Article Text

Abstract
Background: Patients with obstructive sleep apnoea syndrome (OSAS) often display persistent cognitive dysfunction despite effective treatment with continuous positive airway pressure (CPAP). Brain-derived neurotrophic factor (BDNF) is a key mediator of memory and cognition, but its regulation in OSAS and during CPAP treatment is unknown.
Methods: Serum and plasma BDNF concentrations, BDNF secretion by peripheral blood mononuclear cells, and overnight polysomnography were evaluated in 17 men with newly diagnosed OSAS (as defined by a respiratory disturbance index of >10/hour with >70% obstructive events and corresponding daytime symptoms) and 12 healthy control men. In the patients all the parameters were monitored after 1 night and 3 months of CPAP treatment.
Results: There was no significant difference in baseline serum BDNF, plasma BDNF, or spontaneous BDNF secretion by peripheral blood mononuclear cells between untreated patients and controls. After 1 night of CPAP treatment there was a steep fall in median serum BDNF (from 18.0 ng/ml to 4.1 ng/ml) and plasma BDNF (from 58.7 pg/ml to 22.0 pg/ml) concentrations. Following 3 months of treatment BDNF concentrations did not return to baseline. In contrast, BDNF secretion was not suppressed by CPAP treatment.
Conclusions: Patients with untreated OSAS have normal serum and plasma BDNF levels. CPAP treatment is associated with a rapid decrease in serum and plasma BDNF levels which may reflect enhanced neuronal demand for BDNF in this condition.
- BDNF, brain-derived neurotrophic factor
- CPAP, continuous positive airway pressure
- ESS, Epworth Sleepiness Scale
- 5-HT, 5-hydroxytryptamine
- OSAS, obstructive sleep apnoea syndrome
- RDI, respiratory disturbance index
- TGFβ1, transforming growth factor β1
- obstructive sleep apnoea syndrome
- brain derived neurotrophic factor (BDNF)
- continuous positive airway pressure (CPAP)
Statistics from Altmetric.com
- BDNF, brain-derived neurotrophic factor
- CPAP, continuous positive airway pressure
- ESS, Epworth Sleepiness Scale
- 5-HT, 5-hydroxytryptamine
- OSAS, obstructive sleep apnoea syndrome
- RDI, respiratory disturbance index
- TGFβ1, transforming growth factor β1
- obstructive sleep apnoea syndrome
- brain derived neurotrophic factor (BDNF)
- continuous positive airway pressure (CPAP)
The obstructive sleep apnoea syndrome (OSAS) is a major public health burden, with a worldwide prevalence of 4–6% among middle aged men.1,2 OSAS is characterised by repeated airflow interruptions during sleep resulting in oxyhaemoglobin desaturations, sleep fragmentation, and functional impairment such as daytime hypersomnolence and cognitive dysfunction.3 Cognitive dysfunction in OSAS includes deficits in memory, problem solving, and behavioural functioning.4 The precise mechanisms underlying these changes are, as yet, unclear. Although sleep parameters can rapidly be normalised with continuous positive airway pressure (CPAP) treatment, deficits in cognitive performance often persist.5 In addition, the effectiveness of CPAP does not correlate with neuropsychological improvement.6 Thus, the relationship between CPAP treatment and cerebral dysfunction is still poorly understood.5
Brain-derived neurotrophic factor (BDNF) is a key mediator of neuronal and synaptic plasticity in adults.7 It induces long term changes in synaptic composition, ion channel expression, and neurotransmitter production in neuronal structures of the brain.8,9 Neuronal plasticity mediated by BDNF has been shown to be essential for cognitive functions and the consolidation of memory.10 Reduced BDNF levels in the human brain are associated with cognitive deficits, impaired memory performance, and depression.11,12 Substantial amounts of BDNF are stored in circulating human platelets (as reflected by high serum levels of BDNF), whereas low amounts of BDNF are found in human plasma.13,14 There is evidence that peripheral blood BDNF levels relate to BDNF concentrations in the central nervous system.15,16 This is in line with the finding that BDNF readily crosses the blood-brain barrier.17 Despite the fact that sleep is essential for memory consolidation and the facilitation of learning,18 very few data are available on BDNF regulation during sleep. Animal data suggest that sleep related neuroplasticity is associated with enhanced BDNF production and demand in the brain.19,20 In addition, it has been speculated that the interplay between sleep and cognition might involve BDNF.21 However, the regulation of BDNF in OSAS and during CPAP therapy is unknown. A study was therefore undertaken to investigate this regulation in a clinical setting.
