Article Text

Abstract
Background: Exhaled nitric oxide (FENO) is raised in asthmatic children, but there are inconsistencies in the relationship between FENO and characteristics of asthma, including atopy, increased airway responsiveness (AR), and airway inflammation. The aim of this study was to investigate the relationship between FENO and asthma, atopy, and increased AR in children.
Methods: One hundred and fifty five children (79 boys) of mean age 11.5 years underwent an assessment that included FENO measurements, spirometric tests, inhaled histamine challenge, and a skin prick test. Blood was collected for eosinophil count. Current and past asthma like symptoms were determined by questionnaire.
Results: In multiple linear regression analyses FENO was associated with atopy (p<0.001), level of AR (p = 0.005), blood eosinophil count (p = 0.007), and height (p = 0.002) but not with physician diagnosed asthma (p = 0.1) or reported wheeze in the last 12 months (p = 0.5). Separate regression models were conducted for atopic and non-atopic children and associations between FENO and AR, blood eosinophils and height were only evident in atopic children. Exhaled NO was raised in children with a combination of atopy and increased AR independent of symptoms.
Conclusion: Raised FENO seems to be associated with an underlying mechanism linking atopy and AR but not necessarily respiratory symptoms.
- exhaled nitric oxide
- asthma
- atopy
- bronchial hyperreactivity
- children
Statistics from Altmetric.com
There is considerable interest in the measurement of fractional exhaled nitric oxide (FENO), particularly with regard to its potential role in both the diagnosis and management of asthma.1 Levels are raised in asthmatic children2 and adults,3 increase during asthma exacerbations,4 and are reduced after corticosteroid treatment.4 Exhaled NO is thought to reflect airway inflammation in asthma but only limited data are available regarding the relationship between FENO and any direct evaluation of inflammation such as airway biopsy.5,6 On the other hand, numerous studies have investigated the relationships between FENO and indirect indicators of airway inflammation. For example, FENO is positively correlated with eosinophils in sputum7 and lavage fluid.8 Furthermore, some studies have reported an association between FENO and airway responsiveness (AR),9,10 but the data regarding the associations between FENO and both eosinophilia5,6 and AR9–12 are inconsistent.
We have previously described associations between atopy and FENO in infants13 and children14 that are independent of symptoms of asthma. Since our original observations, the importance of taking account of atopy when interpreting FENO measurements has become apparent. Exhaled NO levels are raised in atopic but not in non-atopic asthmatics,11,15 and our observation that FENO is raised in healthy atopic children has been confirmed in adults.16 We believe that inconsistencies in the literature with regard to FENO and indirect markers of inflammation have resulted in part from a failure to fully account for atopy. We therefore hypothesised that atopy modifies the relationships between FENO and important characteristics of asthma (such as AR, eosinophilia, and symptoms). If this is the case, there are important implications with regard to the use of FENO as a diagnostic tool in asthma.
To investigate the association between atopy and FENO in more detail we included FENO measurements in the 11 year follow up of a well characterised birth cohort. This cohort had longitudinal symptom questionnaire data and measurements of lung function, AR, and atopy that allowed accurate phenotypic descriptions with regard to important asthma related characteristics.
METHODS
Subjects and protocol
Subjects were participants in a prospective birth cohort study of lung function, AR, and atopy that included data from probands and all family members enrolled from an unselected population.17 The probands had previously been assessed at 4 weeks, 6 months, 12 months, and 6 years of age. Data for the present study were gathered from the 11 year follow up study. Family members were studied in the first year and at the 6 and 11 year follow up surveys. In the present study 191 of the original cohort of 253 infants and 165 siblings were assessed. All children underwent an assessment that included spirometric tests, inhaled histamine challenge, skin prick testing, and blood eosinophil count. Current and past respiratory symptoms were assessed using a modified ATS questionnaire.18 Assessments took place either at the hospital or the child’s home. Exhaled NO was measured only in those attending hospital (n = 155, 97 of the original cohort; 58 siblings) and the results from these children are presented in this study. None of the children were symptomatic at the time of the study.
The study was approved by the medical ethics committee of Princess Margaret Hospital for Children. Informed consent was obtained from parents.
Exhaled nitric oxide
Exhaled NO was measured using a fast response chemiluminescence analyser (NOA 280, Sievers Instruments Inc, Boulder, CO, USA) as previously described.14 Measurements were taken before spirometry and histamine challenge. Children maintained an expiratory flow of 35 ml/s and mouth pressure of 15 cm H2O.
