Article Text

Statistics from Altmetric.com
Many carefully crafted studies with different end points have shown significant benefits with non-invasive ventilation (NIV) over and above conventional medical treatment alone in the management of hypercapnic exacerbations of chronic obstructive pulmonary disease (COPD).1 However, most data have evaluated highly selected patients within stringent realms of randomised controlled trials. Since strict criteria need to be fulfilled before clinical trial entry (often excluding elderly patients and those with major co-morbidities, electrolyte disturbance and severe exacerbations), outcomes may not be reflective of everyday practice. We wished to highlight demographics, physiological variables, outcomes and 1-year survival in a large cohort of patients receiving ward-based NIV for hypercapnic exacerbations of COPD.
Data were gathered retrospectively from a password-protected database for all patients commenced on ward-based NIV for respiratory failure. All individuals had been admitted to the respiratory unit in Aberdeen Royal Infirmary (a large teaching hospital in the north-east of Scotland) between January 2006 and June 2009 inclusive and had been assessed by a middle grade respiratory physician or above regarding suitability for NIV. In all patients, appropriate pharmacological treatment was initiated and NIV pressures were titrated upwards as tolerated.
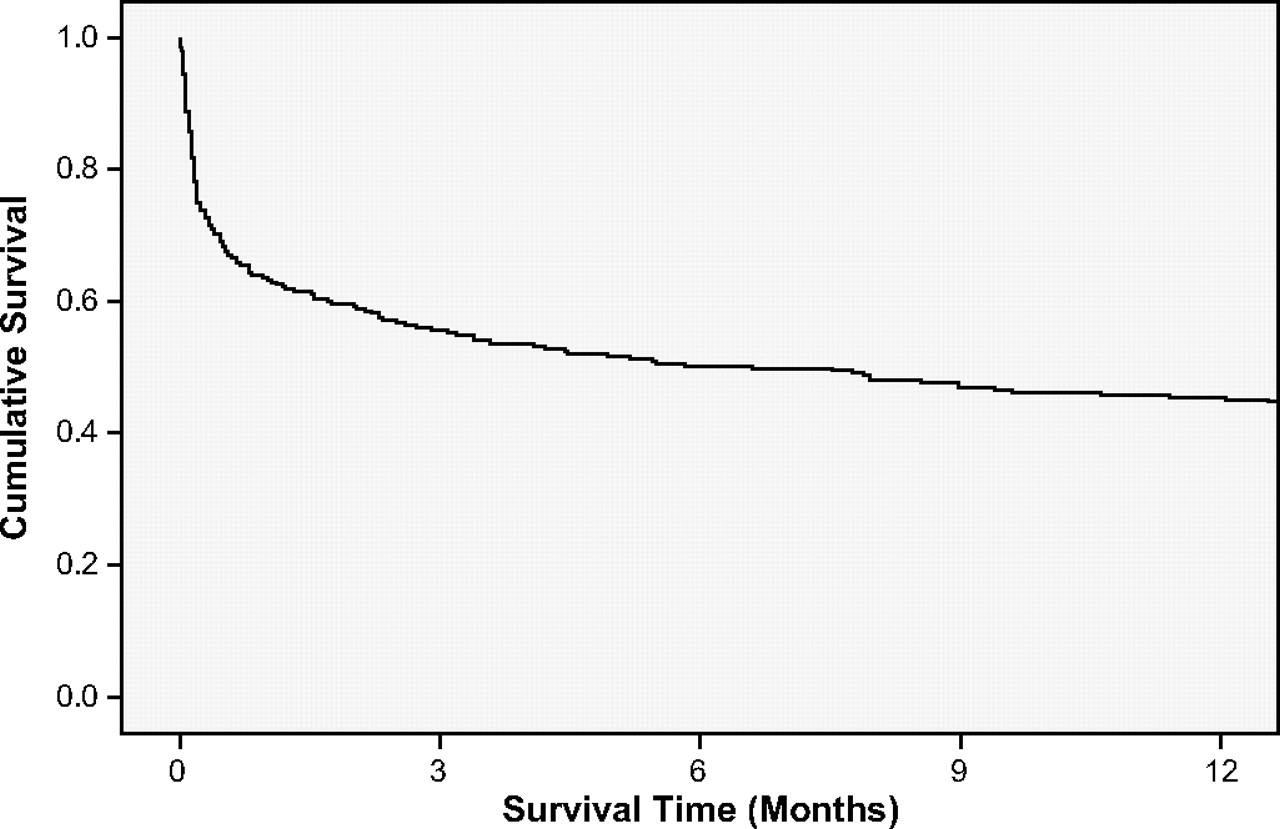
Over a 3.5-year period, 275 separate patients (158 females (57%) with mean age 71 years) received NIV with a mean baseline pH and Pco2 of 7.24 and 10.23 kPa, respectively. Of the 275 patients, 89 (32%) died in hospital (5 of these failed to tolerate NIV and were not considered candidates for intensive care), 174 (63 %) were discharged home and 12 (5%) were transferred to intensive care after failing treatment with NIV. No patients received domiciliary NIV following hospital discharge. Of those discharged, cumulative all-cause mortality after 3, 6, 9 and 12 months was 44%, 50%, 52% and 55%, respectively (figure 1).

{kind=link}
Kaplan–Meier curve showing cumulative survival over 12 months in patients who received non-invasive ventilation for a hypercapnic exacerbation of chronic obstructive pulmonary disease.
These real-life data indicate that in unselected patients with hypercapnic exacerbations of COPD who require NIV, almost two-thirds survive to hospital discharge. As expected, our inpatient mortality was greater than that reported in randomised controlled trials. For example, in one study (n=236 randomised individuals), the inpatient mortality in NIV-treated individuals (n=118) was 10% versus 20% in those receiving usual medical care (p=0.05).2 In another study (n=85 randomised individuals), the inpatient mortality was 9% in those receiving NIV versus 29% in the control group (p<0.05).3 In these studies, the mean pH (7.32 and 7.27, respectively) was greater than the pH in our study (7.24). There is a paucity of published data regarding long-term survival of patients discharged from hospital following treatment with NIV. We have shown that the all-cause mortality rate was as high as 44% within the first 3 months of hospital discharge, although this figure only rose by a further 11% over the subsequent 9 months. This suggests that further studies are required to identify clinical features associated with death within 3 months of hospital discharge. All patients discharged after receiving NIV should be established on optimal pharmacological treatment and considered for interventions such as early pulmonary rehabilitation.4 The role of domiciliary NIV in this patient group also needs further evaluation.5
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.