METHODS
Study design
Twenty one men with newly diagnosed OSAS (inclusion criteria: respiratory disturbance index (RDI) >10/hour, >70% obstructive events, and corresponding daytime symptoms) were recruited. Seventeen male volunteers were recruited as presumably healthy controls (inclusion criteria: no history of snoring, sleep related breathing disorders, or daytime sleepiness). For both patients and controls, exclusion criteria were as follows: (1) any history of a malignant disease; (2) any chronic disease or medication having a major impact on the central nervous system or immune system; (3) signs or symptoms of an intercurrent infection. Before enrollment, participating subjects gave their written informed consent and answered a questionnaire regarding daytime sleepiness (Epworth Sleepiness Scale, ESS) and their medical history. The study was approved by the local ethics committee.
Both patients and controls underwent diagnostic overnight polysomnography using the Alice 3 polysomnography system (Heinen and Löwenstein, Bad Ems, Germany). Sleep measurements during polysomnography included standard electroencephalography (EEG), electrooculography (EOG) and electromyography (EMG) via electrodes.22 In addition, nasal airflow was measured using a thermistor, and oxygen saturation using pulse oxymetry. Respiratory effort was analysed with thoracic and abdominal gauges. Following polysomnography, sleep stages and respiratory events were visually analysed and edited page by page following standard criteria of the American Academy of Sleep Medicine.22,23
In patients, the diagnostic night was followed directly by the first night with CPAP (1 night CPAP) and further polysomnographic monitoring after 3 months of CPAP treatment (3 months CPAP). CPAP titration was performed manually in the first treatment night and, if necessary, also during the control night. CPAP was applied using commercially available devices (SOMNOcomfort, Weinmann, Hamburg, Germany or CPAP S6, ResMed, Mönchengladbach, Germany). Compliance was measured using integrated hour counters in CPAP devices and appropriate compliance software.
Blood parameters and cell culture
Blood was drawn from the cubital vein in the morning at 06.00 hours following each polysomnography (while the patients and controls were still lying in the bed) into heparinised (plasma), additive free (serum) and EDTA containing (for cell separation and blood cell counts) containers and placed on ice immediately. Heparinised (plasma) and additive free (serum) containers were placed on ice for 60 minutes. Afterwards, serum and plasma samples were obtained by centrifugation for 15 minutes (2000 g, 4°C) and stored at −80°C until measured.14 Differential blood cell counts, serotonin (5-hydroxytryptamine, 5-HT), BDNF, and transforming growth factor β1 (TGFβ1) were measured as described previously.14 Monocyte enriched peripheral blood mononuclear cells were isolated for cell culture experiments as previously described,24 and 2×106 cells/ml were cultured in RPMI 1640 with 10% fetal calf serum, 100 U/ml penicillin, and 100 µg/ml streptomycin for 48 hours. Supernatants were aliquoted and stored at −80°C until measured.
Statistical analysis
Data were analysed using SPSS (SPSS Inc, Chicago, IL, USA). Most parameters were non-normally distributed so the Mann-Whitney U test was chosen for the comparison of groups (patients versus controls). For comparisons within patients at different time points, repeated measures ANOVA for related samples was used. Correlations were calculated using Spearman’s correlation coefficient. p values of <0.05 were regarded as significant.
RESULTS
Sleep characteristics and CPAP treatment
Four patients did not appear for the scheduled polysomnography after 3 months of CPAP treatment and were therefore excluded from the study. In the group of healthy controls, five volunteers had to be excluded due to sleep related respiratory events >10/hour during polysomnography. A final number of 17 men with sleep apnoea (mean (SD) body mass index 33.9 (4.1) kg/m2, mean (SD) age 55.6 (10.5) years) and 12 healthy male volunteers with proven absence of sleep apnoea (mean (SD) body mass index 24.4 (3.1) kg/m2, mean (SD) age 48.5 (8.2) years) were therefore evaluated. Two patients were included despite ESS values of less than 10. One patient was not holding a driving licence so the last question of the ESS was not applicable. The other patient suffered from drowsiness and sleepiness in situations demanding at least average attentiveness; his sleepiness was therefore considered clinically relevant. Patients were found to have medium (RDI >15/hour) to severe (RDI >30/hour) OSAS (table 1).23 The median percentage of obstructive events was 99% (minimum 83%, maximum 100%). Following 1 night of CPAP treatment, almost all sleep parameters (except for slow wave sleep, SWS) were significantly improved and not significantly different from controls (p>0.05 for all parameters, table 1). In all of the 17 patients included in the analysis, CPAP devices were used >4 hours per night over the whole time period of 3 months. There were no significant changes in sleep parameters after 3 months of treatment with CPAP compared with the first night of treatment. There were no significant differences in sleep parameters between controls and patients after 3 months of CPAP treatment (table 1).