Pulmonary function and airway responsiveness
Pulmonary function testing was performed using a hand held spirometer (Pneumocheck Spirometer 6100; Welch-Allyn, Skaneateles Falls, NY, USA) in accordance with published guidelines.19 Airway responsiveness to histamine was determined using the rapid dosimeter technique.20 Responsiveness was expressed as the dose of histamine (µM) that provoked at least a 20% fall in FEV1 (PD20) and increased AR was defined as PD20 <7.8 µM histamine.21 A dose response slope (DRS) was also calculated using the method of O’Connor et al.22
Skin prick testing and eosinophil count
Skin reactivity to cow’s milk, egg white, rye grass, mixed grass, Dermatophagoides farinae, Dermatophagoides pteronyssinus, cat dander, dog dander, Alternaria alternans and Aspergillus fumigatus (Hollister-Stier, Elkhart, IN, USA) was assessed by skin prick tests as described by Pepys.23 The positive control was histamine sulphate (10 mg/ml) and the negative control was 0.9% saline. A positive skin prick test was defined as a weal at least 3 mm in its longest dimension. Atopy was defined as the presence of at least one positive skin prick test.
Blood was collected and the eosinophil count was measured using a flow cytometer (Coulter Maxm, Beckman-Coulter Inc). Values are expressed as absolute cell counts.
Statistical analyses
Exhaled NO, DRS, and blood eosinophil values were skewed and were log10 transformed before analysis (a constant of 1 was added to DRS values) to achieve a near normal distribution. Associations between log(FENO) and reported physician diagnosed asthma, wheeze in the last 12 months (recent wheeze), current asthma (wheeze in the last 12 months plus increased AR),21 atopy, log(DRS), log(blood eosinophils), height, age, and spirometric variables were assessed in univariate analyses using Student’s t tests and simple linear regression. Multiple linear regression analyses were undertaken using transformed FENO values as the outcome variable which was computed by taking the antilog of the estimate of increase (or difference) in transformed FENO to give the fold increase per unit change in a continuous explanatory variable or fold difference between levels of a binary explanatory variable. Only factors that had a significance level of at least p⩽0.1 from univariate analyses were included in the model. These were age, height, log(eosinophil count), log(DRS), and atopy. Symptoms were included in the model separately as either reported physician diagnosed asthma or recent wheeze. Interactions between atopy and all other factors were investigated and separate regression models were constructed for both atopic and non-atopic children. Variables in all models were excluded in a stepwise fashion if they did not reach significance at the 5% level. Exhaled NO levels are reported as geometric means (GM) with 95% confidence intervals (CI). All analyses were performed using SPSS version 9.0 (SPSS, Chicago, IL, USA).
RESULTS
Exhaled NO concentrations were measured in 155 subjects (79 boys) of mean (SD) age 11.5 (2.3) years (range 6–18). There was no significant difference with regard to age, sex, height, atopic status, AR, FEV1, eosinophil count, physician diagnosed asthma, reported recent wheeze, and use of inhaled steroids between these children and those in whom FENO measurements were not made (n = 201).
Five children treated with regular inhaled corticosteroids (ICS) were excluded from analyses because of the known effects of ICS on FENO. Of the remaining 150 children, spirometric tests were performed in all individuals, skin prick testing in 149 (99%), bronchial challenge in 144 (96%), and eosinophil counts in 136 (91%). Eighty three children (56%) were atopic, 54 (38%) had increased AR, 34 (23%) reported wheeze in the past 12 months, and 26 (17%) had physician diagnosed asthma.
In univariate analyses, FENO was higher in children who had reported physician diagnosed asthma (16.4 ppb, 95% CI 11.0 to 24.6) than in non-asthmatic children (11.0 ppb, 95% CI 9.4 to 12.9; p<0.03), in those with reported recent wheeze (16.6 ppb, 95% CI 11.9 to 23.2) than in those without recent wheeze (10.8 ppb, 95% CI 9.2 to 12.7; p = 0.01), and in those with current asthma (24.5 ppb, 95% CI 15.0 to 40.0) than in those without current asthma (11.0 ppb, 95% CI 9.5 to 12.8; p<0.001). Atopic children (17.9 ppb, 95% CI 14.9 to 21.4) had significantly higher FENO levels than non-atopic children (7.2 ppb, 95% CI 6.0 to 8.7; p<0.001) and there was a positive correlation between the number of skin prick reactions and FENO (Pearson’s correlation coefficient r = 0.61, p<0.001). There was a positive association between FENO and DRS (r2 = 0.21, p<0.001), eosinophil count (r2 = 0.11, p<0.001), and height (r2 = 0.05, p<0.008). There were no associations between FENO and measurements of pulmonary function when adjusted for height. The relationship between FENO and DRS in atopic and non-atopic children is shown in fig 1.

