Article Text

Statistics from Altmetric.com
- BOS, bronchiolitis obliterans syndrome
- COPD, chronic obstructive pulmonary disease
- FEV1, forced expiratory volume in 1 second
- FVC, forced vital capacity
- IIP, idiopathic interstitial pneumonia
- IPF, idiopathic pulmonary fibrosis
- NSIP,
- non-specific interstitial pneumonia,
- TLC, total lung capacity
- Tlco, carbon monoxide lung transfer factor
- UIP, usual interstitial pneumonia
Application of a classification based on simple lung function testing in IPF
For many years the idiopathic pulmonary fibrosis (IPF) community has debated the merits of the histopathological classification of idiopathic interstitial pneumonia (IIP).1 The ATS/ERS consensus statement identifies the importance of histological categories of usual interstitial pneumonia (UIP) and non-specific interstitial pneumonia (NSIP). Furthermore, it emphasises that IPF is the clinical correlate of UIP. Despite the recognition of the importance of histological characterisation, surgical biopsy rates vary considerably.2 Most clinicians do not subject their patients to surgical biopsy, despite the potential prognostic benefit of detailed histological evaluation, because many patients are elderly and have significantly impaired lung function and other medical co-morbidities resulting in a potentially high mortality rate.3 In addition, HRCT scanning provides diagnostic data of high sensitivity and specificity for the diagnosis of IPF with acceptable interobserver variability.4,5
Meanwhile, the chronic obstructive pulmonary disease (COPD) and lung transplantation communities have applied simple but pragmatically useful classifications. Bronchiolitis obliterans syndrome (BOS), for example, has been subject to a clinical grading system reflecting the degree of impairment of lung function following lung transplantation. The emergence of a classification based on simple lung function testing occurred because of the difficulties in obtaining adequate tissue for the diagnosis of obliterative bronchiolitis. This is comparable to the situation in IPF where tissue is also difficult to obtain. The success of the classification of BOS is reflected by the publication of an updated version.6
The global initiative for COPD (GOLD) is another example of a consensus classification based on simple lung function testing. GOLD provides a staging system ranging from an “at risk” category to a severe disease category.7 Based on simple lung function testing, it is reproducible and has facilitated the identification of patients with COPD. Furthermore, it has enabled worldwide harmonisation of clinical and experimental research studies in COPD.7
Recent publications relating to lung function, focusing specifically on IPF, provide a similar opportunity. The histological classification proposed by Katzenstein and endorsed by the ATS/ERS consensus statement potentially allows for the development of a staging system based on simple and widely available evaluation techniques. The aim of such a classification would not be to supersede the histological classification but rather to build upon it.
The aim of this review is therefore to discuss the potential of a grading system for IPF based solely on simple static lung function studies. For judging disease severity we sought a parameter that identified patients with impaired survival, defined as less than 2 years. For judging disease progression we sought lung function changes which identified patients at increased risk of mortality.
HISTOLOGICAL CLASSIFICATION AND LUNG FUNCTION
The absence of broad agreement on the interpretation of lung function testing in IPF reflects the variability in published data on the subject (table 1).8 Impaired survival has been associated with a variety of findings including no relationship with lung function,9 increased ratio of forced expiratory volume in 1 second to forced vital capacity (FEV1/FVC ratio),10 reduced total lung capacity (TLC),11,12 and change in FVC/carbon monoxide transfer factor (Tlco) after 1 year (table 1).13 Formerly a critical confounding factor influencing the interpretation of lung function was the failure to distinguish between histological subsets in IIP.14,15 Consequently, early published data on lung function have been limited by the absence of focus on specific histological subgroups. Recent publications have therefore focused on lung function data specifically in the context of UIP and NSIP, allowing a consistent theme to emerge (table 1). A PubMed literature search was performed to identify peer reviewed manuscripts relating to lung function testing in IPF published in 1998–2004. This period was chosen because it reflects the clinical impact of the characterisation of patients based on histological subsets as described by Katzenstein et al in 1998.14
Summary of lung function studies in IPF
LUNG FUNCTION AND DISEASE SEVERITY
A global view of historical lung function data emphasises that a poor outcome is associated with “low” lung function. Schwartz et al12 highlighted the fact that reduced lung function was associated with limited survival. In a study of 74 individuals who had undergone lung biopsy, univariate analysis showed that there was a greater hazard of death with lower % predicted FVC and lower % predicted Tlco. However, clinicians require a specific threshold in the context of disease severity.16 The study by Gay et al17 emerged as a key publication in the context of the methodology used for appraising the influence of lung function. In contrast to historical studies which reported group differences in survival and hazard ratios, they applied for the first time receiver operator characteristic (ROC) curve estimates. ROC state the probability that a diagnostic criterion selects a disease subject correctly rather than a non-disease subject.18 In the context of lung function, ROC curves express the ability of a variable to discriminate between death and/or survival. However, despite the application of ROC analysis by Gay et al, no lung function variable identified risk of death (table 1). This is likely to reflect the efforts to study well characterised patients, resulting in a relatively small number of subjects in the study.