Sleep characteristics in patients and controls
BDNF levels in serum and plasma
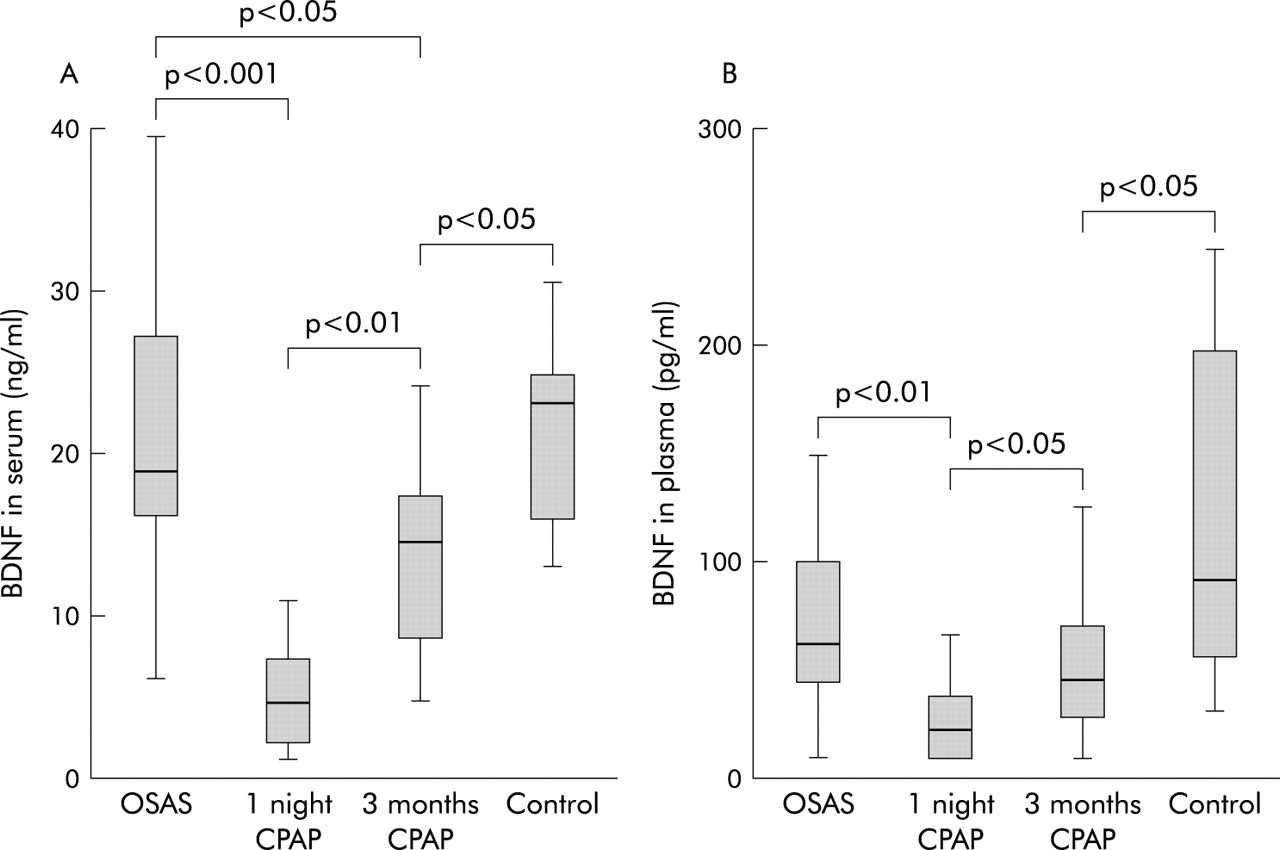
Before starting CPAP treatment there were no significant differences in serum and plasma BDNF levels between patients and controls (fig 1A, B). Serum and plasma BDNF levels in controls were in keeping with previous data obtained from a large group of healthy adults.14 After the first night of CPAP treatment, median BDNF serum concentrations decreased from 18 ng/ml (interquartile range (IQR) 16.2–26.4) to 4.1 ng/ml (IQR 2.4–9.0) (fig 1A). Median BDNF plasma concentrations decreased from 58.7 pg/ml (IQR 35.4–129.3) to 22.0 pg/ml (IQR 8.0–37.6) (fig 1B). After 3 months of CPAP treatment, a significant increase in BDNF concentrations was found (compared with BDNF concentrations after the first night of CPAP treatment). However, serum and plasma BDNF levels were still lower than in controls. Serum (but not plasma) BDNF levels were still significantly lower than before CPAP treatment (fig 1). In patients with untreated OSAS there was no significant correlation between BDNF levels and the RDI (serum BDNF: r = 0.32, p = 0.27; plasma BDNF: r = 0.39, p = 0.19) or the ESS (serum BDNF: r = 0.14, p = 0.62; plasma BDNF: r = 0.10, p = 0.73). During CPAP treatment there were no significant correlations between sleep parameters or CPAP compliance and BDNF serum or plasma levels in patients with OSAS (data not shown).