Relationship between FENO and airway responsiveness (DRS) in atopic (○) and non-atopic (•) children. Separate regression lines for atopic and non-atopic children are included. Only in atopic children is there a significant relationship between FENO and DRS (r2 = 0.301, p<0.001).
In the multiple regression model atopy (p<0.001), DRS (p = 0.003), eosinophil count (p = 0.003), and height (p = 0.002) were all significantly associated with FENO (table 1). Neither physician diagnosed asthma (p = 0.1) nor recent wheeze (p = 0.5) were associated with FENO in this model. There was a significant interaction between atopy and DRS (p = 0.001) and a trend for an interaction between atopy and eosinophil count (p = 0.06). In order to examine these interactions further, separate regression models were constructed for atopic and non-atopic children. In these models DRS, eosinophils, and height were associated with FENO in atopic (table 2) but not in non-atopic children (table 3). Again, neither physician diagnosed asthma nor recent wheeze were associated with FENO in either of these models.
Fold difference in fractional exhaled nitric oxide (FENO) in children with symptoms compared with children without symptoms, and fold increase per unit change in log(eosinophils), log(DRS), and height in study population (n = 150)
Fold difference in fractional exhaled nitric oxide (FENO) in children with symptoms compared with children without symptoms, and fold increase per unit change in log(eosinophils), log(DRS), and height in atopic children (n = 80)
Fold difference in fractional exhaled nitric oxide (FENO) in children with symptoms compared with children without symptoms, and fold increase per unit change in log(eosinophils), log(DRS), and height in non-atopic children (n = 70)
As there were a number of sibling pairs in this cohort, there may be genetic linkage within the group. The children from the original cohort (n = 97) were therefore analysed separately and the observed associations persisted.
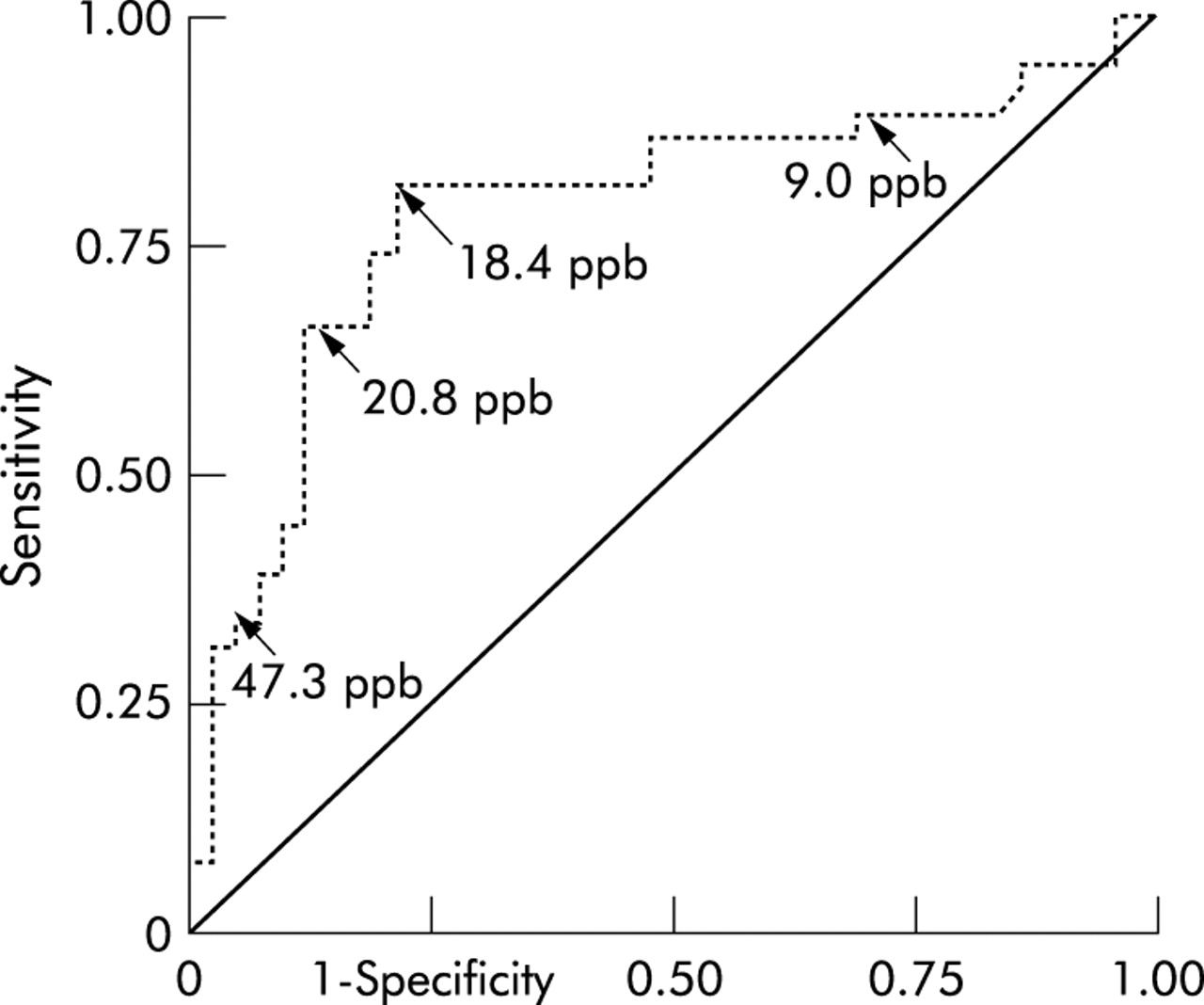
Receiver operator characteristics curve
As FENO was found to be associated with AR only in atopic children and was independent of symptoms, we hypothesised that FENO may provide a simple test to identify atopic children with increased AR. This was investigated by generating a receiver operator characteristic (ROC) curve to determine the specificity and sensitivity of FENO for predicting increased AR in atopic children (fig 2). For this analysis, increased AR was defined as PD20 <7.8 µM.21 A level of 18.4 ppb was identified as giving the best combination of sensitivity and specificity (81.1% and 78.6%). The likelihood ratio for an atopic child in our population having FENO of <18.4 ppb and increased AR is only 0.23. Height, which was associated with FENO in this study, contributed to the variability of the sensitivity and specificity such that individuals below the average height tend to reduce the sensitivity and individuals with above average height tend to reduce the specificity.
{kind=link}
{kind=link}