DISEASE SEVERITY: ADVANCED AND LIMITED DISEASE
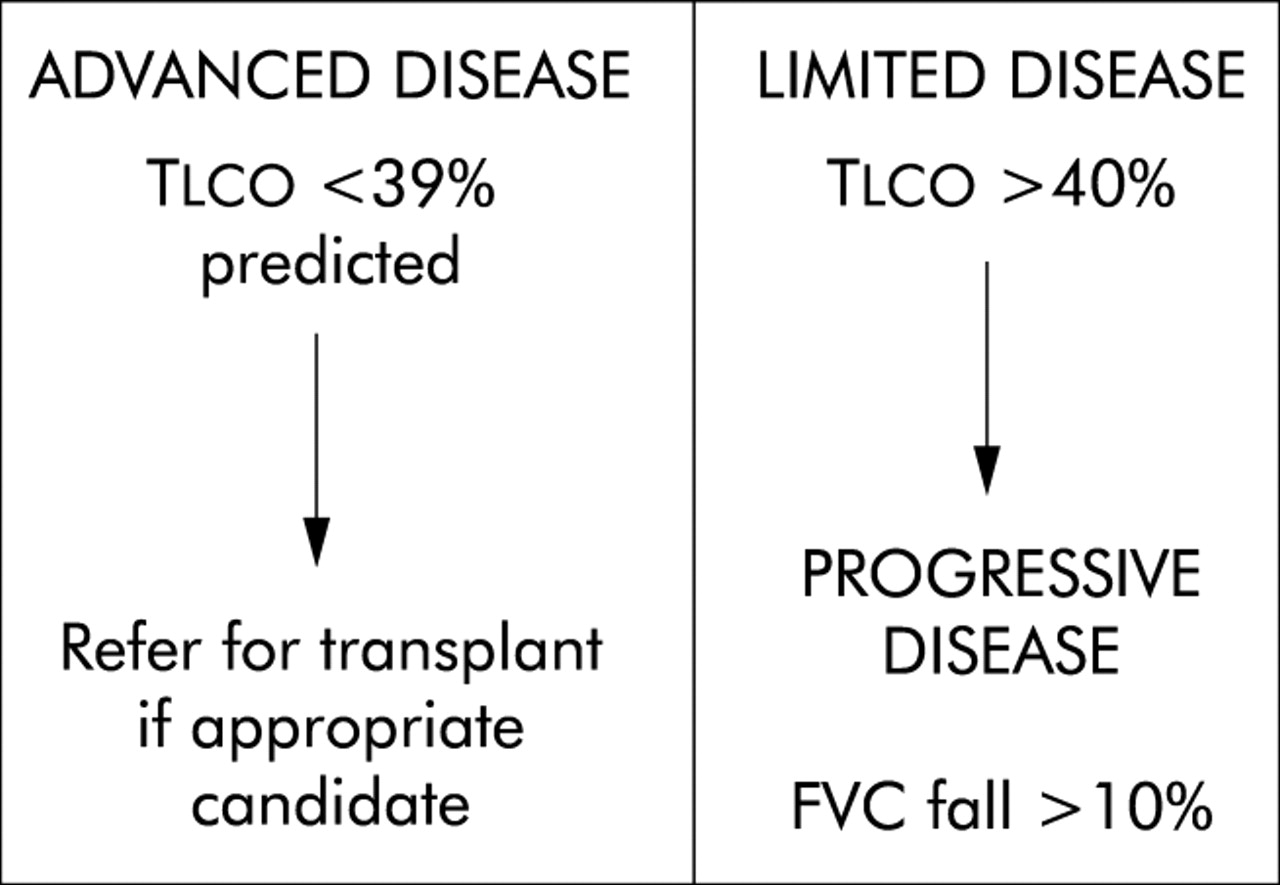
Acknowledging the need for a specific threshold value for estimating disease severity, recent data suggest that severity of disease can be categorised as advanced or limited disease on the basis of lung function. Extending the study by Gay et al by using ROC analysis, Mogulkoc et al19 focused on lung function in the context of transplant referral. This study targeted a well characterised group of 115 patients with IPF aged 45–65 years. A total of 12 variables influencing survival were significant on univariate regression analysis. A multivariate stepwise regression analysis identified only % predicted Tlco and HRCT fibrosis as independent predictors of 2 year survival. ROC analysis of % predicted Tlco gave an area of 0.8 (CI 0.7 to 0.9) and HRCT fibrosis score gave an area of 0.86 (CI 0.77 to 0.95). It was shown that a gas transfer factor of <39% of predicted combined with HRCT scores had an 80% sensitivity and specificity for predicting death within 2 years. This allowed the observation of a simple measure of Tlco to be associated with a specific limited time frame of survival. Identification of a threshold value associated with increased mortality serves as the basis for a distinction between advanced and limited disease (fig 1).