(A) Serum and (B) plasma concentrations of brain-derived neurotrophic factor (BDNF) in controls and patients with OSAS after the diagnostic night without CPAP (OSAS), after the following night with CPAP (1 night CPAP), and after 3 months of CPAP treatment (3 months CPAP). Box plot graphs display the median (line within the box), interquartile range (edges of the box), and the range of all values less distant than 1.5 interquartile ranges from the upper or lower quartile (vertical lines). Significant differences between groups or time points are marked with p values (levels of significance).
Platelet counts and platelet markers
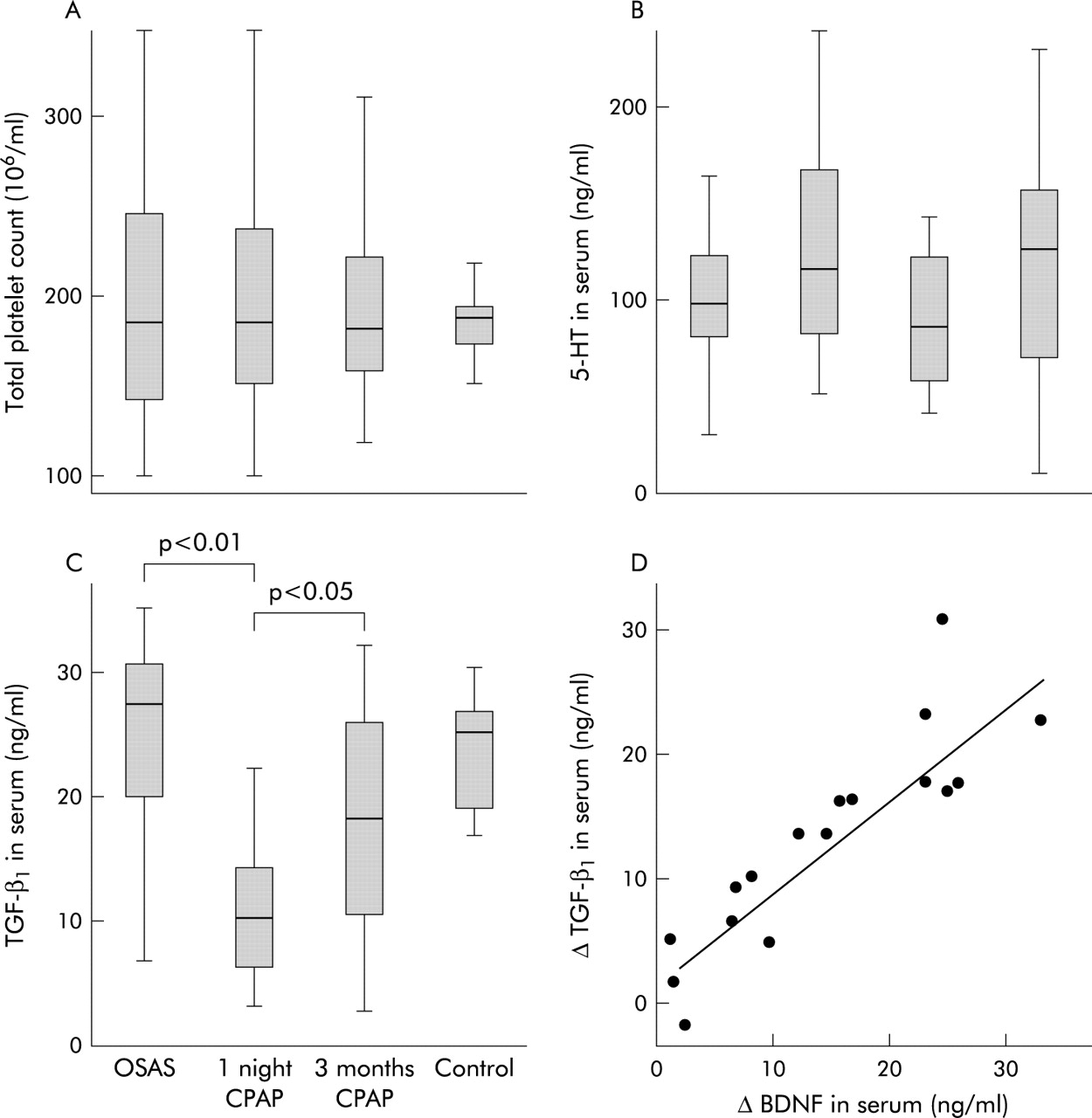
Despite the different range, median platelet counts were similar in controls and patients at all time points (fig 2A). To further elucidate the underlying mechanisms, the regulation of platelet markers was investigated. There was no significant difference in TGFβ1 and 5-HT levels in serum between controls and patients with untreated OSAS. In both controls and patients with untreated OSAS there was a correlation between serum BDNF and serum TGFβ1 levels (OSAS: r = 0.72, p<0.01; controls: r = 0.73, p<0.01), but no significant correlation between serum BDNF and 5-HT levels (OSAS: r = 0.08, p = 0.77; controls: r = −0.06, p = 0.86). One night of CPAP treatment led to a significant decrease in serum TGFβ1 levels but not in serum 5-HT levels (fig 2B and C). In addition, there was a strong correlation between the individual reduction in serum BDNF and TGFβ1 concentrations (r = 0.90, p<0.001) following the first night of treatment (fig 2D). In contrast, there was neither a change in TGFβ1 plasma levels following CPAP treatment nor a correlation between BDNF and TGFβ1 levels in plasma (data not shown).