ROC curve indicating the sensitivity and specificity for predicting increased AR in atopic children. Sensitivity and specificity were 81.1% and 78.6%, respectively, for an FENO level of 18.4 ppb.
DISCUSSION
This study has shown that atopy modifies the associations between FENO and both AR and blood eosinophil counts. An important finding is that FENO is raised in children with a combination of both atopy and increased AR, and this was independent of symptoms. Interestingly, FENO was not raised in subjects with only atopy or increased AR. These data suggest that raised FENO levels are the result of a mechanism(s) linking increased AR and atopy and extend the recently published observations of Steerenberg et al.24
We have previously reported an association between raised FENO and positive skin prick reactions in healthy children.14 The association between increased FENO and atopy in healthy subjects has been confirmed in other studies,16 but it is not a universal finding.25 Similarly, the data regarding the association between FENO and AR have been inconclusive.9–12 The results of this study extend our earlier observations and help to explain some inconsistencies in reported data. Our observations also explain the consistent reports of raised FENO levels in atopic compared with non-atopic asthmatics.11,15
A major finding from both our study and a recent study by Steerenberg et al24 is that the relationship between FENO and AR is only evident in atopic children. Ludviksdottir and colleagues15 reported a similar relationship in asthmatic adults. There is a well established relationship between atopy and increased AR in both children26,27 and adults,27 and our data suggest that increased NO production in the airways may be associated with a mechanism linking these two factors. This may involve inflammatory processes and would support the hypothesis that FENO is a marker of allergic airway inflammation. Peat et al28 suggested that IgE mediated inflammatory reactions in the airways of atopic children could lead to increased AR. We found that there was a relationship between FENO and blood eosinophils which was also dependent on the presence of atopy. This relationship has also been reported in an unselected population of children,24 as well as in a group of asthmatic children.29 In our study there was a positive correlation between peripheral eosinophils and DRS in the atopic but not the non-atopic children (data not shown). Blood eosinophils, however, do not necessarily reflect inflammatory processes in the lungs,30 and an alternative explanation is that increased FENO in this phenotype may be due to genetic variations in NO synthase (NOS) genes. In patients with asthma31 and cystic fibrosis,32 variations in FENO are associated with a polymorphism in the NOS1 gene. The NOS1 isoform has been shown to be important in the regulation of AR in animal models.33 Further investigations are required to determine the contribution of the various NOS isoform(s) to NO production in the airways of children with atopy and increased AR.