{kind=link}
A classification of IPF based on simple lung function criteria. Tlco, carbon monoxide transfer factor; FVC, forced vital capacity.
The concept of advanced IPF was corroborated by the work of Latsi et al.20 In a retrospective study of 104 patients with a histologically confirmed diagnosis, determinants of early mortality at presentation and mortality after 6 months of follow up were studied. In patients dying within 2 years of presentation, the median Tlco was 39% of the predicted value. These authors present patients with advanced disease as an “early mortality” group in whom physiology was the best determinant of survival. A key observation in this study is that a subgroup of patients with severely reduced Tlco, defined as <35% of predicted, had a survival time of less than 2 years irrespective of whether they had UIP or NSIP. Those with a Tlco of >35% of predicted had a 65% survival at 3 years. This emphasises that, once a certain threshold of physiological impairment is reached, mortality is increased.
As lung function is the primary investigation performed by pulmonologists, patients may therefore be defined as having advanced disease (Tlco <39% of predicted), allowing the potential identification of patients with poor early survival. Although FVC is predictive of survival in univariate modelling, it does not maintain its effect in multivariate analysis.21 The severity of IPF is therefore best graded by Tlco estimation. For patients with limited disease (Tlco >40% of predicted), longer survival is more likely. It is in this latter group that serial lung function studies have particular prognostic value.
LUNG FUNCTION AND DISEASE PROGRESSION
ROC curve analysis highlights the fact that Tlco is superior to FVC for evaluating disease severity.19 In contrast, a change in FVC may be the most reliable simple lung function variable to highlight disease progression. When appraising lung function studies of disease progression in IPF, three points deserve consideration: the coefficient of variation of the test, the baseline from which the change occurs, and the time scale used to determine change.
The intertest variation has been widely studied. A 10% change in FVC is required accurately to reflect a change in vital capacity. Using Tlco requires a change of 15% or more. Consequently, the baseline from which change occurs is vital to observe. Because many patients with IPF present with a Tlco of <39% of predicted, a further 15% fall from baseline is difficult to document. Individuals require adequate pulmonary reserve to exhibit a change in that parameter. Inadequate reserve may explain why a significant proportion of patients fail to show evidence of lung function progression. Patients with limited disease or adequate pulmonary reserve therefore lend themselves to evaluation of disease progression.
The time required to observe a change in lung function is also critical. As the mean survival of some groups of patients may be as low as 2.5 years, a prolonged period of observation of, for example, 1 year biases a study towards patients with favourable survival and limited disease. Hanson et al13 were the first to study the change in lung function over 1 year. They studied 58 patients and evaluated the influence of a 10% change in FVC and a 20% change in Tlco. This cohort had favourable characteristics including a mean age of 55 years and a mean survival of 88 months. The mean survival of patients exhibiting a change (24% of the total) in FVC was 2.5 years. The mean survival of patients exhibiting a change was also 2.5 years in Tlco (22% of the total.)
