Article Text

Statistics from Altmetric.com
Peak expiratory flow (PEF) monitoring is recommended in the management of moderate to severe asthma,1 and PEF outcome variables are used in many clinical trials. However, adherence with PEF monitoring is poor, and this is often attributed to the burden of measurement and recording. This analysis examined whether adherence with symptom monitoring was impaired by asking patients also to record PEF measurements.
Data were obtained from a randomised double blind study of breathing techniques in adults with poorly controlled asthma. Full details of the clinical trial are reported elsewhere.2 Subjects were non-smokers aged 19–80 years, using reliever as-needed ⩾4 times/week and taking inhaled corticosteroids ⩾200 μg/day. Figure 1 shows the study design, with between-visit intervals of 2 or 6 weeks. Throughout the study, 57 subjects used electronic diary spirometers (AM2, Erich Jaeger GmbH, Hoechberg, Germany) twice daily to answer questions about symptom frequency/intensity and treatment. There were three “PEF periods” during which subjects also measured spirometry twice daily. PEF was displayed after each of three manoeuvres followed by the highest PEF. At study visits, data were uploaded and reviewed by the research assistant but physician feedback was not provided. Subjects with poor adherence were not withdrawn. Weekly adherence was calculated as [(number of monitoring sessions completed)/(expected number sessions)*100] using a maximum of two sessions/day to exclude data “dumping”.3 Mixed model analysis (SAS 9.1) was used to examine the effect on adherence of PEF monitoring, time until/since closest study visit, age and gender. The ethics committees of Royal Prince Alfred Hospital, Camperdown and The Alfred Hospital, Melbourne approved the study and all patients provided written informed consent.
{kind=link}
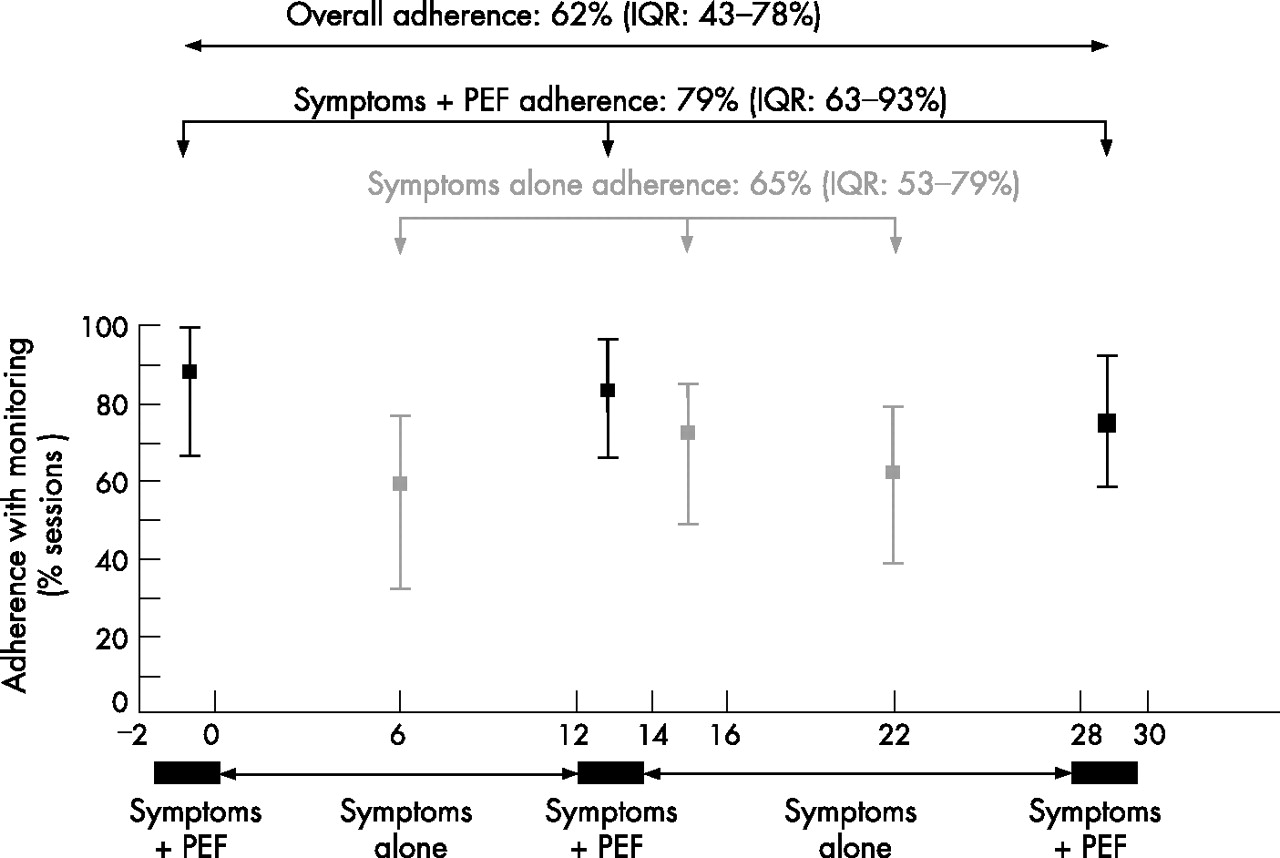
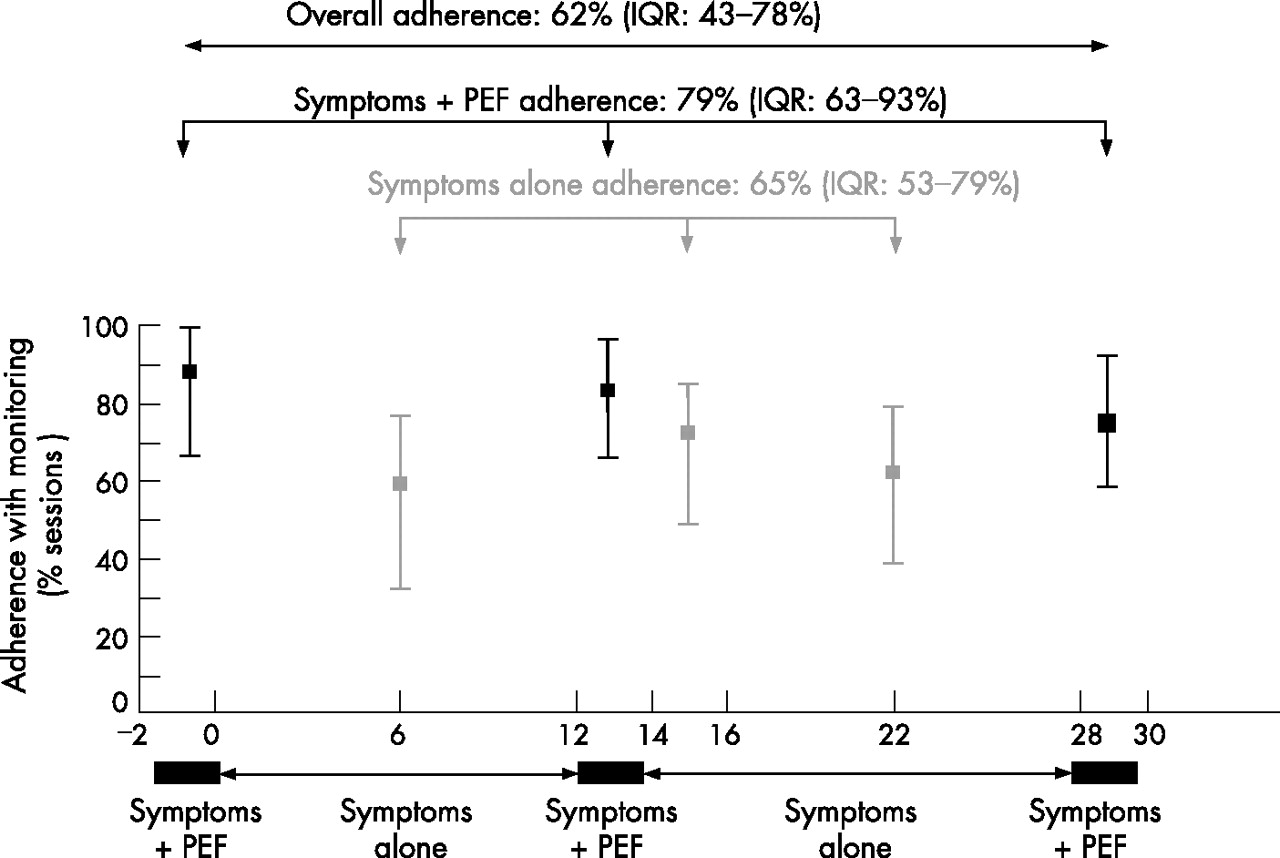
Adherence with symptom and peak expiratory flow (PEF) monitoring. Adherence was assessed as the percentage of scheduled twice daily “diary sessions” (symptoms with or without PEF) completed, with a maximum of two sessions/day evaluated. Median values and interquartile range (IQR) for adherence during each period are shown.