Interestingly, we found that the association between FENO and atopy and increased AR was independent of symptoms. This was a representative population sample of asthmatic children, although children with more severe asthma (those taking ICS) were excluded because of the known effects of ICS on FENO. Our findings are in agreement with those of Leuppi et al34 who found significantly raised FENO levels in atopic children with increased AR, regardless of symptoms. These authors suggested that FENO may be more closely associated with increased AR than symptoms. In contrast, Henriksen et al10 found that suspected asthmatic adolescents with both atopy and increased AR had higher FENO levels than healthy subjects with a similar phenotype. Similarly, Steerenberg et al24 found that FENO was associated with respiratory symptoms in atopic children, but it appears that these authors might not have controlled for AR when investigating the association between FENO and symptoms. Our results, if confirmed in future studies, suggest that raised FENO levels in children are associated with a common asthma phenotype (that is, atopy and increased AR) but not with asthma per se.
Our observation that FENO is raised in healthy children with both atopy and increased AR raises an intriguing possibility that NO might be protective in these children who are at risk of asthma but who have not developed symptoms. Indeed, there have been suggestions that NO may have a bronchoprotective role through its actions on smooth muscle relaxation and inhibition of smooth muscle proliferation.35 Alternatively, raised FENO may identify children who have latent asthma and are at risk of developing symptoms. Both atopy and increased AR in childhood have been reported as risk factors for the subsequent development of asthma in early adulthood.36 However, atopy and increased AR can coexist in adults in the absence of symptoms.27 The association between raised FENO levels and the development of asthma later in life can only be addressed by longitudinal data. This cohort will be reassessed 5 years after the present data were obtained.
There has been considerable interest in FENO as a diagnostic tool for asthma. A number of studies have reported good sensitivity and specificity of raised FENO for discriminating between asthmatics and non-asthmatics.37–39 In each of these studies the asthmatic patients had increased AR or significant airways reversibility while the non-asthmatics all responded normally. No study has investigated the diagnostic value of FENO in an unselected population. On the basis of our results we propose that low levels of FENO may be useful to exclude increased AR in atopic children with symptoms and, therefore, to help to exclude a diagnosis of asthma. Increased AR is almost ubiquitous in clinically obvious asthma and most asthmatic children are atopic.21 Tests of AR are not feasible in most clinical situations, particularly in children. Our data suggest that atopic children with respiratory symptoms but low FENO levels are unlikely to have increased AR. Indeed, in our study, if FENO levels are less than 18.4 ppb, the likelihood ratio for atopic children to have increased AR is only 0.23. We suggest that the diagnostic value of low FENO levels could be further tested in a prospective study.
We have used an expiratory flow rate of 35 ml/s for measuring FENO. The study was started before publication of recommendations for the measurement of FENO in children.40 However, the marginally lower expiratory flow rate than that suggested in these guidelines used in our study is unlikely to affect our findings since Kissoon et al41 have reported that flow rates between 30 and 50 ml/s are appropriate for children. Indeed, the use of a low flow rate may have increased our ability to measure differences in FENO between groups. Deykin et al38 showed in adults using higher flow rates that the discriminatory power of FENO for differentiating between asthmatic and non-asthmatic subjects was not affected by expiratory flow rates ranging from 47 ml/s to 500 ml/s.
In summary, we have shown that atopy is important in the relationship between FENO and AR. In this study, FENO was associated with increased AR only in atopic children. Furthermore, there was an association between FENO and blood eosinophils that was also only evident in atopic children. This supports the concept that FENO reflects allergic airway inflammation and this may be one of the mechanisms explaining the relationship between atopy and AR. Alternatively, raised FENO levels in children with both atopy and increased AR may be due to variations in NOS genes. This needs to be explored further. Raised FENO levels in non-asthmatic atopic children with increased AR may either be predictive for the development of asthma or may indicate a protective role of NO against the development of symptoms. These issues will be addressed in the next follow up study of this population of children. After controlling for both atopy and increased AR, we were unable to show an association between FENO and asthma or asthma like symptoms. This suggests that raised FENO levels in children are associated with a common asthma phenotype but not with asthma per se. These results have implications for the use of FENO as a diagnostic tool for asthma. However, we have proposed a role for FENO in atopic children with symptoms of unknown aetiology to exclude increased AR and, by inference, to help to exclude asthma.
Acknowledgments
The authors would like to express their gratitude to study members and their parents for participating in this project.
REFERENCES
Footnotes
-
Dr Turner was supported by the NH&MRC. Dr Franklin and Dr Stick are supported by the NH&MRC.
Linked Articles
- airwaves