Comparison with platelet markers. (A) Platelet counts, (B) serum 5-hydroxytryptamine (5-HT) concentrations, and (C) serum transforming growth factor-β1 (TGFβ1) concentrations in the same groups as detailed in fig 1. Box plot details are as described in fig 1. Significant differences between groups or time points are marked with p values (levels of significance). (D) Serum levels of BDNF or TGFβ1 after one night of CPAP treatment were subtracted from serum levels before CPAP treatment of each patient, giving the individual decrease in BDNF (ΔBDNF in serum) or TGFβ1 (ΔTGFβ1 in serum) after one night of CPAP treatment. Each point represents one patient; the line is the regression line calculated with SPSS.
Spontaneous BDNF release by mononuclear cells
In 15 of the 17 patients, cell culture experiments with monocyte enriched peripheral blood mononuclear cells were performed before and 3 months after initiation of CPAP treatment. Similar experiments were performed in control subjects (n = 12). There was no significant difference in the spontaneous release of BDNF between controls and untreated patients with OSAS (p = 0.91, fig 3). Despite a higher median level (138.9 pg BDNF/ml medium after treatment v 34.0 pg BDNF/ml medium before treatment), there was no significant difference in spontaneous BDNF release before and after 3 months of CPAP treatment (p = 0.31) in patients with OSAS (fig 3).

{kind=link}
{kind=link}
{kind=link}
Spontaneous release of BDNF by mononuclear cells. Monocyte enriched peripheral blood mononuclear cells were cultured for 48 hours and BDNF concentrations measured in cell free supernatants. The figure shows BDNF concentrations (pg/ml) in supernatants of patients with OSAS before CPAP treatment (OSAS), after 3 months of CPAP treatment (3 months CPAP, n = 15 patients), and controls (n = 12). Box plot details are as described in fig 1. p values are given for each comparison between groups or time points.
