Article Text

Statistics from Altmetric.com
Case
A 58-year-old woman with a 40 pack-year smoking history presented with several weeks of shortness of breath, chest pain radiating to the back and a hoarse voice. Initial chest X-ray showed a new left upper lobe mass concerning for malignancy. She then underwent positron emission tomography(PET)-CT, which revealed a fluorodeoxyglucose (FDG)-avid left hilar lung mass, (figure 1, red arrow) and left supraclavicular and mediastinal lymphadenopathy (figure 1, orange and green arrows). The PET-CT also showed asymmetric FDG uptake of the vocal folds at the level of the thyroid cartilage (right greater than left), suggestive of left vocal fold paralysis (figure 2, yellow arrow). A CT image of the vocal folds is depicted in figure 3.
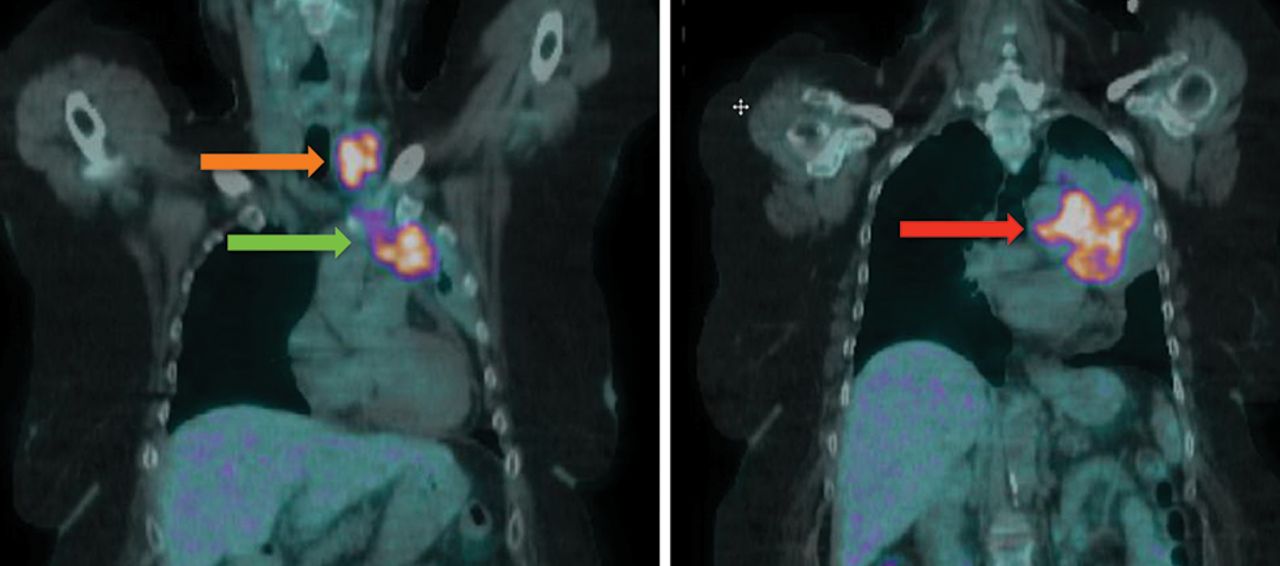
PET-CT of the chest showing FDG-avid left hilar mass (red arrow) and left supraclavicular and mediastinal lymphadenopathy (orange and green arrows). FDG, fluorodeoxyglucose; PET, positron emission tomography.

PET-CT showing asymmetric FDG uptake of vocal folds at the level of the thyroid cartilage (yellow arrow). FDG, fluorodeoxyglucose; PET, positron emission tomography.

{kind=link}
{kind=link}
{kind=link}
CT of the vocal folds at the level of the thyroid cartilage.
Such asymmetric FDG uptake as seen in this patient is thought to result from decreased and increased glucose consumption by the paralysed and functioning vocal folds, respectively. Asymmetry in FDG uptake is more prominent when paralysis is acute or subacute rather than chronic.1 The most likely aetiology of vocal fold paralysis in this patient was compression of the left recurrent laryngeal nerve by either the hilar lung mass or the associated mediastinal lymphadenopathy. This nerve courses below the aortic arch posterior to the ligamentum arteriosum, which appears to correspond to the area where the hilar mass and mediastinal lymphadenopathy were located.2 It is more common to see left rather than right recurrent laryngeal nerve compression due to its longer course and passage through the aortopulmonary window. Such compression would explain the patient’s complaint of hoarseness, which is commonly the earliest sign of compression or invasion of the recurrent laryngeal nerve.
The patient underwent endoscopic biopsy, which revealed small cell lung carcinoma. Further invasive assessment to evaluate hoarseness was not needed, as the PET-CT was diagnostic. She was determined to have limited stage small cell lung carcinoma, and was started on cisplatin and etoposide as an inpatient to minimise symptoms and reduce disease burden. Chemotherapy plus radiation therapy were continued as an outpatient. After about 1 month of therapy, the patient reported improvement in both dyspnoea and hoarseness.
Footnotes
Contributors Drs CM, ZAKF, BO and AZC all contributed to the planning, conduct and reporting of the manuscript. Dr CM is responsible for the overall content as guarantor.
Competing interests None declared.
Patient consent Obtained
Provenance and peer review Not commissioned; externally peer reviewed.