Article Text

Abstract
Background: A study was undertaken to evaluate the efficacy of dexamethasone in patients mechanically ventilated for lower respiratory infection caused by respiratory syncytial virus (RSV-LRTI).
Methods: In a multicentre randomised controlled trial patients were randomised to receive either intravenous dexamethasone (0.15 mg/kg 6 hourly for 48 hours) or placebo. End points were the duration of mechanical ventilation, length of stay (LOS) in the pediatric intensive care unit (PICU) and in hospital, and the duration of supplemental oxygen administration.
Results: Thirty seven patients received dexamethasone and 45 received placebo. There was no significant difference in any of the end points between the two groups. In a post hoc analysis patients were stratified into those with mild gas exchange anomalies (Pao2/Fio2 >200 mm Hg and/or mean airway pressure ⩽ 10 cm H2O, bronchiolitis group) and those with severe gas exchange anomalies (Pao2/Fio2 ⩽200 mm Hg and mean airway pressure >10 cm H2O, pneumonia group). In the 39 patients with bronchiolitis the duration of mechanical ventilation was 4.3 days shorter in the dexamethasone group than in the placebo group (4.9 v 9.2 days, 95% CI −7.8 to −0.8, p=0.02) and the duration of supplemental oxygen was 3.6 days shorter (7.7 v 11.3 days, 95% CI −8.0 to −0.1, p=0.048). No differences in end points were found in the pneumonia group.
Conclusions: Dexamethasone had no beneficial effect in patients mechanically ventilated for RSV-LRTI but was found to have a beneficial effect in patients with bronchiolitis.
- children
- dexamethasone
- mechanical ventilation
- respiratory syncytial virus
Statistics from Altmetric.com
Respiratory syncytial virus (RSV) is the most common cause of lower respiratory tract infections in young children.1 Almost all children are infected at least once with RSV before the age of two. About 1% of the children with RSV lower respiratory tract infection (RSV-LRTI) need to be admitted to hospital.2 Respiratory failure progresses in 5–8% of them, necessitating mechanical ventilation.3–5
A substantial body of experimental and clinical evidence suggests that the immune response during RSV-LRTI may be deleterious for the host,6–8 suggesting that immune modulating drugs such as corticosteroids may be effective. This has been the subject of many trials, most of which found that corticosteroids were not beneficial in patients with mild RSV-LRTI.9 However, in a previous trial we found that corticosteroids might be beneficial in patients with severe RSV-LRTI. Oral prednisolone shortened both the duration of mechanical ventilation and the length of stay (LOS) in hospital in a small subgroup of patients who needed mechanical ventilation.10 To evaluate the role of corticosteroids in this patient group further we performed a multicentre, prospective, double blind, randomised, placebo controlled trial to determine the efficacy of intravenous dexamethasone in patients mechanically ventilated for RSV-LRTI.
METHODS
Study design
The study was conducted in five pediatric intensive care units (PICU) in the Netherlands. All patients younger than 24 months on mechanical ventilation for RSV-LRTI were eligible for enrolment. The presence of RSV infection was confirmed by direct immunofluorescence assay (Imagen, Dako, Denmark) of a nasopharyngeal aspirate during the first 24 hours after hospital admission. The decision to start mechanical ventilation was taken in the referring hospital or by the attending intensive care physician. Patients were only included after parents gave their written informed consent. Those who had used systemic or inhaled corticosteroids within the 2 months before admission were excluded. The medical ethical review board of each participating centre approved the study.
Patients were ventilated with a Servo 300A (Siemens, Munich, Germany), or an Evita 4 (Dräger, Lübeck, Germany) ventilator. Ventilation setting management, weaning policy, and the decision to stop ventilation were left to the attending PICU team according to local policies. Ventilation strategies and sedation protocols did not differ widely in the participating PICUs. Clinical decisions were made by each patient’s physicians independent of the study protocol. In order to minimise the potential bias caused by differences in patient management in the different centres, randomisation was stratified for each participating centre. Patients were allocated to dexamethasone or placebo by computerised block randomisation in groups of 10, centrally performed by an independent pharmacist. Each participating centre received a randomisation list and the trial medication preparation protocol. The trial medication was prepared in advance in the pharmacy where the concealed randomisation list was kept until the study was completed. Each enrolled patient received the trial medication with the next number in sequence. The trial medication was intravenous dexamethasone (0.15 mg/kg 6 hourly for 48 hours) or placebo and had to be started within 24 hours after the start of mechanical ventilation.