Figure 1 shows that adherence to monitoring was higher during PEF periods than non-PEF periods (79% vs. 65%, p<0.0001). Mixed model analysis showed that weekly adherence with monitoring increased by 13% with PEF monitoring (p<0.0001) and by 5% with each 10 years of increasing age (p<0.0001). There was no effect of gender (p = 0.80) or time to next/last visit (p = 0.59).
In contrast with the perception that PEF monitoring is burdensome to patients, this analysis showed that, with electronic diaries, asking adults to measure PEF significantly improved their adherence with monitoring. While a randomised study would be required to formally evaluate the impact of PEF measurement on adherence with monitoring, this is the first study to assess differences in adherence with monitoring with and without PEF. We used subjects as their own controls as they crossed over between periods.
We have previously reported good adherence with long-term electronic monitoring of symptom and PEF data, when PEF data were closely incorporated into asthma management.4 In the present study, good adherence was also achieved with similar electronic devices, despite the routine nature of the monitoring for assessment of study outcome variables and the absence of physician feedback to subjects.
Adherence represents a balance between burden and benefit, both real and perceived. Although electronic devices can reduce the burden of monitoring in asthma,4 patients may perceive little personal benefit from recording how they feel (symptom monitoring). By contrast, PEF monitoring provides patients with objective information, complementary to their subjective experience.1 Such personal feedback may act as an incentive, improving adherence with monitoring, even if the PEF data are not—as in previous electronic monitoring studies—interpreted by a clinician4 or displayed on-screen as a time-trend analysis.5
Self-monitoring is a cornerstone of chronic disease management and clinical trial design by providing data about patients’ day-to-day status that is not captured by interval assessments. Although patients who agree to participate in clinical trials are likely, by nature, to be more adherent than those in clinical practice, plans for monitoring in either setting should incorporate strategies which enhance adherence and preclude retrospective completion, and hence improve the validity and utility of self-recorded data. The present findings show that the provision of feedback to patients, such as by PEF measurement, may improve rather than hamper adherence with monitoring, provided the burden of monitoring is minimised by use of patient-friendly electronic devices.
Footnotes
-
This study was conducted under the auspices of the Cooperative Research Centre for Asthma, jointly funded by the Australian Federal Government and industry including AstraZeneca, Aventis Pharma, and GlaxoSmithKline. HKR was funded by the Asthma Foundation of New South Wales. CAS was funded by the Australian Government Department of Education, Science and Training via an Australian Postgraduate Award.
-
Competing interests: None.
-
The clinical trial from which these data were obtained was completed in August 2004 and was therefore not required to be registered in a clinical trial registry.
The study of adherence was initiated by HKR. EGB and CAS conducted data analysis with input from Wei Xuan and HKR. CAS and HKR co-wrote the manuscript. The clinical trial protocol was developed by Christine R Jenkins and HKR and was carried out by CAS, HKR, Karen Symons, Susan Forrest-Blythe, Caroline Reddel, Frank Thien and Ciça Santos, with input from Carol Armour and Sinthia Bosnic-Anticevich.