Acknowledging this, two recent publications progress the strategy described by Hanson et al.13 Firstly, Collard et al,22 in a study of 81 patients with UIP, evaluated change in lung function over both 6 and 12 months. The median survival of the patients subject to 6 month evaluation was 4.8 years and 6.2 years for those studied at 12 months. The mean Tlco of the group was 52% of predicted. Changes in TLC % predicted, FVC % predicted, and Tlco % predicted over 6 months predicted survival. Of these, the change in FVC % predicted was the best predictor. Flaherty et al21 studied 109 patients, 80 of whom had UIP and 29 had NSIP. The mean Tlco of the group was 50% of predicted. 32% of patients had a fall of >10% in FVC and 49% of patients remained within 10% of baseline. On multivariate analysis, controlling for histological subgroups and baseline lung function, a change in FVC over 6 months was an independent risk factor for mortality. Both studies included patients with preserved Tlco in the region of 50% of predicted.21,22
Changes in Tlco are an alternative measure of disease progression. Latsi et al20 observed a higher mortality in patients with a decline in Tlco at 6 and 12 months, whether trends were quantified numerically or categorically. However, repeat Tlco measurements can be difficult to standardise, explaining the need for a greater change in Tlco than in FVC in order to categorise deterioration. In the study by Latsi et al, serial Tlco trends had only a minimal prognostic advantage over serial FVC trends and the analysis included a significant subset of patients with advanced disease. In the recently published interferon gamma-1b treatment study only 14% of 300 patients with a mean Tlco of 37% were defined as having disease progression based on a 15% change in Tlco (Bill Bradford, personal communication).23
Therefore the authors favour classification of disease progression based on change in FVC at 6 months rather than 1 year because this allows the early identification of progressive disease. However, in patients with limited disease the potential value remains of re-evaluating progression at 1 year, as demonstrated by Flaherty and Latsi.20,21 Re-evaluation at 12 months may be particularly important in the context of a “marginal” decline in FVC of 5–10%, which may reflect either measurement variation or genuine disease progression. Thus, the definition of disease progression using change over 6 months should not obscure the need to refine prognostic evaluation at 1 year and at least 6 monthly intervals thereafter.
BENEFITS AND DISADVANTAGES OF A CLASSIFICATION
The potential benefits of a classification based on lung function are substantial. There is a critical need for a classification based on lung function for a condition in which it is difficult to acquire tissue. It would standardise nomenclature and facilitate entry into emerging treatment studies. It may also optimise referral for lung transplantation. A limited window of opportunity exists to refer IPF patients for lung transplantation. The short transplant window is reflected by the high mortality rate in patients with IPF awaiting lung transplantation.24 The proposed classification, particularly based on the concept of advanced disease, may facilitate more accurate referral, the time of listing being determined by local organ availability.
Although a tentative and provocative first step, there are potential limitations to the proposed classification. It must be acknowledged that the data presented by Mogulkoc and Latsi are retrospective and should ideally be validated by a prospective evaluation. Furthermore, Thabut and Fournier25 emphasise weaknesses with reference to the definition of disease progression based on a 10% change in FVC. For instance, a change in FVC from 90% predicted to 80% predicted is not clinically comparable to a change from 60% to 50%. There is also an inherent difference between group data and the individual patient. Although group data show that 46% of patients who exhibit a 10% fall may survive 5 years, this does not equate with an individual patient having a 46% chance of surviving 5 years.
It must also be recognised while monitoring disease progression that only a proportion of patients may exhibit a change in lung function. In the study by Flaherty et al, 32% of patients had a fall of >10% in FVC while 49% of patients remained within 10% of baseline.21 In the interferon gamma-1b treatment study, 25% of patients were defined as having disease progression based on a change in FVC.23 To address this, specialist centres have developed composite indices containing a mixture of parameters, with and without imaging data.26,27 Preliminary analysis suggests that such scoring systems may be more accurate prognostically than individual lung function variables. However, these scoring systems may not be easily applicable to the broader community of non-specialist centres, especially when exercise testing and radiographic profusion scores are included. The focus should therefore be firstly to emphasise the need for staging based on lung function tests. Although a lung function classification is a first step, in the future HRCT data and simple field exercise tests such as the 6 minute walk test may provide complementary data.28,29 The proposed lung function schema provides a trigger for discussion and a framework from which additional simple and pragmatic markers of progressive disease can be identified.
Acknowledgments
The authors acknowledge the Irish Lung Fibrosis Association, the University of Michigan Fibrotic Lung Disease Network, and the Brompton Interstitial Lung Disease Group.
Application of a classification based on simple lung function testing in IPF
REFERENCES
Footnotes
-
Conflict of interest: none