End points for the efficacy analysis were the duration of mechanical ventilation, LOS in the PICU and in the hospital, and duration of supplemental oxygen.
The mean blood pressure and glucosuria tests were recorded daily on the first 5 days of admission. To monitor the duration of viral shedding, RSV immunofluorescence assay of nasopharyngeal aspirate was repeated on days 2, 3, 7, 10 and 14 while the patient was an inpatient. If two consecutive assays were negative the viral shedding was considered to be negative.
Statistical analysis
The previously found difference of 1.5 days in mechanical ventilation was considered to be clinically relevant; in order for this difference to be detected, 60 patients (30 in each arm) would be needed (α=0.05, β=80%).
Statistical analysis was performed with SPSS for Windows, version 10.1 (SPSS Inc). The Student’s t test was used to compare group means for normally distributed data; otherwise the Mann-Whitney U test was applied. Proportions were compared by the χ2 test. A two sided p value of <0.05 was considered statistically significant. Data were analysed according to the intention to treat principle. Data in the tables are given as mean (SE) unless otherwise stated.
RESULTS
Eligible patients
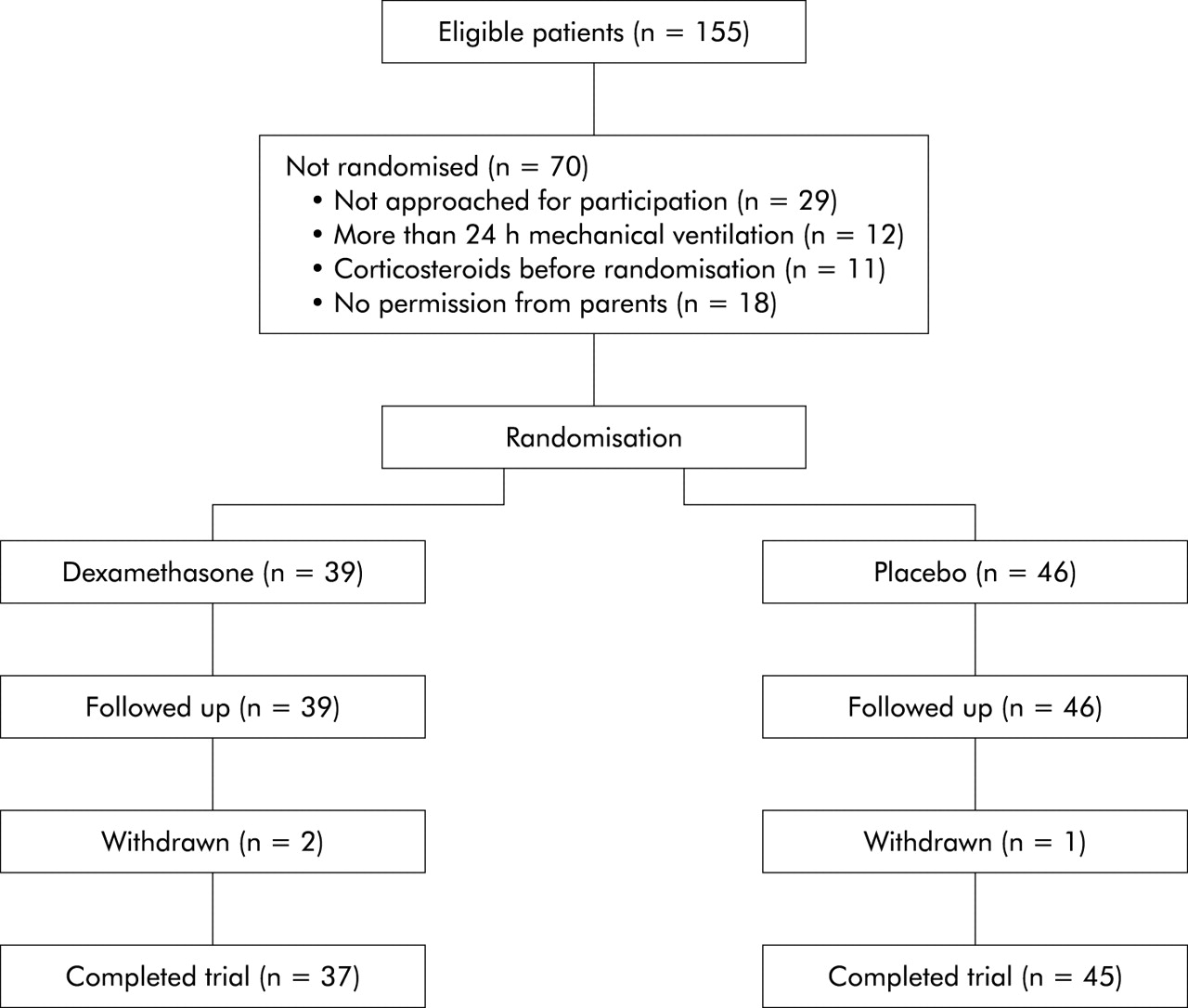
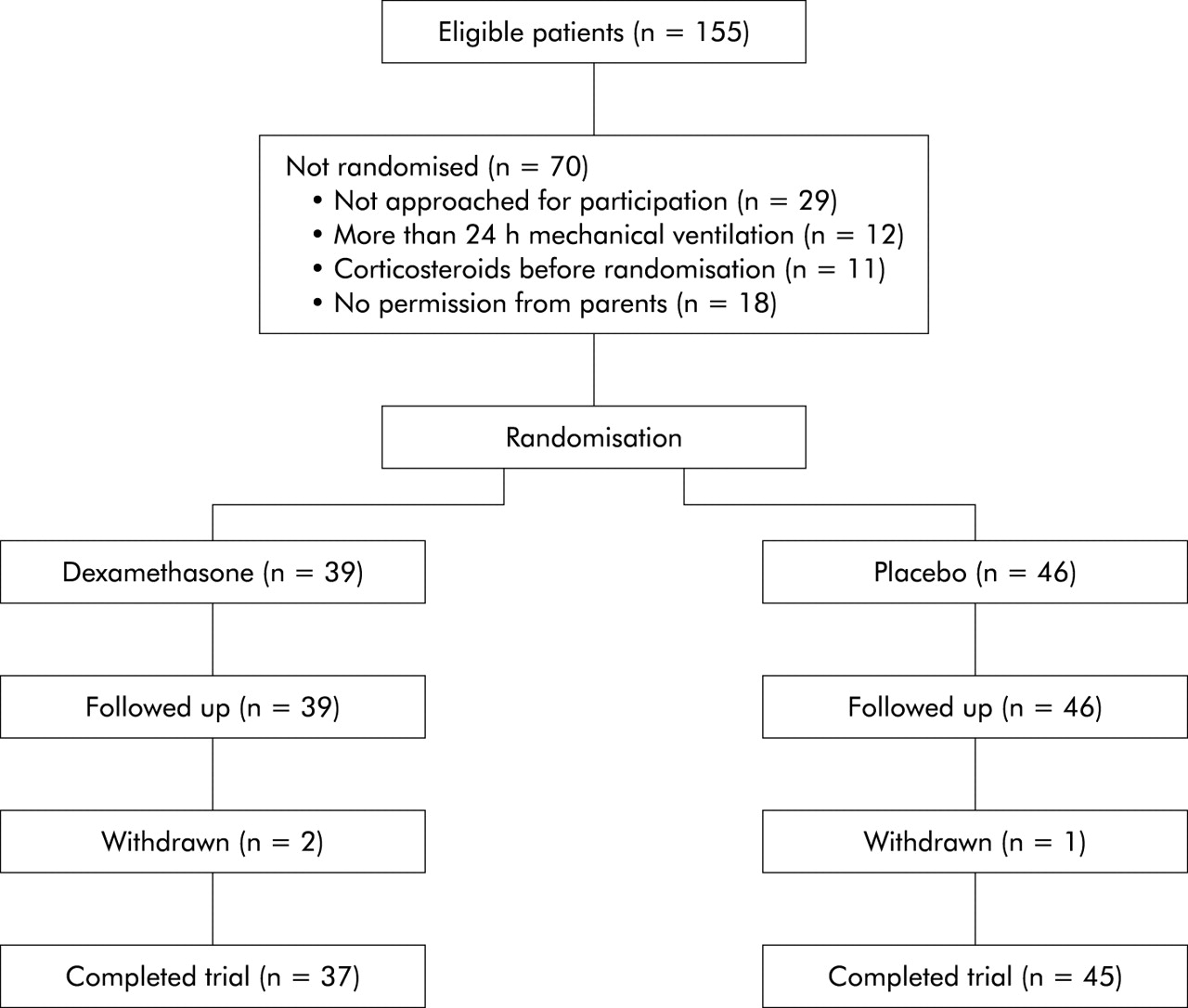
From December 1997 to March 2001 155 patients met the inclusion criteria and were eligible for enrolment. Seventy patients were not randomised for reasons shown in fig 1. Of the 85 patients who were enrolled, 39 were randomised to receive dexamethasone and 46 to receive placebo. After enrolment three patients were withdrawn, one (dexamethasone group) because she died 4 days after admission due to severe cerebral oedema in combination with refractory seizures existing already before inclusion, and two because their medication vials (one containing dexamethasone and the other placebo) were accidentally interchanged. Eighty two patients therefore completed the trial, 37 of whom received dexamethasone and 45 placebo.