DISCUSSION
Despite normalisation of sleep parameters following successful treatment with CPAP, a large subpopulation of patients with OSAS continue to display cognitive deficits.6 The aetiology of this phenomenon is as yet unknown, and there is no specific treatment for this clinical condition.5 Our findings show that effective CPAP treatment impacts on circulating stores of BDNF, a key mediator of cognition in adults.
In patients with OSAS, 1 night of CPAP treatment resulted in a steep fall in previously normal serum BDNF concentrations. Due to relatively low BDNF levels in human plasma (<0.5 ng/ml), BDNF levels in human serum (10–30 ng/ml) serve as an estimate for the amount of BDNF stored in platelets.14 Platelets, which acquire BDNF from external sources and release BDNF following agonist stimulation, appear to be a unique BDNF transportation system in the human body.13 There is an abundant production of BDNF in peripheral tissues which is not completely attributable to a local function of BDNF in these tissues.25 It has therefore been postulated that peripheral BDNF is taken up by neurones of the central and peripheral nervous system.25 Circulating platelets may not only serve as a transportation system for BDNF, but also as a repository which can release large amounts of BDNF on acute demand in specific organs.13 Since platelet levels of BDNF are not influenced by age, weight or height,14 the amount of BDNF stored in platelets seems to be relatively stable. The median fall in serum BDNF concentrations to less than 25% of previous values after one night of CPAP treatment is therefore exceptional and has not been previously reported in other conditions.
Several lines of evidence point to a depletion of BDNF stores in platelets during the first night of CPAP treatment. Firstly, differences in BDNF serum concentrations were not attributable to a change in platelet numbers after starting CPAP treatment. Secondly, a suppression of BDNF production appears unlikely, since BDNF is neither synthesised by human platelets nor its precursors.13 Analysis of platelet markers provided further evidence for a specific BDNF depletion of platelets. In a previous study with healthy adults (68 men and 72 women, 20–60 years old) we found a stronger correlation of BDNF with the platelet α-granule marker TGFβ1 (r = 0.75, p<0.01) than with the platelet dense core granule marker 5-HT (r = 0.31, p<0.05).14 The analysis of men with untreated OSAS and control men in our present study supported these findings: there was a strong correlation of BDNF with TGFβ1 but not with 5-HT in serum. These data suggest that BDNF might be co-localised with TGFβ1 in platelet α-granules14 rather than with 5-HT in dense core granules.26 The parallel fall in TGFβ1 and BDNF serum concentrations following CPAP treatment is therefore compatible with a degranulation of platelet α-granules. This degranulation cannot be explained by an overall activation of platelets, since there is no evidence in the literature for an increase in platelet activity during the first night of CPAP treatment.27 Instead, the concomitant decrease in serum and plasma BDNF concentrations suggests that BDNF is specifically removed from peripheral blood. The hypothesis that enhanced consumption rather than decreased production of BDNF accounts for low circulating BDNF levels during CPAP treatment is further supported by our cell culture experiments which found no decrease in spontaneous BDNF release by peripheral blood mononuclear cells after CPAP treatment.
In conclusion, this study has shown that CPAP treatment is associated with a decrease in circulating BDNF concentrations but not a decrease in BDNF secretion. We hypothesise that this phenomenon reflects increased neuronal demand for BDNF during treatment, since neurones can acquire peripheral BDNF to change neuronal activity and synaptic transmission.28,29 Low circulating BDNF levels in this critical time period could therefore interfere with cognitive improvement. It might be speculated that circulating BDNF does not reflect baseline cognitive performance, but the ability to react to unusual demand. This would explain the finding that circulating BDNF levels did not differ between controls and untreated patients with OSAS (in spite of presumably different cognitive performances). Notably, there was no correlation between the improvement in sleep parameters and the decrease in BDNF levels following CPAP treatment. In light of the reported discrepancy between the improvement in sleep parameters and cognitive functions during CPAP treatment,6 these findings further support the hypothesis that BDNF might be specifically related to cognitive changes during treatment. Further studies are needed to elucidate whether low circulating BDNF levels or insufficient BDNF production relate to deficits in cognitive improvement during treatment with CPAP.
Acknowledgments
The authors thank Dr Christiana Zingler and Prof Dr Peter Schuff-Werner (Institute of Clinical Chemistry and Pathobiochemistry, University of Rostock) for providing HPLC and blood cell count measurements.
REFERENCES
Footnotes
-
This study was funded by the University of Rostock (Grant FORUN 989043).
-
The authors have no competing interests to declare.
Linked Articles
- Airwaves