (data not shown). There were also no interactions between breastfeeding duration and the early life risk factors: RSV, wheezing phenotypes, cold air hyper-responsiveness or atopy (data not shown).
Discussion
This analysis demonstrates that a longer duration of breastfeeding is associated with lower prevalence of recurrent cough in adulthood 22–32 years later. While wheeze at age 22 was also reduced in association with longer breastfeeding, this relationship did not account for the significant relation with recurrent cough. The relation between feeding and recurrent cough could not be attributed to group differences between those who did and did not breastfeed exclusively as these differences were controlled in analyses.
There is significant evidence that breastfeeding is associated with reduced acute respiratory symptoms in infancy and early childhood. In addition to studies which show a reduced prevalence of cough3 and/or wheeze in infancy1 2 associated with breastfeeding, there is evidence of reduced respiratory symptoms into the preschool years. A Finnish study18 showed a dose–response relation between duration of exclusive breastfeeding and persistent cough up to 7–9 months, although adjusted odds for cough increased with increasing breastfeeding after that age, suggesting the presence of unmeasured confounders. Sucharew et al 19 showed that recurrent night cough to age 3 was less common among breastfed children, although when wheezing was included in the model the relation with breastfeeding became non-significant. We have previously shown in this same cohort that longer duration of breastfeeding is associated with reduced prevalence of wheeze to age 6 years among non-atopic children.20 However, to our knowledge, there has been no previous report of an association of infant feeding and prevalence of cough or other respiratory symptoms in adult life independent of a diagnosis of asthma.
Whether breastfeeding reduces risk for asthma is controversial. Although a meta-analysis found that exclusive breastfeeding was associated with a lower risk of asthma between ages 2 and 521, we, and others, have shown prospectively that the relation to asthma in late childhood is far from simple and that maternal characteristics may alter the effect.14 22 In the current analysis, subjects with recurrent cough are more likely to report wheeze, asthma, rhinitis, sinusitis and heart burn. However, they are no more likely to be atopic than subjects without recurrent cough consistent with our earlier observations about recurrent cough without wheeze in childhood.12 Further, the relation with recurrent cough was independent of asthma, and adjusting for the other conditions did not change the relationship observed. This suggests that adult recurrent cough is not cough-variant asthma but rather a different phenotype, potentially the tip of the iceberg for later respiratory morbidity.
Cough is common in childhood8 and typically occurs in association with acute respiratory infections. Although this symptom has received little attention relative to wheeze, we have recently shown that recurrent cough in infancy is a risk factor for subsequent asthma.8 In adult life, however, recurrent cough may be an early manifestation of airway obstruction. In the older National Health and Nutrition Examination Survey population,23 individuals with recurrent cough, defined as ‘usual cough on most days for 3 consecutive months or more during the past year,’ were more likely have moderate to severe obstruction and to report fair/poor health than those with no symptoms. Symptomatic mild obstruction is associated with a faster decline in FEV1 and greater utilisation of healthcare services for respiratory outcomes24 relative to subjects without symptomatic mild obstruction. These results suggest that chronic respiratory symptoms in adulthood may be risk factors for both morbidity and poor quality of life even in the absence of a diagnosis, thereby warranting research into their early life predictors. Recurrent cough is also associated with cigarette smoking25 that often precedes development of airflow obstruction.26 In our study, although smoking was more common among subjects with recurrent cough, adjusting for smoking did not alter the relation with breastfeeding.
There may be several possible biological explanations for the association of infant feeding practices with recurrent cough in adult life. First, it is possible that early respiratory illnesses increase risk for later respiratory symptoms, and the protective effect of breastfeeding on the former may reduce the risk for the latter. In this cohort, however, neither early wheezing LRIs nor RSV LRIs were associated with recurrent cough in adult life, indicating that they cannot account for the relation of infant feeding to adult cough. Second, it has been shown that some components of human milk are associated with epigenetic changes in infancy, but the mechanisms involved are still unclear27 and any link between epigenetic changes and subsequent risk for cough or other respiratory symptoms in adult life remains to be elucidated. Other studies have suggested that the use of a bottle, particularly for feeding in the crib prior to sleep,28 regardless of content, may be as important as what is in the bottle in conferring risk for cough and wheezing in infancy. Soto-Ramirez et al 29 showed that infants who are exposed to the bottle, even when they are receiving human milk, are more likely to experience cough and wheeze in infancy, suggesting that bottle feeding may result in regurgitation and aspiration, which could lead to increased mucous production in the airways. While we do not have data on Tucson Children’s Respiratory Study subjects as to whether exclusively breastfed infants were ever fed with a bottle, there was no relation of early cough with later recurrent cough. Finally, breastfeeding has been shown to bear a relation with subsequent lung function, with some studies documenting larger lung volumes in adolescence10 30 as well as an increased FEV1/FVC31 associated with breastfeeding. Adjusting our models for lung volume did not alter the results. Although the mechanism for the observed relation is unclear, studies have shown a relation of infant feeding practices to other adult health outcomes such as Crohn’s disease or metabolic syndrome, providing support that such a long-term effect is plausible.32–35
This analysis has several potential limitations. First, there are multiple differences between mothers who breastfeed and those who do not. While we adjusted for key factors such as education and age, there may be other unmeasured differences that could have contributed to the observed effect. Second, the results relied on self-report of symptoms in adult life, which may be affected by reporting bias associated with asthma; however, the relation persisted when asthma was included as a potential confounder in multivariate analyses. Third, subjects with recurrent cough were also more likely to have other symptoms and diagnoses, raising the possibility that the effect is not specific to recurrent cough. Adjusting for these other symptoms did not alter the results. In addition, study participants who were breastfed for longer were more likely to still be participating in the study at age 32 (80%) compared with those breastfed for the intermediate (75%) and shortest duration (68%). However, the proportions responding at ages 22 and 26 were roughly comparable between the high and low breastfeeding groups, and the trends with recurrent cough are in the same direction and of comparable magnitude at all ages. Strengths of the study include the prospective assessment of infant feeding practices, the high participation rate, the consistency of findings across the adult ages and the extensive follow-up of this non-selected population.
In conclusion, this analysis documents a protective relation between breastfeeding in early life and recurrent cough at ages 22–32. Longer duration of breastfeeding is associated with a dose-related reduced prevalence of adult recurrent cough, suggesting potential long-term protective effects on respiratory health. Future research should consider relations of breastfeeding with adult symptoms and conditions, to ascertain whether this behaviour in early life is associated with alterations in adult health beyond the protection it provides in infancy.
References
Footnotes
Contributors Study concept and design: FDM, ALW, DAS and KDG; participant recruitment: ALW; acquisition of data: ALW, FDM and WJM; analysis of data: DAS, KDG, SG, WJM and FDM; data interpretation and drafting of the manuscript: KDG, DAS, SG, WJM, ALW and FDM. All authors critically read, commented on and approved the final version of the manuscript.
Funding This work was supported by US Department of Health and Human Services, National Institutes of Health, National Heart Blood and Lung Institute grant number 132523.
Competing interests None declared.
Patient consent Not required.
Ethics approval This research was approved by the institutional review board of the University of Arizona.
Provenance and peer review Not commissioned; externally peer reviewed.