{kind=link}
Enrolment of patients to trial.
Baseline characteristics
The baseline characteristics of the study participants are shown in table 1. The proportion of males was higher in the dexamethasone group than in the placebo group and the dexamethasone group was significantly younger than the placebo group. There were no other differences in baseline characteristics between the two treatment groups.
Characteristics of patients on admission in the PICU according to treatment group
Outcome
The mean duration of mechanical ventilation in the dexamethasone group was 1.6 days shorter than in the placebo group; this difference was not statistically significant (table 2). There was no difference in either the mean LOS in the PICU and in the hospital or the mean duration of supplemental oxygen between the two treatment groups. The results were not different after correction for sex or age (data not shown). Five patients (two in the dexamethasone group and three in the placebo group) needed to be re-intubated because of upper airway obstruction following intubation.
Mean (SE) duration of mechanical ventilation, length of stay (LOS) in the paediatric intensive care unit (PICU) and hospital, and duration of supplemental oxygen in the two treatment groups
During the course of the trial Tasker et al published a study in which they reported that mechanically ventilated patients with RSV-LRTI may present with two patterns of disease which can be distinguished on the basis of early respiratory parameters.5 In order to determine whether the effect of dexamethasone was dependent on these clinical patterns we performed a post hoc subgroup analysis. Patients were stratified according to the Pao2/Fio2 ratio and the mean airway pressure (MAP) on the day of admission, analogous to the criteria described by Tasker et al.5 Arterial blood gas analysis data were available for 80 patients during the first 24 hours of admission (in case more blood gas analyses were available the worst Pao2/Fio2 was chosen). These patients were stratified into a bronchiolitis group (mild gas exchange anomalies: Pao2/Fio2 >200 mm Hg and/or MAP⩽10 cm H2O, n=39) and a pneumonia group (severe gas exchange anomalies: Pao2/Fio2 ⩽200 mm Hg and MAP >10 cm H2O, n=41). There were no differences in baseline characteristics between the dexamethasone and placebo treated patients within the bronchiolitis and pneumonia groups. The results of the end point analyses in these subgroups are shown in table 3. In the bronchiolitis group the mean duration of mechanical ventilation in the patients who received dexamethasone was 4.3 days shorter than in those who received placebo (4.9 v 9.2 days, 95% CI −7.8 to −0.8 days, p=0.02). The mean LOS in the PICU was 2.4 days shorter in the dexamethasone group than in the placebo group but this difference was not statistically significant (7.9 v 10.3 days, 95% CI −6.8 to 2.0, p=0.28). However, in the mild group three patients (two of whom received dexamethasone and one placebo) needed to be re-intubated because of upper airway obstruction following intubation. If these three patients were excluded from the analysis there was a significant difference of 3.9 days in mean LOS in the PICU (6.6 v 10.5 days, 95% CI −7.6 to −0.2, p=0.039) The mean LOS in hospital and the mean duration of supplemental oxygen were also shorter in the dexamethasone group than in the placebo group, but only the difference in duration of supplemental oxygen reached statistical significance. In the pneumonia group there was no significant difference in any of the end points between the dexamethasone and placebo treated patients.
Mean (SE) duration of mechanical ventilation, length of stay (LOS) in the paediatric intensive care unit (PICU) and hospital, and supplemental oxygen in days in the two treatment groups according to subgroup analysis*
Concomitant treatment
There were no differences in concomitant treatment with antibiotics, bronchodilators or paralysing agents between the two treatment groups (table 4). None of the patients received palivizumab before admission or ribavirin during admission. Three patients received corticosteroids after randomisation; two (one from each treatment group) were started after 8 days with the aim of getting them off the ventilator earlier and one in the dexamethasone group was started on corticosteroids after 2 days because of suspicion of adrenal insufficiency.
Concomitant treatment according to treatment group
Side effects
Mean blood pressure both before the start of trial medication (59 v 58 mm Hg in the dexamethasone and placebo group, respectively, p=0.72) and during the first 5 days of admission (42 mm Hg in both groups, p=0.36) did not differ between the two treatment groups. In one patient (dexamethasone group) malignant hypertension developed 3 days after start of the trial medication which later proved to be caused by a renal vein thrombosis. During the first 5 days of admission glucosuria was found on 7 of the 146 days when urine was checked in the dexamethasone group and on 5 of the 163 days when urine was checked in the placebo group (p=0.56).
During the first 2 weeks of admission at least two RSV immunofluorescence assays were repeated in 58 patients (23 in the dexamethasone group and 35 in the placebo group). In six patients in the dexamethasone group and in nine in the placebo group the test became negative (p=0.60).
DISCUSSION
The results of this trial show that dexamethasone does not lead to a shorter duration of mechanical ventilation in patients with RSV-LRTI. Although dexamethasone shortened the duration of mechanical ventilation by more than 1 day in the whole study cohort, this difference did not reach statistical significance. Our results confirm a very recently published trial that also evaluated the efficacy of dexamethasone in mechanically ventilated patients with RSV-LRTI. However, this trial was primarily designed to evaluate differences in virus quantity and the authors stated that it was underpowered to detect differences of <50% between the two groups.11
RSV induced respiratory insufficiency may present with two different patterns. The first pattern, classically referred to as bronchiolitis, is characterised predominantly by obstruction of the airways while the second pattern, classically referred to as pneumonia, is characterised by a predominantly restrictive parenchymal lung disease with alveolar consolidation on the chest radiograph and has many features in common with acute respiratory distress syndrome (ARDS).12 Tasker et al have shown that it is possible to identify the group with four quadrant alveolar consolidation on the chest radiograph (compatible with RSV pneumonia) by using the alveolar arterial oxygen gradient (AaDo2) and MAP during the first 24 hours of admission to the PICU. They found that AaDo2 of ⩾400 mm Hg and MAP of >10 cm H2O had a very high positive and negative predictive value for a four quadrant alveolar consolidation. In addition, they found that the LOS of this group in the PICU is much longer than for those with mild gas exchange anomalies on admission and suggested that trials evaluating treatment of mechanically ventilated patients with RSV-LRTI should stratify for these two disease patterns.5 By combining the results of lung function studies in patients with RSV-LRTI with the results of the study by Tasker et al, Newth concluded that patients with mild gas anomalies may reflect a mainly obstructive pulmonary function pattern (i.e. bronchiolitis) while severe gas exchange anomalies are consistent with a severe restrictive pulmonary function pattern (i.e. pneumonia).12–14 In addition, Newth showed that the AaDo2 value of ⩾400 mm Hg that was used corresponds to a Pao2/Fio2 ratio of approximately ⩽200 mm Hg which is used to define ARDS.13,15 By applying a cut off value of 200 mm Hg for the Pao2/Fio2 ratio and of 10 cm H2O for the MAP to differentiate between patients with RSV bronchiolitis and those with pneumonia (who did not fulfil both criteria), we found a marked difference in the efficacy of dexamethasone between these subgroups. Dexamethasone reduced mechanical ventilation by more than 4 days and LOS in the PICU by more than 2 days in the bronchiolitis group. In addition, the LOS in hospital and the duration of supplemental oxygen were reduced by dexamethasone, only the latter end point being statistically significant.
For several reasons our results should be interpreted with caution. Firstly, the efficacy of dexamethasone in patients with RSV bronchiolitis was demonstrated by a post hoc analysis. This only generates the hypothesis that corticosteroids may be beneficial in patients with bronchiolitis and needs to be confirmed in a prospectively conducted randomised trial. Secondly, Tasker et al found an important difference in LOS in the PICU between patients with mild gas exchange anomalies and those with severe gas exchange anomalies. By applying their criteria we would have expected to find a similar difference between these two subgroups in the placebo treated patients but this was not the case, which underscores the need for further studies on this topic.
The efficacy of corticosteroids in patients with RSV-LRTI has been studied for decades with conflicting results.10,16–29 Although some found a beneficial effect,10,16–19,21,22 most well designed randomised controlled trials did not show that corticosteroids were beneficial.23–29 Like other workers, in an earlier trial we were unable to show that oral prednisolone was beneficial in patients with mild RSV-LRTI.10 However, prednisolone shortened the duration of mechanical ventilation and the LOS in hospital in a small group of patients on mechanical ventilation. The results reported here support our previous findings that corticosteroids are beneficial in a subgroup of patients with RSV bronchiolitis. Further research is needed to identify more precisely patients in the PICU with RSV-LRTI in whom corticosteroids are potentially beneficial.
Since no treatment is available for RSV-LRTI, our findings may indicate a step forward in the search for effective treatment. This may have an important socioeconomic impact since hospital admissions for bronchiolitis have increased substantially over the last decade and it is estimated that, in the USA, more than 120 000 children are admitted annually with RSV-LRTI.30
In our previous trial we used oral prednisolone in a dose of 1 mg/kg/day for 7 days. Because the beneficial effect of prednisolone was mainly seen in the first 3 days, in the current trial a shorter and higher dose of intravenous corticosteroids was used. On the basis of the dose used in patients with laryngitis subglottica and meningitis,31,32 the dose of dexamethasone chosen was 0.6 mg/kg/day (equivalent to 6 mg/kg/day prednisolone). The parenteral route was chosen because mechanically ventilated patients were studied.
The beneficial effects of intravenous dexamethasone should outweigh the potential side effects. No significant side effects were found in the present study, which is in accordance with what is known about short courses of steroid treatment.33
In conclusion, dexamethasone was not found to be beneficial in patients needing mechanical ventilation for RSV-LRTI. However, post hoc subgroup analysis suggested a beneficial effect of dexamethasone in a subgroup of patients with RSV bronchiolitis. Although our findings indicate a significant improvement in the therapeutic possibilities for patients with RSV bronchiolitis who need mechanical ventilation, this observation can only be considered hypothetical and should be tested in a prospective randomised controlled trial.
Acknowledgments
We thank the trial pharmacists and medical staff and nurses of all participating centres for their help with preparing the trial medication and including patients and completing the trial respectively, and the Department of Clinical Epidemiology and Biostatistics, Academic Medical Center, Amsterdam for their statistical advice and support.
REFERENCES
Linked Articles
- Airwaves